All published articles of this journal are available on ScienceDirect.

Anatomical Evaluation of Mandibular Premolars in Saudi Population: An In Vivo Cone-beam Computed Tomography Study
Authors Info & Affiliations
Abstract
Background:
Cone-beam computed tomography (CBCT) offers a three-dimensional (3D) image of the anatomical structures in the maxillofacial region. CBCT can provide images with sufficient spatial resolution and low radiation dose in endodontic diagnosis and treatment planning.
Objective:
This study aimed to evaluate the root canal morphology of mandibular premolars in a Saudi sub-population by showing the importance of cone-beam computed tomography radiographic analysis in detecting varieties of the root canal system.
Methods:
A total of 776 mandibular first and second premolars were analyzed. Teeth that have completed root development and apical closure were included. To accurately evaluate the external and internal morphologies of the teeth, three sections (i.e., the serial axial, coronal, and sagittal sections) were acquired for each tooth. Data are presented in terms of frequencies and percentages. The chi-squared test was used to determine the differences between two sides (right and left). A p-value of less than 0.05 was considered statistically significant.
Results:
Among the 397 mandibular first premolars, 99.5% had one root, 69.5% had one canal, and 29.5% had two canals. In terms of root canal configuration, 69.5%, 6.3%, 22.2%, and 0.3% of the teeth had Vertucci type I, type III, type V, and type VII canal configurations, respectively. Similarly, among the mandibular second premolars, 100% had one root, 96.8% had one canal, and 2.1% of teeth had two canals. Most of the samples (96.8%) had Vertucci type I canal configuration, and 1.6% and 0.8% of the teeth had Vertucci type III and type V canal configurations, respectively. In both groups of teeth, no statistically significant differences were observed between the right and left sides (P> 0.05).
Conclusion:
Mandibular premolars could have challenged internal morphology, and CBCT small field of view is advised in case periapical x-ray is inconclusive.
1. INTRODUCTION
Precise and assertive treatment strategy is an indispensable part of root canal therapy. Diagnostic imaging assists clinicians in envisioning the dental anatomy in zones that cannot be viewed clinically. Periapical radiographs (PAs) have been considered the best diagnostic tool and thus help dentists detect the pathology and clinicians develop a treatment plan [1]. Cone-beam computed tomography (CBCT) offers a three-dimensional (3D) image of the anatomical structures in the maxillofacial region. CBCT can provide images at a low radiation dose and sufficient spatial resolution for use in the endodontic diagnosis, planning the treatment strategy, and detecting endodontic pathology [2, 3]. Moreover, CBCT overcomes most of the shortcomings of traditional radiography, such as the 3D evaluation of root canals and the surrounding anatomy [4]. Although PA is the imaging modality of choice for endodontic patients, the limited field of view of CBCT should be considered in the initial treatment of teeth with potential extra canals and suspected complex morphology and dental anomalies [5].
The 3D view of the root canal morphology of teeth is necessary during root canal therapy for preventing missed canals and other endodontic mishaps [6]. Mandibular premolars show many anatomical variations in the number of root canals and root canal configurations, which cannot be detected in two-dimensional (2D) radiographs and orthopantomography. Internal morphology may present as fine ribbon-like canals [7] and C-shaped canals [8], which make adequate chemo-mechanical cleaning and shaping and obturation challenging for operators. Many studies evaluated mandibular first and second mandibular premolars and reported; one canal in 69.3–86%, two canals in 14–25.5% [9-12], and three canals in 0.5% [9], and 0.4% [10] in the first premolars. While second premolar teeth, studies showed the number of root canals was one in 97.5% and two in 2.5% of the teeth studied [10], and the incidence of three root canals ranged from 0 to 0.4% [9, 10].
Age, gender, and ethnicity could be responsible for these variations [13]. Root canal morphology can have marked racial prediction, thus requiring understanding the root canal anatomies of people from various ethnic backgrounds [14]. A wide range of reviews on the root canal anatomy of Saudi Arabians featured only two studies on mandibular premolars; one utilized in vivo CBCT and the other in vitro CBCT using staining on the first mandibular premolar [15-17].
