
Benign Orofacial Lesions in Libyan Population: A 17 Years Retrospective Study
Authors Info & Affiliations
Abstract
Objectives: To analyze the frequency and type of benign orofacial lesions submitted for diagnosis at Tripoli Medical Centre over 17 years period (1997-2013). Materials and Methods: Entries for specimens from patients were retrieved and compiled into 9 diagnostic categories and 82 diagnoses. Results: During the 17 years period, a total of 975 specimens were evaluated, it comprised a male-female ratio of 0.76:1. The mean age of biopsied patients was 36.3±18.32 years. The diagnostic category with the highest number of specimens was skin and mucosal pathology (22.87%); and the most frequent diagnosis was pyogenic granuloma (14.05%). Conclusion: Pyogenic granuloma, lichen planus, radicular cyst and fibroepithelial polyp were found to be the most predominant diagnoses. Frequencies of most benign orofacial diseases were comparable to similar studies in the literature and to those reported from the eastern region of Libya. Further surveys are needed to define the epidemiology of orofacial diseases in Libyan population.
INTRODUCTION
Histopathological analysis is an important complementary tool that aids in the establishment of a definitive diagnosis. It is essential that dental practitioners have a perceived knowledge of the clinical and demographic characteristics associated with the occurrence of the versatile benign orofacial lesions, since many of them may exhibit similar clinical and/or radiographic characteristics to one another or may resemble malignant conditions.
Conducting an overall and detailed medical history and a comprehensive exploration of the oral cavity is essential to obtain a correct diagnosis. This influences the prognosis and the implementation of the appropriate treatment for each patient.Although occasionally it is possible to establish a clinical diagnosis, in most cases it is essential to conduct additional simple tests that provide valuable information, such as biopsies.
Biopsy is of paramount importance in the diagnostic process of oral lesions which, by clinical examination alone, can often be difficult and inaccurate [1]. Of particular importance is the contribution of biopsy and histopathology to the early detection of premalignant and malignant Lesions. Failure to biopsy may lead to persistence of a misdiagnosed malignant lesion or other serious pathology, resulting in an unfavourable downstream course for the patient and the attending clinician [2].
Most of the published epidemiological studies on orofacial lesions including those among Libyan population [3-6] are concerned with documenting the incidence or the prevalence of specific disease entity, such as dental caries, periodontal diseases or oral mucosal lesions. Furthermore, the majority of these investigations lack histological confirmation of diagnosis. Relatively few published surveys document the range of histologically diagnosed lesions over a given time frame. Among these, three studies from the United States with 400 specimen over one year [7], 4723 specimens over 20 years [8] and 15783 specimens over 18.5 years [9], one study from Spain with 562 specimen over 14 years [10], another from Singapore with 2057 specimen over 5 years [11] and the largest survey comprising 44007 specimens submitted over 30 years in the United Kingdom [12].
Moreover, there are few documentations of the occurrence of orofacial lesions in Africa and the Middle East. These include: a study of 818 benign oral masses among Jordanian population [13] which reported high frequencies of pleomorphic adenoma, pyogenic granuloma and fibroepithelial polyp, a survey of 385 biopsied jaw lesions in Kuwait [14] that reported high frequencies of radicular cyst, dentigerous cyst and keratocystic odontogenic tumor and a survey of 310 oral lesions in Yemen [15] that reported high frequencies of benign tumors and Qad-induced white lesions. In Libya, a study of 405 benign tumors revealed that keratocystic odontogenic tumors and ameloblastoma were the most predominant diagnoses [5].
The aim of this study was to determine the range and the demographic characteristics of benign orofacial lesions in 975 oral and maxillofacial pathology specimens, submitted for diagnosis at Tripoli Medical Centre over 17 years period (1997-2013).
MATERIALS AND METHODS
This study was approved by Libyan International Medical University Ethical Committee and data acquisition was supervised by the head of oral and maxillofacial surgery unit at Tripoli Medical Centre.
Inclusion criteria were all histopathological reports of benign orofacial specimens referred to the oral and maxillofacial surgery unit at Tripoli Medical Centre between 1997 and 2013. Case files with missing patient information or inconclusive diagnoses were excluded from the study.
Classification Criteria
Specimens were compiled into 9 diagnostic categories according to their histological presentation as following: skin and mucosal pathology, gingival and periodontal pathology, odontogenic cysts, salivary gland pathology and tumors benign tumors, bone pathology, odontogenic tumors, non odontogenic cysts and miscellaneous. The miscellaneous group contained diseases that could not be placed into any other diagnostic category.
