All published articles of this journal are available on ScienceDirect.

Awareness and Utilization of Bulk-Fill Composites among Dental Practitioners in Saudi Arabia
Abstract
Objective:
The aim of this study was to assess the knowledge and utilization of Bulk-Fill (BF) resin composites among dental practitioners in Saudi Arabia.
Materials and Methods:
An online survey was distributed through Twitter, Instagram and WhatsApp applications among dentists in Saudi Arabia. A 31-item questionnaire covering personal data, general knowledge and utilization of BF composites was used. Responses were collected and analyzed for trends. A knowledge scale was developed based on answers with specific weight for each correct answer provided by the participants. A score of ≥ 50% was considered as a satisfactory knowledge level for participants. Statistical analysis was conducted using One-sample Z- and Chi-square tests followed by Bonferroni correction at 0.05 significance level.
Results:
The total number of participants of the survey was 183, of which 41.5% had some knowledge and utilized BF composites in their practice. Only 9.84% of the participants score ≥ 50% on the knowledge scale. A significantly low proportion recognized accurately the compositional difference between BF and conventional resin composite as well as the minimum irradiance values needed for proper polymerization of BF. There was no effect for gender or years of experience on the knowledge or utilization of BF materials (p-value = 0.172).
Conclusion:
The proportions of practitioners with adequate knowledge and utilization of BF materials were very low. Additional focus must be provided in order to expose graduating dentists to advances in resin composite formulations.
1. INTRODUCTION
The use of dental composite is increasing owing to patient’s demand for tooth-colored restorations [1]. The properties of composite resins have improved significantly in the last few years [2]; however, inherent limitation owing to the shallow depth of cure of resin composite necessitated the utilization of an incremental technique during the placement of composites in cavities deeper than 2 mm [3, 4]. This is done to ensure that light from curing devices can reach the deeper parts of the restoration leading to an adequate degree of conversion of monomers into polymers [5]. This is very critical to the longevity of the restorations since it was reported previously that under-cured resin composites are more likely to fail, necessitating their replacement [6-8].
In order to streamline the clinical procedure of deeper cavities, new formulations were developed which allow for the filling of cavities up to 5 mm deep in a single increment. These materials are known as Bulk-Fill (BF) resin composites [9]; and have different chemistries compared to conventional resin composites [10]. BF materials tend to have special fillers with more translucency values in order to allow deeper penetration of light [11]. Also, higher light-cure irradiance values are required in order to deliver enough energy into the bottom of the cavity enabling the polymerization of the material. Even though, irradiance values between 400 and 600 mW/cm2 can be considered adequate for curing conventional resin composite [12], BF formulations require irradiance values exceeding 1,000 mW/cm2 in order to ensure an adequate degree of conversion [13]. Further, new and more sensitive photoinitiators are used to ensure adequate initiation and propagation of the polymerization reaction [9].
Understanding key differences in chemistry and application techniques between conventional and BF resin composite is very important to clinicians. Since these materials are relatively new, not all practicing dentists might be aware of these differences. Choosing the correct material, the proper application technique and the light curing device with adequate irradiance value are paramount in ensuring a successful restoration. Furthermore, proper utilization data must be known in order to provide relevant recommendations for daily practice, especially for recently graduating dentists.
Thus, the aim of the current study was to assess the knowledge and utilization of dental practitioners of bulk-fill resin composite materials. Establishing a baseline knowledge status can allow decision-makers and university professors to cope with workplace practices as well as community demand.
2. MATERIALS AND METHODS
2.1. Ethics Statement
The questionnaire and methodology for this study were approved by the Research Ethics Committee of the Faculty of Dentistry at King Abdulaziz University (Ethics approval number: 112-10-19 in April, 3rd, 2019). Further, a confidentiality disclosure was included in the introductory portion of the online questionnaire. The study was conducted between November 2019 and March 2020.
2.2. Target Group
The target audience for the survey was dental practitioners in Saudi Arabia. The questionnaire was sent electronically via social media applications (Twitter, Instagram, Telegram, and Whatsapp) based on local databases targeting governmental universities and hospitals as well as private schools and practices. The selection was random based on sending the link over the social media outlets.