Thus, this research aims to evaluate the root canal morphology of mandibular premolars based on the number of roots in the tooth, the number of canals in the roots, and the canal configurations according to Vertucci’s classification in the Saudi sub-population using in vivo CBCT. Such an investigation seems helpful to add to the body of knowledge for Saudi ethnicity. The null hypothesis was that there is no difference in the anatomy of mandibular premolars of a Saudi population in the southern region compared to other national and international studies.
2. MATERIALS AND METHODS
The database archive of the College of Dentistry of Jazan University was searched for CBCT radiographs from 2016 to 2017. A total of 208 CBCT radiographs were retrieved. These radiographs belonged to 100 males and 108 females from 17 to 59 years of age livingin Jazan City, Southern region of Saudi Arabia. Prior to the study, ethical approval from the Scientific Research-College of Dentistry, Jazan University (Ref#: CODJU-1922F) was obtained. No consent form was required from the patients because all CBCTs were retrieved retrospectively from the archive of the College of Dentistry. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2013. The CBCT machine used in this study was (3D Accuitomo 170 Morita; Osaka, Japan) with the following parameters: 5–8 mA, 90 Kv, exposure time of 17.5 s, and voxel size of 0.25 mm. A software imaging program (Morita’s i‐Dixel 3D) was used to process the CBCT radiographs. A total of 776 mandibular first and second premolars (397 first and 379 second premolars) were analyzed in the present study.
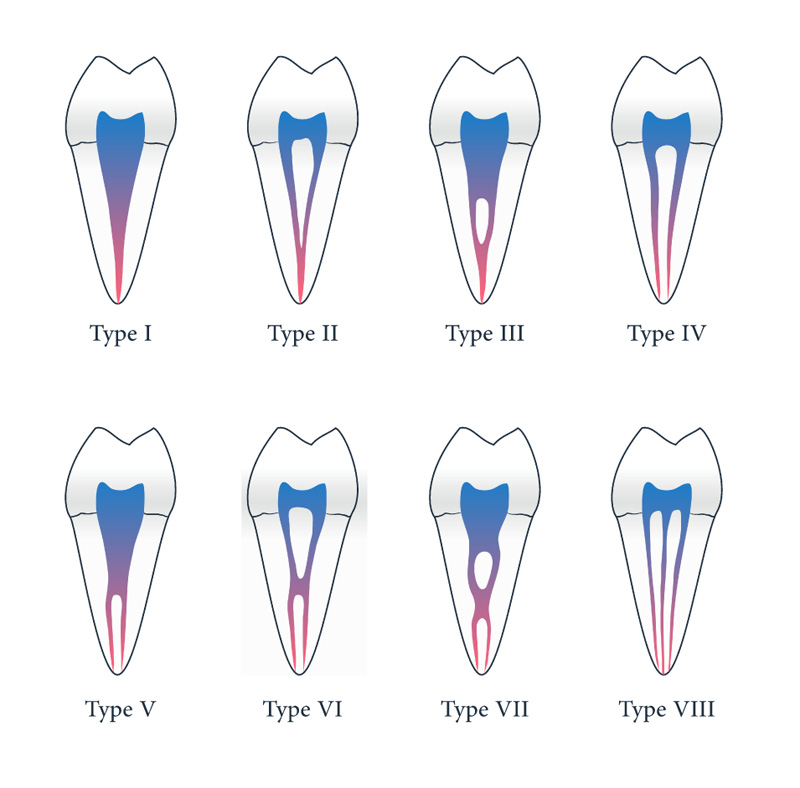
The inclusion criteria were teeth with fully developed roots, closed apices, and patients of Saudi Arabian origin who generally have the same ethnic background. The exclusion criteria were teeth with root canal treatment, calcified canals, and resorbed roots. Teeth with distorted or unclear CBCT radiographs were also excluded. To accurately evaluate the external and internal morphologies of the teeth, three sections (i.e., the serial axial, coronal, and sagittal sections) were acquired for each tooth. The following parameters were evaluated: the number of roots, the number of canals, and the root canal configurations according to Vertucci’s classification [18] (Fig. 1). The comparison of these parameters between the right and left sides was also considered.
For reliable measurements, one observer evaluated 25% of the total sample twice with an interval period of three weeks. The results of Cohen’s Kappa test revealed a nearly perfect intra-examiner agreement between observations with a value of 87.5% and an asymptotic standard error of ±9.2%.