RESULTS
During the 17 years period, a total of 1385 histopathological specimens were received from the oral and maxillofacial surgery unit at Tripoli Medical Centre, 83 cases were excluded due to incomplete data acquisition or unclear diagnosis. Of the remaining 1302 specimens, 975(74.88%) were of benign conditions and 327(25.12%) were of malignant conditions. Fig. (1) shows the distribution of diagnoses according to their histological grouping.

Distribution of diagnoses according to histological grouping.
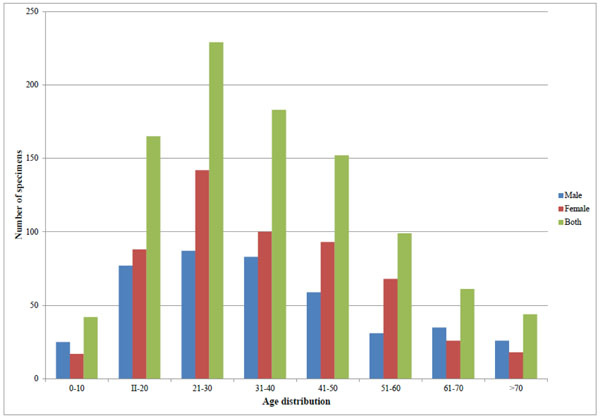
The distribution of age groups as related to gender.
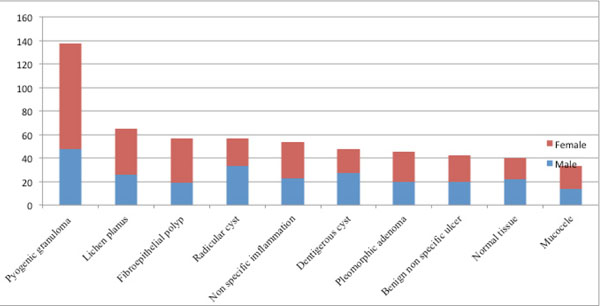
The 10 most frequent diagnoses.
Distribution of diagnoses according to the histological grouping.
| Skin and mucosal pathology | |||||
|---|---|---|---|---|---|
| Diagnosis | Number | Male | Female | Mean Age | % of group |
| Lichen planus | 65 | 26 | 39 | 44.98 | 29.14 |
| Fibroepithelial polyp | 57 | 19 | 38 | 38.4 | 25.65 |
| Chronic non specific inflammation | 54 | 23 | 31 | 37.98 | 24.21 |
| Discoid lupus erythematosus | 10 | 4 | 6 | 43.3 | 4.48 |
| Pemphigus vulgaris | 8 | 2 | 6 | 45.87 | 3.58 |
| Actinic keratosis | 5 | 4 | 1 | 68.8 | 2.24 |
| Focal epithelial hyperplasia | 4 | 4 | 0 | 33.5 | 1.79 |
| Compound nevus | 4 | 3 | 1 | 40 | 1.79 |
| Seborrheic keratosis | 4 | 3 | 1 | 55.5 | 1.79 |
| Leukoplakia | 3 | 2 | 1 | 61 | 1.34 |
| Solar elastosis | 2 | 0 | 2 | 60 | 0.89 |
| Trichoepithelioma | 2 | 1 | 1 | 31 | 0.89 |
| Lichenoid reaction | 2 | 1 | 1 | 28.5 | 0.89 |
| Hydrocytoma | 1 | 0 | 1 | 63 | 0.44 |
| Erythema multiforma | 1 | 0 | 1 | 26 | 0.44 |
| Aphthous ulcer | 1 | 1 | 0 | 14 | 0.44 |
| Total | 223 | 93 | 130 | 100 | |
| Gingival and periodontal pathology | |||||
| Diagnosis | Number | Male | Female | Mean Age | % of group |
| Pyogenic granuloma | 137 | 48 | 89 | 33.93 | 71.35 |
| Peripheral giant cell granuloma | 25 | 6 | 19 | 36.08 | 13.02 |
| Plasma cell gingivitis | 9 | 1 | 8 | 41.33 | 4.68 |
| Acute Periodontal abscess | 7 | 4 | 3 | 44.28 | 3.64 |
| Inflammatory gingival hyperplasia | 6 | 3 | 3 | 31 | 3.15 |
| Chronic gingivitis | 4 | 2 | 2 | 41.25 | 2.08 |
| Peripheral ossifying fibroma | 4 | 0 | 4 | 33 | 2.08 |
| Total | 192 | 64 | 128 | 100 | |
| Odontogenic cysts | |||||
| Diagnosis | Number | Male | Female | Mean Age | % of group |
| Radicular cysts | 57 | 33 | 24 | 31.78 | 49.17 |
| Dentigerous cysts | 48 | 27 | 21 | 30.09 | 41.37 |
| Residual cysts | 6 | 6 | 0 | 24 | 5.17 |
| Calcifying odontogenic cyst | 2 | 2 | 0 | 19 | 1.71 |
| Lateral periodontal cyst | 1 | 0 | 1 | 30 | 0.87 |
| Gingival cyst | 1 | 0 | 1 | 20 | 0.87 |
| Glandular odontogenic cyst | 1 | 1 | 0 | 40 | 0.87 |
| Total | 116 | 69 | 45 | 100 | |
| Diagnosis | Number | Male | Female | Mean Age | % of group |
| Salivary glands pathology and tumors | |||||
| Diagnosis | Number | Male | Female | Mean Age | % of group |