2.3. Online Questionnaire Design
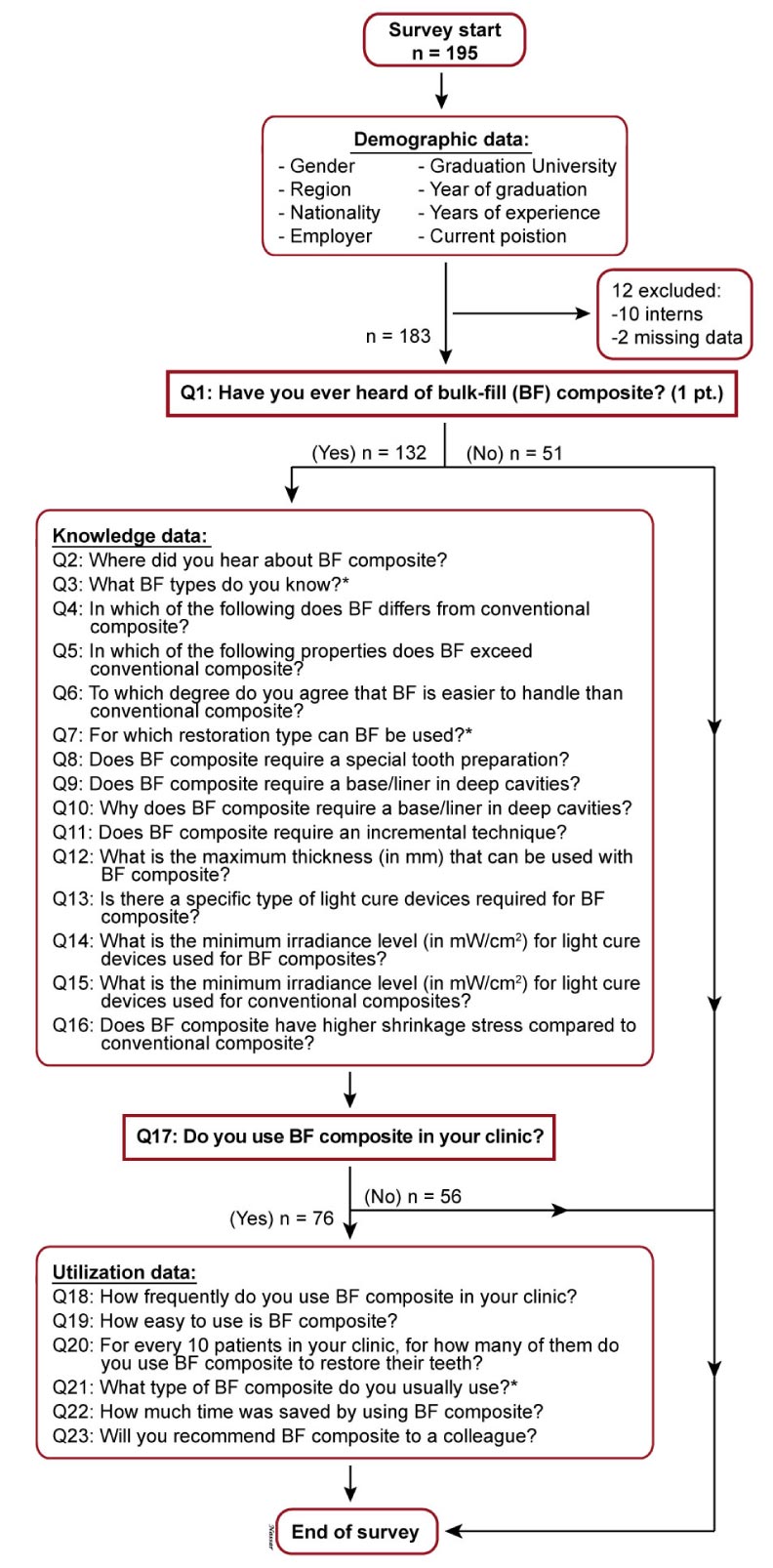
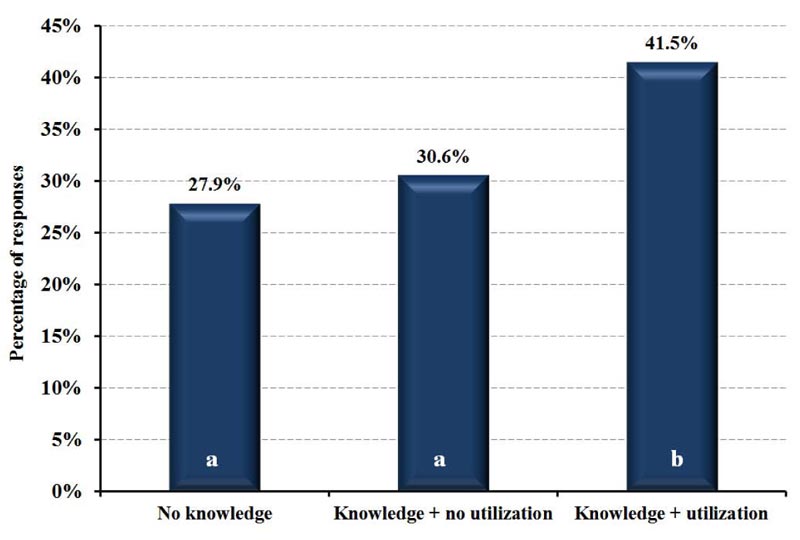
The online questionnaire was designed using Google Forms software (Google LLC, Mountain View, California, United States) and was divided into sections: 1) demographic data [8 questions], 2) knowledge about BF resin composite properties and technique [16 questions], and 3) utilization of BF resin composite in daily practice [6 questions]. After the demographic information part of the survey, two conditional questions were included in the survey at the beginning of the knowledge and utilization sections (Fig. 1). Based on answering these two questions, the participants were categorized into 3 groups: 1) participants without knowledge, 2) participants with knowledge but no utilization, or 3) participants with knowledge and utilization.
2.4. Study Parameters
For each parameter within the demographic data, each answer level was compared to others to determine trends and differences within the sample. For each question within the knowledge section, the proportion of participants with the correct answer was determined. Each correct answer was given a score, and the total knowledge scale (KS; out of 25 points) was determined for each participant to estimate the level of knowledge concerning BF resin composite. A KS ≥ 50% was considered a satisfactory knowledge level. For the utilization section, proportions of answers for each question were compared. Furthermore, the effect of demographic data on knowledge and the effect of knowledge on utilization were also investigated.
2.5. Statistical Analysis