2.1. Statistical Analysis
The data were analyzed using statistical software (SPSS V25; IBM, Chicago, IL). Descriptive statistics were presented in terms of frequencies and percentages. The Chi-squared test was used to determine the differences between both sides (right and left). The contingency coefficient option was selected for more than two categories, and a p-value of less than 0.05 was considered significant.
3. RESULTS
3.1. Mandibular First Premolars
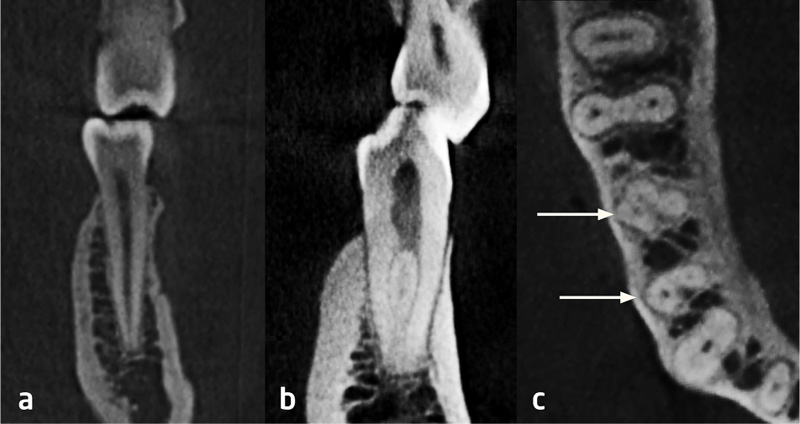
Among the evaluated teeth, 397 were mandibular first premolars. Out of the 397 mandibular first premolars, 395 (99.5%) had one root and only 2 (0.5%) teeth had two roots. More than two-thirds of the sample (69.5%) had one canal, 117 (29.5%) had two canals, and only 4 (1.0%) teeth had three canals (Fig. 2). Meanwhile, 276 (69.5%), 25 (6.3%), 88 (22.2%), and 1 (0.3%) teeth had Vertucci type I, Vertucci type III, Vertucci type V, and Vertucci type VII canal configurations, respectively, and 7 (1.8%) teeth had a different type of root canal configuration (Table 1).
Table 2 shows the comparison between the right and left sides. All the mandibular first premolars (100.0%) in the left side had one root, while 99.0% (n = 196) of the teeth on the right side had one root and 1.0% (n = 2) had two roots, with no significant difference (P = 0.248) between the two sides. Similarly, no significant difference was found (P = 0.843) between the two sides in terms of the number of canals. Only two teeth on each side had three canals, while the rest had one canal. Most of the teeth in both right and left sides, with no significant difference, had a Vertucci type I or V canal configuration, and few were found with a Vertucci type III or VII canal configuration. Five teeth on the right side and two teeth on the left side had other types of root canal configuration.
| Frequency | Percent | ||
|---|---|---|---|
| Number of roots (N= 397) | |||
| 1 root | 395 | 99.5 | |
| 2 roots | 2 | 0.5 | |
| Number of canals (N= 397) | |||
| 1 canal | 276 | 69.5 | |
| 2 canals | 117 | 29.5 | |
| 3 canals | 4 | 1.0 | |
| Vertucci types (N= 397) | |||
| Type I | 276 | 69.5 | |
| Type III | 25 | 6.3 | |
| Type V | 88 | 22.2 | |
| Type VII | 1 | 0.3 | |
| Other | 7 | 1.8 | |
| Right | Left | P | ||
|---|---|---|---|---|
| Number of roots (N= 397) | ||||
| 1 root | 196 (99.0) | 199 (100.0) | 0.248 | |
| 2 roots | 2 (1.0) | 0 (0.0) | ||
| Total | 198 (49.9) | 199 (50.1) | ||
| Number of canals (N= 397) | ||||
| 1 canal | 135 (68.2) | 141 (70.9) | 0.843 | |
| 2 canals | 61 (30.8) | 56 (28.1) | ||
| 3 canals | 2 (1.0) | 2 (1.0) | ||
| Total | 198 (49.9) | 199 (50.1) | ||
| Vertucci types (N= 397) | ||||
| Type I | 135 (68.2) | 141 (70.9) | 0.795 | |
| Type III | 12 (6.1) | 13 (6.5) | ||
| Type V | 45 (22.7) | 43 (21.6) | ||
| Type VII | 1 (0.5) | 0 (0.0) | ||
| Other | 5 (2.5) | 2 (1.0) | ||
| Total | 198 (49.9) | 199 (50.1) | ||
3.2. Mandibular Second Premolars
Three hundred and seventy-nine mandibular second premolars were evaluated. All teeth (100%) had one root. Among them, 367 (96.8%) teeth had one canal, 8 (2.1%) teeth had two canals, and 4 (1.1%) teeth had three canals. Most of the sample teeth (96.8%) had Vertucci type I, and 6 (1.6%), 3 (0.8%), and 3 (0.8%) teeth had Vertucci type III, Vertucci type V, and different types of root canal configuration, respectively (Table 3).