| Pleomorphic adenoma | 45 | 20 | 25 | 37.86 | 37.81 |
| Mucocele | 33 | 14 | 19 | 20 | 27.73 |
| Chronic sialadenitis | 23 | 12 | 11 | 41.26 | 19.32 |
| Ranula | 6 | 2 | 4 | 32.83 | 5.04 |
| Sjogren’s syndrome | 4 | 0 | 4 | 65 | 3.36 |
| Warthin tumor | 4 | 3 | 1 | 46 | 3.36 |
| Salivary gland hyperplasia | 2 | 1 | 1 | 20.5 | 1.7 |
| Salivary calculi | 1 | 0 | 1 | 17 | 0.84 |
| Acute parotitis | 1 | 0 | 1 | 13 | 0.84 |
| Total | 119 | 52 | 67 | 100 | |
| Benign tumors [excluding salivary gland tumors] | |||||
| Diagnosis | Number | Male | Female | Mean Age | % of group |
| Fibroma | 21 | 13 | 8 | 29.78 | 20.58 |
| Squamous cell papilloma | 18 | 4 | 14 | 39.33 | 17.64 |
| Hemangioma | 15 | 8 | 7 | 32.06 | 14.7 |
| Lipoma | 12 | 3 | 9 | 43.18 | 11.76 |
| Neurofibroma | 7 | 4 | 3 | 26.14 | 6.9 |
| Verruca vulgaris | 6 | 4 | 2 | 59.66 | 5.88 |
| Lymphangioma | 5 | 2 | 3 | 24.2 | 4.9 |
| Myofibroma | 5 | 0 | 5 | 35.6 | 4.9 |
| Schwannoma | 3 | 3 | 0 | 36.33 | 2.94 |
| Keratoacanthoma | 2 | 1 | 1 | 28 | 1.96 |
| Osteoma | 2 | 1 | 1 | 26.5 | 1.96 |
| Leiomyoma | 2 | 0 | 2 | 15 | 1.96 |
| Teratoma | 1 | 0 | 1 | 30 | 0.98 |
| Angiofibroma | 1 | 0 | 1 | 52 | 0.98 |
| Myoepithelioma | 1 | 1 | 0 | 24 | 0.98 |
| Xanthogranuloma | 1 | 1 | 0 | 23 | 0.98 |
| Total | 102 | 45 | 57 | 100 | |
| Miscellaneous | |||||
| Diagnosis | Number | Male | Female | Mean Age | % of group |
| Benign non specific ulcer | 42 | 20 | 22 | 54.19 | 41.58 |
| Normal Tissue | 40 | 22 | 18 | 40.17 | 39.6 |
| Chelitis granulomatosis | 5 | 2 | 3 | 34.8 | 4.96 |
| Abscess | 3 | 1 | 2 | 65 | 2.97 |
| Periapical granuloma | 3 | 2 | 1 | 33.66 | 2.97 |
| Diagnosis | Number | Male | Female | Mean Age | % of group |
| Miscellaneous | |||||
| Sarcoidosis | 2 | 1 | 1 | 23 | 1.98 |
| Tuberculosis | 2 | 0 | 2 | 47 | 1.98 |
| Histiocytoma | 2 | 2 | 0 | 3 | 1.98 |
| Chronic candidiosis | 2 | 1 | 1 | 52 | 1.98 |
| Total | 101 | 51 | 50 | 100 | |
| Bone pathology | |||||
| Diagnosis | Number | Male | Female | Mean Age | % of group |
| Central giant cell granuloma | 17 | 4 | 13 | 35.62 | 29.31 |
| Ossifying fibroma | 16 | 6 | 10 | 22.81 | 27.59 |
| Osteomyelitis | 12 | 6 | 6 | 39.08 | 20.69 |
| Fibrous dysplasia | 11 | 3 | 8 | 20 | 18.97 |
| Aneurysmal bone cyst | 1 | 1 | 0 | 23 | 1.72 |
| Paget disease | 1 | 0 | 1 | 50 | 1.72 |
| Total | 58 | 20 | 38 | 100 | |
| Odontogenic tumors | |||||
| Diagnosis | Number | Male | Female | Mean Age | % of group |
| Ameloblastoma | 21 | 8 | 13 | 36.75 | 43.74 |
| Odontogenic keratocysts | 14 | 5 | 9 | 28.57 | 29.15 |
| Odontogenic myxoma | 5 | 2 | 3 | 26.8 | 10.41 |
| Squamous odontogenic tumor | 3 | 1 | 2 | 19.33 | 6.25 |
| Adenomatoid odontogenic tumor | 3 | 2 | 1 | 28.66 | 6.25 |
| Calcifying epithelial odontogenic tumor | 1 | 1 | 0 | 30 | 2.1 |
| Complex odontome | 1 | 0 | 1 | 47 | 2.1 |
| Total | 48 | 19 | 29 | 100 | |
| Non odontogenic cysts | |||||
| Diagnosis | Number | Male | Female | Mean Age | % of group |