All Data were collected, tabulated and subjected to statistical analysis. All analyses were performed using SPSS Version 20 (SPSS Inc., Chicago, Illinois, USA). Qualitative categorical variables were described by frequencies and percentages. Data were presented, when appropriate, by the Pareto method. Quantitative variables were described by the mean and standard deviation.
Shapiro-Wilk test of normality was used to test the normality hypothesis of the knowledge scale. Z test was applied for the difference between two proportions. Chi-squared test was used for the assessment of the relation between two categorical variables. Post-hoc analysis using adjusted residuals and Bonferroni correction were used for further analysis of the effect of employment status if the chi-squared test was significant. A 0.05 significance level was used for all tests. During analysis, some answer options were grouped together in order to maintain the statistical assumptions of the test.
3. RESULTS
3.1. Demographic Data
A total of 195 responses were received for the online survey; of which 12 were excluded (10 participants were interns and 2 responses had missing data; Fig. 1). Consequently, the final number of participants in this survey was 183 practitioners. Fifty-one participants did not have previous knowledge of BF composites, and 132 had some knowledge; of which 76 practitioners had used BF composite at some point. The general characteristics of the cohort are included in Table 1. Most participants were general practitioners (95%), graduated from King Abdulaziz University (57%) during the last 10 years (91%), and with less than 5 years of experience (86%).