All teeth (100.0%) on both sides had one root. More than 90% of the teeth on both sides had one canal, and only 2 teeth on each side had three canals. However, no significant difference was found between the two sides (P = 0.753). Similarly, no significant difference (P = 0.865) was found between the right and left sides in terms of root canal configuration. More than 90% and 1.6% of the teeth on both sides had Vertucci type I and Vertucci type III canal configurations, respectively (Table 4).
| Frequency | Percent | ||
|---|---|---|---|
| Number of roots (N= 379) | |||
| 1 root | 379 | 100.0 | |
| Number of canals (N= 379) | |||
| 1 canal | 367 | 96.8 | |
| 2 canals | 8 | 2.1 | |
| 3 canals | 4 | 1.1 | |
| Vertucci types (N= 379) | |||
| Type I | 367 | 96.8 | |
| Type III | 6 | 1.6 | |
| Type V | 3 | 0.8 | |
| Other | 3 | 0.8 | |
| Right | Left | P | ||
|---|---|---|---|---|
| Number of roots (N= 379) | ||||
| 1 root | 187 (100.0) | 192 (100.0) | NC | |
| Total | 187 (49.3) | 192 (50.7) | ||
| Number of canals (N= 379) | ||||
| 1 canal | 180 (96.3) | 187 (97.4) | 0.753 | |
| 2 canals | 5 (2.7) | 3 (1.6) | ||
| 3 canals | 2 (1.1) | 2 (1.0) | ||
| Total | 187 (49.3) | 192 (50.7) | ||
| Vertucci types (N= 379) | ||||
| Type I | 180 (96.3) | 187 (97.4) | 0.865 | |
| Type III | 3 (1.6) | 3 (1.6) | ||
| Type V | 2 (1.1) | 1 (0.5) | ||
| Other | 2 (1.1) | 1 (0.5) | ||
| Total | 187 (49.3) | 192 (50.7) | ||
| Mandibular First Premolar | Mandibular Second Premolar | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Name of Researcher and Year |
Number of Canals | Vertucci’s Canal Configuration | Number of Canals | Vertucci’s Canal Configuration | |||||||||||||||||||
| 1 | 2 | 3 | I | II | III | IV | V | VI | VII | VIII | 1 | 2 | 3 | I | II | III | IV | V | VI | VII | VIII | ||
| Alfawaz et al. – 2019 [16] | 96.4% | 3.1% | 0.5% | 88% | 3.6% | 3.1% | 12% | 1.5% | - | - | 1.5% | 95.6% | 3.8% | 0.6% | 90.1% | 4.4% | 0.3% | 2.6% | 0.9% | - | - | 1.7% | |
| Jang et al. -2019 [17] | 78.7% | 10.3% | - | 78.8% | 2.27% | 3.19% | 0.4% | 10.9% | - | - | - | 98.4% | 1.6% | - | 98.4% | 1.4% | 0.2% | - | - | - | - | - | |
| ZareJahromi et al. – 2018 [15] | 89.47% | 10.1% | - | - | - | - | - | - | - | - | - | 97.3% | 2.19% | - | - | - | - | - | - | - | - | - | |
| Vyoma et al. - 2016 [18] | L | 98% | 2% | - | 94.5% | 1% | 2% | - | 1.5% | - | - | 1% | 100% | - | - | 95% | 0.5% | 2% | 0.5% | 1% | - | - | - |
| R | 96% | 4% | - | 99% | 1% | - | |||||||||||||||||
| Llena et al. - 2014 [20] | L | 82.4% | 6% | - | 78.1% | 8.2% | - | - | 12.3% | 1.3% | - | - | 82% | 17.8% | - | 90.6% | 1.8% | - | - | 7.5% | - | - | - |
| R | 74,4% | 23.1% | 2.6% | 94.4% | 5.6% | - | |||||||||||||||||
| Chourasia et al. 2017 [19] | 72% | 26% | 2% | 69% | - | 8% | 4% | 16% | - | - | 2% | - | - | - | - | - | - | - | - | - | - | - | |
| Present study | L | 70.9% | 28.1% | 1% | 70.9% | - | 6.5% | - | 21.6% | - | - | 2% | 97.4% | 1.6% | 1% | 97.4% | - | 1.6% | - | 0.5% | - | - | 0.5% |
| R | 68.2% | 30.8% | 1% | 68.2% | - | 6.1% | - | 22.7% | - | - | 2.5% | 96.3% | 2.7% | 1.1% | 96.3% | - | 1.6% | - | 1.1% | - | - | 0.5% | |
4. DISCUSSION