| Sebaceous cyst | 5 | 4 | 1 | 41.6 | 31.25 |
| Nasolabial cyst | 4 | 1 | 3 | 33 | 25 |
| Epithelial inclusion cyst | 4 | 3 | 1 | 54.5 | 25 |
| Nasopalatine cyst | 2 | 2 | 0 | 25.5 | 12.5 |
| Branchial cyst | 1 | 0 | 1 | 21 | 6.25 |
| Total | 16 | 10 | 6 | 100 | |
Fig. (2) shows the distribution of age groups as related to gender. Of the 975 benign conditions, 423 were of males and 552 were of females (male: female ratio: 0.76:1). Age of biopsied patients ranged from 1 to 95 years (mean 36.3 ± 18.32 years). The distribution of diagnoses according to histological grouping is shown in Table 1.
Overall, pyogenic granuloma was the most predominant diagnosis (14.05%) followed by lichen planus (6.66%) and radicular cysts (5.84%). The most frequent pathology in each category was as following: skin and mucosal pathology: Lichen planus (65 specimens); gingival and periodontal pathology : pyogenic granuloma (137 specimens); odontogenic cysts: radicular cyst (57 specimens); salivary gland pathology and tumors: pleomorphic adenoma (45 specimens); benign tumors: fibroma (21 specimens); miscellaneous: benign non specific ulcer (42 specimens); bone pathology: central giant cell granuloma (17 specimens); odontogenic tumors: ameloblastoma (21 specimens); non odontogenic cysts: sebaceous cyst (5 specimens).
The 10 most frequent diagnoses are shown in Fig. (3); these comprised 578, nearly 60% of all specimens. Pyogenic granuloma was the most predominant diagnosis (14.05%) followed by lichen planus (6.66%) and radicular cysts (5.84%).
DISCUSSION
Most previous investigations concentrate on studying a single type of benign oral diseases or a group of closely related ones. This study investigates all benign oral lesions in a group of Libyans. Information obtained from similar surgical pathology reports are of great values to oral surgeons facing benign oral diseases on daily basis. Furthermore, results of such surveys may constitute a baseline for large-scale population based investigations.
Most published studies investigating the oral lesions are either limited to a specific disease entity like odontogenic cysts [3], tongue lesions [5], odontogenic tumors [4, 16-18] or salivary gland tumors [19]; or limited to a specific population group such as children [20] elderly [21] or military [22]. Therefore, direct comparisons with previous reports are difficult.
The number of benign orofacial specimens histologically analyzed at Tripoli Medical Centre over 17 years period accounted for 70.4% (975 specimens) of all submitted specimens. Overall, there was a slightly higher tendency for orofacial lesions to occur in females, with the male: female ratio at 0.76:1. This was also reported by Tay [11], Jones and Franklin [12] and Torres-Domingo et al. [23]. However, males were more commonly affected by certain conditions; these include odontogenic and non odontogenic cystic lesions.