| Category | Response | Percent | Significance Between Responses | P-Value for Z-test |
|---|---|---|---|---|
| Gender | Male | 49.7 | No | 0.92 |
| Female | 50.3 | |||
| Nationality | Saudi* | 97.8 | Yes | < 0.001 |
| Non-Saudi | 2.2 | |||
| City/region | Central region | 9.8 | Yes | < 0.001 |
| Western region* | 80.9 | |||
| Eastern region | 4.9 | |||
| Northern region | 1.1 | |||
| Southern region | 3.3 | |||
| Graduation University | Taiba University | 3.8 | Yes | < 0.001 |
| King Saud University | 4.4 | |||
| King Khalid University | 1.6 | |||
| Um Al Qura University | 2.2 | |||
| Alfarabi College | 4.4 | |||
| King Abdulaziz University* | 57.4 | |||
| Ibn Sina College | 9.8 | |||
| Batterjee College | 2.7 | |||
| Imam University | 1.6 | |||
| Other | 12 | |||
| Year of Graduation | Before 1980 | 0 | Yes | < 0.001 |
| 1981 - 1990 | 0.6 | |||
| 1991 - 2000 | 2.7 | |||
| 2001 - 2010 | 6.0 | |||
| 2011 – 2019* | 90.7 | |||
| Current Position | General practitioner* | 94.5 | Yes | < 0.001 |
| Specialist | 3.8 | |||
| Consultant | 1.1 | |||
| Other | 0.6 | |||
| Years of Experience | < 5* | 86.3 | Yes | < 0.001 |
| 5 - 9 | 10.9 | |||
| 10 - 15 | 1.1 | |||
| >15 | 1.1 | |||
| Employer | Unemployed | 44.8 | No | 0.054 |
| Government | 31.7 | |||
| Private | 23.5 |
3.2. Knowledge Data
Only 76 out of 183 (41.5%) participants have the knowledge and utilize BF composite. Fig. (2) illustrates the proportions of participants in regards to knowledge and utilization. There was no significant difference between females (18%) and males (9.9%) regarding knowledge of BF materials (p = 0.172). The knowledge scale (KS), normalized on a 100 point, with a score below 50% was considered unsatisfactory. The KS data followed a normal distribution and showed that only 18 out of 123 (9.84%) participants had a satisfactory knowledge level. KS was not influenced by gender, years of experience or employment status (p> 0.05).
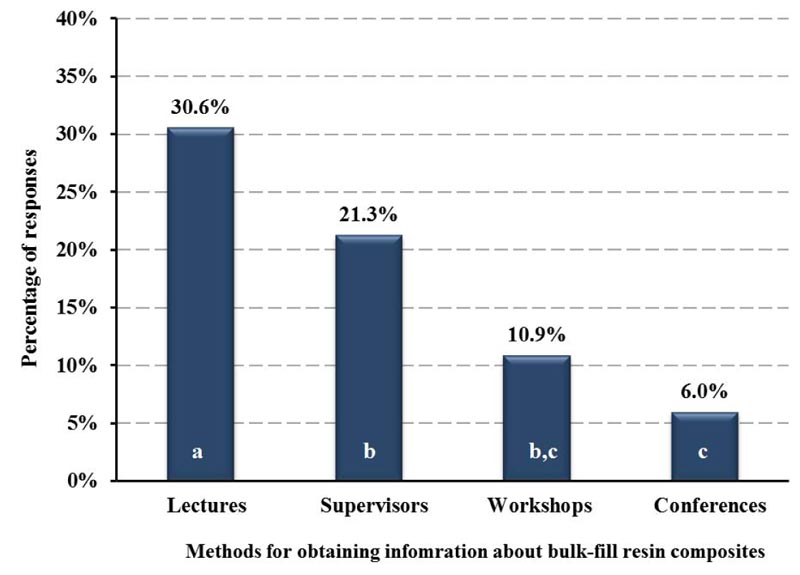
Table 2 shows the proportions of answers for each question in the knowledge section of the survey along with the results of statistical tests. The data is presented both out of the total participants of the survey (n = 183; percentages might not add to 100%) and out of the participants who responded yes to Q1 (n = 132; percentages will add up to 100%). Lectures were the main source of information (Fig. 3), SDR was the most commonly reported BF material by participants, and core build-up was the most frequent application reported (Fig. 4).
Considering the difference between BF and conventional composites, only a significantly low proportion (7%) chose “photoinitiators” (p< 0.001). A similarly low proportion (7%) chose “degree of conversion/depth of cure” (p< 0.001). In addition, BF materials were considered easier to use compared to conventional formulations (p< 0.001), being not suitable for anterior restorations (6%), and do not require a special cavity preparation (62%) or an incremental approach (70%).