In the present retrospective study, mandibular premolars were evaluated using CBCT to detect the internal and external morphologies, which indicate that most of the first and second premolars had one root and one canal and a complicated root canal system. The preoperative diagnosis of endodontic cases includes clinical examination and diagnostic imaging as an essential aid [19]. Precise radiographic imaging helps clinicians reach a better diagnosis by obtaining a better view of the root canal anatomy. Many methods have been used to study the root canal configuration, including the use of dye, the clearing of teeth [20], injecting the teeth with radiopaque contrast media, and taking digital radiography [21]. In the above studies, teeth were extracted, and the samples were irreversibly destroyed; consequently, the results could not be produced or analyzed again [22]. In addition, traditional 2D radiographs, like the widely used intra-oral periapical radiographs, have limited diagnostic potential as they are difficult to understand, particularly when the anatomy and the background pattern are intricate [23]. Thus, diagnostic tools, like CBCT, which can provide precise 3D image quality with low radiation exposure, are necessary. Compared with conventional radiographs, CBCT exhibits superior image reliability and delivers images of soft and hard tissues [24]. Thus, in the present study, CBCT was used to analyze the root canal morphology of mandibular premolars in the Saudi Arabian sub-population. A detailed comparison of our results and those of other studies is presented in Table 5.
4.1. Mandibular First Premolars
According to the present study, 99.5% of the mandibular first premolars had one root and 69.5% of the premolars had one canal, indicating that majority of the mandibular first premolars had one canal. This finding is consistent with the results of the studies conducted by Zare Jahromi et al. on the Iranian population [25], Alfawaz et al. on the Saudi population [16], Jang et al. on the Korean population [26], Vyoma et al. on the Indian population [27], Chourasia et al. on Southern Saudi Arabian sub-population [17], and Llena et al. on Spanish population [1]. The studies mentioned above also revealed that the number of first premolars with two canals was lower than that of the first premolars with one canal, which is consistent with the finding of the present study in which only 29.5% of the mandibular first premolars had two canals. Similarly, the mandibular first premolars with three canals account only for 1% of the total sample size in our study, but those in the studies by Chourasia et al. on the Southern Saudi Arabian sub-population [17] and Llena et al. on the Spanish population [1] accounted for 2% and 2.6% of the sample size, respectively. In a few studies, the mandibular first premolars with three canals were reported to be 0 and 0.5% in the Iranian and Saudi populations [16, 25]. Vertucci’s classification of canal configuration in the present study reveals that 69.5%, 6.3%, 22.2%, and 0.3% of the mandibular first premolars had Vertucci type I, type III, type V, and type VII canal configurations, and 1.8% had a different canal configuration, which is not described by Vertucci’s classification and can be addressed by a different classification system, like that of Ahmed et al. [28].
The comparison of this study’s results with those of other studies indicates that the majority of the canals have a Vertucci type I canal configuration [1, 16, 17, 26, 27]. Some studies also reported the presence of type III canal configuration in mandibular first premolars [16, 17, 26]. Chourasia et al. reported the highest percentage of type III canal configuration of 8% in a study conducted on the Southern Saudi Arabian sub-population [17]. The next highest percentage of type III canal configuration was reported in our study, that is, 6.1% to 6.5%. In the Indian and Korean populations, the percentages are 2% and 3.19%, respectively [26, 27].