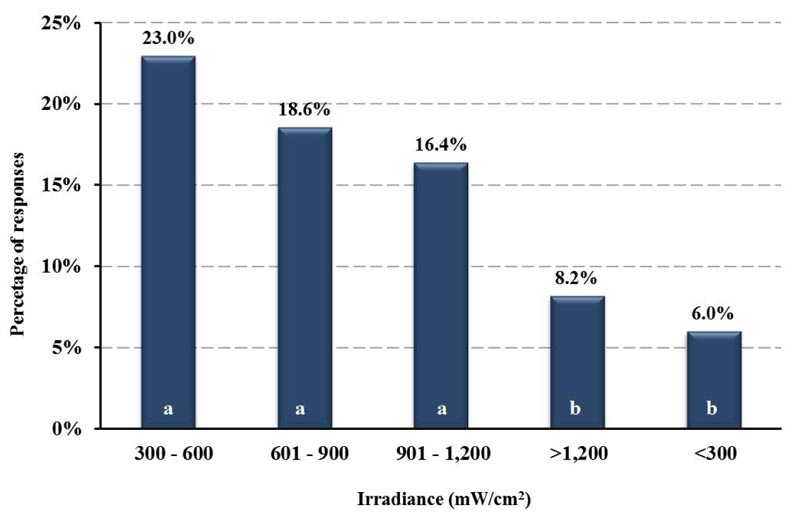
Regarding the minimum irradiance level in mW/cm2 for light cure used for BF resin composites, 300 - 600, 601 - 900, and 901 - 1200 mW/cm2 were the ranges commonly chosen with no statistical significance between the choices. (p> 0.05; Fig. 5). For conventional composites, however, 901 - 1200, 300 - 600, and 601 - 900 were the ranges chosen with no statistically significant difference between the choices (p> 0.05).
| Question | Answer (Abbreviation) |
Out of Total Participants (n = 183)1 |
Percentage out of Knowledgeable Participants (n = 132)2 |
Multiple Comparison | P-Value | Knowledge Score (points) | ||
|---|---|---|---|---|---|---|---|---|
| % | Total | % | Total | |||||
| Q2 | Lectures (L) | 31 | 69 | 44 | 100 | L vs. S | 0.043 | 1 |
| - | Supervisors (S) | 21 | 31 | - | S vs. W | 0.007 | 1 | |
| - | Workshops (W) | 11 | - | 16 | - | W vs. C | 0.091 | 1 |
| - | Conferences (C) | 6 | - | 9 | - | 1 | ||
| Q3 | SDR (BF1) | 35 | 105 | 33 | 100 | BF1 vs. BF2 | 0.58 | 0.5 |
| - | FilltekBulk-Fill (BF2) | 32 | 31 | - | BF1 vs. BF3 | 0.022 | 0.5 | |
| - | TetricBulk-Fill (BF3) | 24 | 23 | - | BF2 vs. BF3 | 0.081 | 0.5 | |
| - | Sonic Fill 2 (BF4) | 14 | 13 | - | BF2 vs. BF4 | < 0.001 | 0.5 | |
| - | - | - | BF3 vs. BF4 | 0.011 | ||||
| Q4 | Polymers (P) | 11 | 106 | 11 | 100 | Ph vs. P) | < 0.001 | 0 |
| - | Filler particles (FP) | 27 | 26 | - | Ph vs. FP | < 0.001 | 0 | |
| - | Photoinitiators (Ph) | 8 | 7 | - | 2 | |||
| - | Polymerization reaction (PR) | 19 | 18 | - | Ph vs. PR | < 0.001 | 0 | |
| - | Polymerization shrinkage and gap formation (PS) | 40 | - | 38 | - | Ph vs. PS | < 0.001 | 0 |
| Q5 | Durability (D) | 17 | 126 | 13 | 100 | DC vs. D | < 0.001 | 0 |
| - | Color stability (CS) | 9 | 7 | - | DC vs. CS | < 0.001 | 0 | |
| - | Polymetric stability (PS) | 18 | 14 | - | DC vs. PS | < 0.001 | 0 | |
| - | Marginal adaptability (MA) | 28 | 22 | - | DC vs. MA | < 0.001 | 0 | |
| - | Degree of conversion/depth of cure (DC) | 8 | - | 7 | - | - | - | 2 |
| - | Polymerization shrinkage (PS) | 44 | 35 | - | DC vs. PS | < 0.001 | 0 | |
| - | None | 2 | 1 | - | DC vs. None | < 0.001 | 0 | |
| - | Other | 1 | - | DC vs. Other | < 0.001 | 0 | ||
| Q6 | Agree vs. strongly agree | 56 | 68 | 78 | 100 | Agree vs. Disagree | < 0.001 | 0.5 / 1.0 |
| - | Disagree vs. strongly disagree | 6 | 8 | - | 0 | |||
| - | Undecided | 6 | 14 | - | 0 | |||
| Q7 | Core Buildup (TR1) | 49 | 131 | 38 | 100 | TR1 vs. TR2 | 0.015 | 0.5 |
| - | Posterior Restoration (TR2) | 37 | 28 | - | TR2 vs. TR3 | 0.662 | 1 | |
| - | MOD (TR3) | 34 | 26 | - | TR2 vs. TR4 | < 0.001 | 1 | |
| - | Anterior Restoration (TR4) | 6 | 5 | - | TR3 vs. TR4 | < 0.001 | 0 | |
| - | I don't know | 4 | 3 | - | 0 | |||
| Q8 | No | 44 | 72 | 62 | 100 | No vs. Yes | < 0.001 | 1 |
| - | Yes | 9 | 13 | - | 0 | |||
| - | Maybe | 10 | 14 | - | 0 | |||
| - | I don't know | 8 | 11 | - | 0 | |||
| Q9 | No | 14 | 72 | 19 | 100 | No vs. Yes | < 0.001 | 0 |
| - | Yes | 44 | 61 | - | 1 | |||
| - | I don't know | 14 | 20 | - | 0 | |||
| Q10 | For pulpal protection from unreacted monomer (BDC1) | 27 | 72 | 38 | 100 | BDC1 vs. BDC2 | 0.276 | 1 |
| - | For pulpal protection from mechanical irritant (BDC2) | 22 | 31 | - | BDC1 vs. BDC3 | < 0.001 | 0 | |
| - | For better marginal adaptation (BDC3) | 5 | - | 7 | - | BDC2 vs. BDC3 | < 0.001 | 0 |
| - | I don't know | 17 | - | - | 0 | |||
| Q11 | No | 50 | 72 | 70 | 100 | No vs. Yes | < 0.001 | 0.5 |
| - | Yes | 9 | 12 | - | 0 | |||
| - | Maybe | 8 | 11 | - | 0 | |||
| - | I don't know | 5 | 7 | - | 0 | |||
| Q12 | 3 | 13 | 72 | 18 | 100 | 3 vs. 4 | < 0.001 | 0 |
| - | 4 | 34 | 47 | - | ≥5 vs. 4 | 0.067 | 2 | |
| - | ≥5 | 25 | 35 | - | ≥5 vs. 3 | 0.009 | 0 | |
| Q13 | No | 54 | 72 | 74 | 100 | No vs. Yes | < 0.001 | 0 |
| - | Yes | 19 | 26 | - | 2 | |||
| Q14 | 300 - 600 (IRR1) | 23 | 72 | 32 | 100 | IRR1 vs. IRR2 | 0.303 | 0 |
| - | 601 - 900 (IRR2) | 19 | 26 | - | IRR1 vs. IRR3 | 0.115 | 0 | |
| - | 901 - 1,200 (IRR3) | 16 | 23 | - | IRR1 vs. IRR4 | < 0.001 | 2 | |
| - | >1,200 (IRR4) | 8 | 11 | - | IRR2 vs. IRR3 | 0.582 | 0 | |
| - | <300 (IRR5) | 6 | 8 | - | IRR2 vs. IRR4 | 0.004 | 0 | |
| - | - | - | IRR3 vs. IRR4 | 0.017 | ||||
| - | - | - | IRR4 vs. IRR5 | 0.416 | ||||
| Q15 | 901 - 1,200 (IRR1) | 24 | 72 | 33 | 100 | IRR1 vs. IRR2 | 0.452 | 0 |
| - | 300 - 600 (IRR2) | 21 | 29 | - | IRR1 vs. IRR3 | 0.092 | 1 | |
| - | 601 - 900 (IRR3) | 17 | 24 | - | IRR1 vs. IRR4 | < 0.001 | 2 | |
| - | <300 (IRR4) | 8 | 11 | - | IRR2 vs. IRR3 | 0.35 | 0 | |
| - | >1,200 (IRR5) | 2 | 3 | - | IRR2 vs. IRR4 | 0.001 | 0 | |
| - | - | - | IRR3 vs. IRR4 | 0.012 | ||||
| - | - | - | IRR4 vs. IRR5 | 0.01 | ||||
| Q16 | No | 20 | 72 | 28 | 100 | No vs. Yes | 0.068 | 2 |
| - | Yes | 28 | 39 | - | 0 | |||
| - | Maybe | 10 | 14 | - | 0 | |||
| - | I don't know | 14 | 19 | - | 0 | |||
2Percentages out of participants who responded yes to Q1 (participants with knowledge about bulk-fill composites). Percentages will add up to 100%.