In the present study, we also compared the mandibular first premolars on the contralateral sides in terms of the number of canals and Vertucci’s classification for canal configuration. The mandibular first premolars on the right side reported a higher presence of two canals (i.e., 30.8%) than those on the left side (i.e., 28.1%), but the difference was insignificant. The findings are consistent with those of a study on the Malaysian population using the same methodology [29].
In terms of canal configuration, mandibular first premolars to the left showed 70.9% of Vertucci’s type I configuration, 6.5% showed type III configuration, and 21.6% showed type V configuration. Similarly, on the right side, 68.2% of mandibular first premolars had Vertucci’s type I configuration, 6.1% showed type III configuration, and 22.7% showed type V configuration. This type of comparison was done for the first time in our study. In a few studies, the only number of canals was compared in contralateral premolars, but the comparison in terms of Vertucci’s classification has not been reported [1, 27].
4.2. Mandibular Second Premolars
In the present research, an assessment of the mandibular second premolar was also done. It was observed that 100% of mandibular second premolars had one root and 96.8% had one canal, which indicates that most mandibular second premolars had 1 canal. This finding was in accordance with the results of studies conducted by Zare Jahromi et al. on the Iranian population [25], Alfawaz et al. on the Saudi population [16], Jang et al. on the Korean population [26], Vyoma et al. on the Indian population [27], Chourasia et al. on the Saudi Arabian southern region sub-population [17], and Llena et al. on the Spanish population [1].
In all the above-stated research, it was also observed that 2nd premolars with 2 canals were reasonably lesser than 2nd premolars with 1 canal. This was observed in the present study also wherein only 2.1% of mandibular second premolars consisted of 2 canals. Likewise, in our study, mandibular second premolars with 3 canals accounted for only 1.1% of the total sample size but conferring to the study conducted by Llena et al. on the Spanish population [1], mandibular second premolars with 3 canals accounted for 0% of the sample size. When categorized by Vertucci’s classification of canal configuration, it was observed in the present study that 96.8% of mandibular second premolars had Vertucci’s type I canal configuration, 1.6% had type III canal configuration, 0.8% had type V canal configuration, 0.8% had type VII canal configuration, and 0.8% had different canal configuration that is not described in Vertucci’s classification. When this result was compared with other studies, it was witnessed that in all studies majority of the canals had Vertucci’s type I canal configuration [1, 16, 26, 27]. Few studies also reported the presence of type III canal configuration in mandibular first premolars [16, 17, 26]. The highest percentage of type III canal configuration was reported to be 2% in a study conducted by Vyoma et al. on the Indian population [27]. The next highest percentage of type III canal configuration was reported in our study, which was 1.6%.
The mandibular second premolars on the contralateral sides were also evaluated in terms of the number of canals and Vertucci’s classification for canal configuration. The mandibular second premolars on the right side reported a higher presence of two canals (i.e., 2.7%) than those on the left side (i.e., 1.6%). In terms of canal configuration, 97.4%, 1.6%, and 0.5% of the mandibular second premolars in the left side exhibited Vertucci’s type I, type III, and type V configurations, respectively. Similarly, 96.3%, 1.6%, and 1.1% of the mandibular second premolars on the right side have Vertucci’s class I, type III, and 1.1% type V configurations, respectively. Our results are consistent with those of the study on the Malaysian population [29], with no statistically significant difference between the right and left sides.
The null hypothesis was accepted, and the results of the present investigation fell within the range of national and international studies.
This study has some limitations, including the sample size, which could result from having data from only one city. However, it added to the body of knowledge in the Saudi population since limited studies were found. Also, the results show the importance of CBCT in detecting the root canal system precisely regardless of the limitations. A similar study could be conducted with a larger sample size from all regions of Saudi Arabia to improve the accuracy of the results.
CONCLUSION
The results of the present study indicate that majority of the first and second mandibular premolars have one root with one canal. Some variations were observed and verified by a small field of view CBCT during treatment planning when 2D periapical- radiography could not provide enough details for a more predictable outcome.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
Prior to the study, ethical approval from the Scientific Research-College of Dentistry, Jazan University (Ref#: CODJU-1922F) was obtained.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
No consent form was required from the patients because all CBCTs were retrieved retrospectively from the archive of the College of Dentistry.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available from the corresponding author [S.B], upon a reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