| Question | Answer (Abbreviation) |
Out of Total Participants (n = 183)1 |
Percentage out of Bulk Fill Users (n=76)2 |
Multiple Comparison | P-Value | ||
|---|---|---|---|---|---|---|---|
| % | Total | % | Total | ||||
| Q18 | Never | 31 | 72 | 42 | 100 | Never vs. Rarely | 0.076 |
| Rarely | 22 | - | 31 | - | Never vs. Often | < 0.001 | |
| Sometimes (every 2-3 month) | 7 | - | 9 | - | Rarely vs. Often | 0.013 | |
| Often | 13 | - | 18 | - | Sometimes vs. Often | 0.051 | |
| Q19 | Easy | 27 | 40 | 68 | 100 | Easy vs. Other responses | < 0.001 |
| Other responses (not easy) | 13 | - | 32 | - | - | - | |
| Q20 | 1-3 | 29 | 42 | 70 | 100 | 1-3 vs. 4 or more | < 0.001 |
| 4 or more | 13 | - | 30 | - | - | - | |
| Q21 | SDR (BF1) | 23 | 56 | 41 | 100 | BF1 vs. BF2 | 0.369 |
| Filltek Bulk-Fill(BF2) | 19 | - | 34 | - | BF1 vs. BF3 | 0.002 | |
| Tetric Bulk-Fill (BF3) | 11 | - | 20 | - | BF2 vs. BF3 | 0.028 | |
| SonicFill 2 (BF4) | 2 | - | 4 | - | BF3 vs. BF4 | < 0.001 | |
| Other | 1 | - | 1 | - | - | - | |
| Q22 | Very little | 8 | 39 | 20 | 100 | A lot of time vs. Very little | 0.01 |
| Sometime | 15 | - | 38 | - | A lot of time vs. Sometime | 0.665 | |
| A lot of time | 16 | - | 42 | - | Sometime vs. Very little | 0.031 | |
| Q23 | No/Maybe | 10 | 42 | 24 | 100 | No/Maybe vs. Yes | < 0.001 |
| Yes | 32 | - | 76 | - | - | - | |
2Percentages out of participants who responded yes to Q17 (bulk-fill user).Percentages will add up to 100%.
3.3. Utilization Data
There was no significant effect for years of experience on the utilization of BF materials. Also, the effect of gender was not significant (females = 49.2%, males = 36.6%; p= 0.172). However, Post-hoc analysis with Bonferroni correction revealed that unemployed participants had lower utilization compared to the employed groups (p = 0.017).
Table 3 summarizes answers for each question in the utilization section of the survey as well as results of statistical analysis. The data is presented both out of the total participants of the survey (n = 183; percentages might not add to 100%) and out of the participants who responded yes to Q17 (n = 76; percentages will add up to 100%). The majority of participants did not use BF resin composites (53%); however, among those who did, SDR was the most used (23%), and 27% of these groups considered the technique to be easy. Still, only between 1 and 3 in every 10 patients are provided a BF composite restoration since only 31% of the group utilizing BF believed it saved them sometime during the clinical encounter.
Regardless of the ease of use and time saving with BF composites, these factors have no statistically significant effect on the use or frequency of use of BF composites (p> 0.05). However, there was a strong correlation between the ease of use and recommendation of the use of BF composites to a colleague (p< 0.001).
4. DISCUSSION
BF composites have been launched to the dental market to simplify restorative procedures by filling cavities in one increment. This has been related to the translucency of resin matrix [14] and the development of new photoinitiator systems [15], which allow curing of BF composites in an increment of 4 – 5 mm [16]. Since then, their use has been extended to cover several applications, including posterior restorations [17], bases and liners [18] and core build-up [19]. These materials are available as low viscous (flowable) or highly viscous (sculptable). The flowable types suit deep parts of cavities as they can easily flow to fill all parts, but they are not strong enough to withstand forces of mastication. They, therefore, have to be capped with the more viscous type [20]. This survey aimed to investigate the awareness and utilization of BF composites among dental practitioners working in Saudi Arabia.
The proportion of females with satisfactory knowledge level was higher than males, but when it comes to utilization, females had a lower utilization rate than males. As expected, with ≥ 5 years of experience, the level of satisfactory knowledge and utilization of BF composites increases and working in privates sectors was associated with a higher level of satisfactory knowledge and utilization rate. On the contrary, regardless of the ease of use and time saving with BF composites as highlighted by participants, this has no impact on their utilization or frequency of use but the recommendation to colleagues. This indicates that there is no association between the knowledge the participants had and their utilization. This could be related to materials availability, participants’ preference, or lack of training.
Considering the difference between BF and conventional composites, polymerization shrinkage and gap formation came first but not photoinitiators, degree of conversion, and depth of cure. This could indicate that the participants are only concerned with the clinical performance of the material but not with the actual change in composition that brought such performance. Several approaches have been employed by manufacturers to improve the depth of cure of BF composites [21]. They include the addition of more reactive photoinitiators to the commonly used comphorquinone [22]. Another approach relies on increasing the material translucency by increasing the filler content, reducing the filler size and controlling its refractive index [23]. It is imperative that the practicing dentist becomes aware of these variations in order to modify the application technique based on the intended application.
Regarding the polymerization shrinkage and gap formation of BF versus conventional composites, there is a big controversy in the literature, and this has always been related to the type of BF being used [24, 25, 23]. Some studies showed that BF composite has lower polymerization shrinkage and gap formation than conventional composites [26, 27]. Other studies, however, showed comparable shrinkage for both material types [28, 29]. Studies focusing on photoinitiator systems in both BF and conventional composites are very scarce. This might also contribute to the lack of concern of participants with the type of photoinitiators in their responses.
Although participants showed good overall knowledge regarding the fact that bulk-fill composites can be used at once to fill cavities of 4 - 5 mm, it should also be brought to attention that in cases where the cavity depth is greater than 5 mm, as in endodontically treated teeth or in class II cavities with very deep gingival margin, an incremental approach is recommended with a maximum incremental size of 4 - 5 mm following manufacturer’s recommendations. This is needed to ensure adequate transfer of the light energy from the light cure device across the material and into the deeper potions of the filling.
Polymerization of the dental composite is crucial for optimizing its physical and mechanical properties as well as the clinical success [30]. Inadequate polymerization results in reduced mechanical and physical properties, decreased bond strength with tooth structure, marginal deterioration, and possible cytotoxicity [31]. Therefore, using the appropriate light-curing unit to deliver adequate and sufficient energy required for optimum polymerization is needed. For polymerization of dental composites, irradiation with blue or blue/violet light is required [32]. Parameters as irradiance, radiance exposure, and irradiation spectrum are the main parameters to be considered for each light curing unit used for polymerization of dental composites [32]. With recent light emitting diode (LED) curing devices, the irradiance has been dramatically enhanced to reduce the exposure time required for successful polymerization [33]. Most modern devices operate at irradiance of 1000 - 1500 mW/cm2. The conventional quartz-tungesten-halogen (QTH) curing devices have irradiance level of 400 - 500 mW/cm2, [34]. With BF composites that have a variety of photoinitiators, the development of curing unit with multiple LEDs (polywave LED) has been introduced to emit different wavelengths to cover different photoinitiators [36]. For most BF composites, a monowave or polywave LED curing device with irradiance level ≥1000 mW/cm2 is required [35]. From the responses in the survey, there is a knowledge gap regarding the minimum irradiance level required for both BF and conventional composites. The most commonly chosen level was 300 - 600 mW/cm2 for BF and 901 - 1200 mW/cm2 for conventional composites.
CONCLUSION
According to the results of this survey, several key points require reinforcement and hands-on training in both didactic and clinical sessions. Firstly, nearly 93% of the participants, unemployed males with >5 years of experience, in particular, have unsatisfactory knowledge level about BF composites. Since the study was conducted between November 2019 and March 2020, some effects of the COVID-19 pandemic might have affected the employment status. Secondly, most participants considered polymerization shrinkage and gap formation, but not the photoinitiator and depth of cure, as the main difference between BF and conventional composites. Thirdly, the minimum irradiance level of light cure, required for BF and conventional composites, has also been misperceived by participants. Finally, regardless of the ease of use and time saving with BF composites as highlighted by participants, these factors had no statistically significant effect on the use or frequency of use of BF composites by participants. The highest utilization rate was observed with those having ≥ 5 years of experience; still, the overall utilization of BF was low. There was, however, a strong correlation between the ease of use and recommendation of the use of BF composites to colleagues. Therefore, for a future course or program improvement, different ways to encourage participants to apply what they learn should be considered to solve this issue.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the ethical committee of the Ethics Committee of the Faculty of Dentistry at King Abdulaziz University, Saudi Arabia (Ethics approval number: 112-10-19 in April, 3rd, 2019).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
A consent form was signed by all participants.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author, [H.M.N.] upon a reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