Skin and Mucosal Pathology
This category contained the highest number of biopsied specimens. Lichen planus was ranked the most predominant diagnosis among the skin and mucosal lesions, and the second most frequently diagnosed pathology with 65 (6.6%) specimens. Similar results were reported by Rossi and Hirsch [8], Tay [11], Jones and Franklin [12] and Cury et al. [24]. However, Sixto-Requeijo reported substantially higher number of cases [10]. There was a higher tendency for this disease to occur in females as reported in previous studies [12, 23]. This is probably due to the hormonal changes and stress among females [23]. Fibroepithelial polyp is believed to be a non specific focal hyperplasic reaction of the lamina propria in response to chronic irritation. In our study, it accounted for 5.84% of the total biopsies, which is significantly lower than reported by Jones and Franklin and others [12, 13]. As reported in previous results [12, 13], fibroepithelial polyps were almost as twice in females as in males.
Gingival and Periodontal Pathology
Within this category, Pyogenic granuloma was the most predominant diagnosis and it amounted to 14.01% of the total. In most western studies, including those from United Kingdom [12], Singapore [11] and Brazil [25], it made up only 1.8-2.43% of the overall biopsies. However, our results were similar to biopsied tissues from Jordanian [13] and Yemeni populations [26]. The high female predilection for pyogenic granuloma may reflect the effect of estrogen and progesterone hormones in pregnancy on the pathogenesis of the condition, it was suggested that these hormones make the gingival tissue more susceptible to chronic inflammation caused by plaque and calculus [26]. In the present study, there was high frequency of pyogenic granuloma in females in child bearing age (mean age: 33.93).
Cystic Lesions
Both odontogenic and non odontogenic cysts were more prevalent among males. Radicular and dentigerous cysts were the most commonly diagnosed lesions in the odontogenic cysts category accounting for 49.17% and 41.37%, respectively. These findings were also reported in other studies from Libya [1], Singapore [27] and Canada
[17]. Radicular cysts comprised 5.84% of all biopsied specimens, ranked the third most common diagnosis. It was ranked the forth most frequent diagnosis (5.3%) in the United Kingdom [12].
Odontogenic keratocysts including parakeratinized and orthokeratinized types were reclassified as keratocystic odontogenic tumors and jaw cysts with keratinisation according to the new WHO guidelines of 2005 [17]. Keratocystic odontogenic tumors comprised 1.43% of the total submitted specimens, this is substantially lower than the figures found in the United Kingdom [12], Mexico [28] and Germany [29] but similar to those reported in a previous study in Libyan population [30].
Benign Tumors
The ratio of benign to malignant tumors is approximately 0.3:1, Fibroma was the most frequent diagnosis in this category, supporting previous findings in the literature [2, 10, 23, 25]. In contrast, Jones and Franklin reported high occurrence of squamous cell papilloma and low proportions of fibromas [12]. The frequency of fibroma was higher in males, a result contrasting with previous studies [2, 25, 21].
Odontogenic Tumors
Odontogenic tumors accounted for only 3.48% of all submitted specimens; which was similar to findings by Jones and Franklin [12], Delay [16], Bhaskar [31] and Regezi [32] and this tends to confirm that these lesions are rare. Bhaskar [32] reported a preponderance of odontogenic tumours at 2.37% of all submitted specimens, while Kim and Ellis [33] reported that of 847 cases referred to the Armed Forces Institute of Pathology; only 53.4% (460 cases) were correctly identified as dental follicles and/or dental papillae; common misdiagnosis included odontogenic myxoma and other odontogenic tumours. The study by Kim and Ellis emphasized the importance of referral of such lesions to an oral and maxillofacial pathologist.
Our results showed that ameloblastoma was the most predominant odontogenic tumor, which is similar to that found by Tay [16] and Jones and Franklin [12] but differs from other studies. For example, ameloblastoma are more common in the African [17] and Chinese [18] whereas odontomas appear to be more common in Canada [16] and Mexico [28].
Salivary Gland Pathology and Benign Tumors
Mucocele, chronic sialadenitis and ranula were the most predominant diseases; similar results were reported by Jones and Franklin [12]. Mucocele made up 3.38% of the total specimens, compared with 3.4%, 4.3% and 11.6% from other findings in the literature [12, 34], it was found to be the most frequent salivary gland lesion with predominance in children and young adults.
Benign tumors of salivary glands included pleomorphic adenoma and warthin tumor. Pleomorphic adenoma, a benign tumor of epithelial origin, made 4.6% of the total specimens. This was a relatively higher percentage than the figures reported by Jones and Franklin, and others [10, 21]. It was found to be the most predominant benign tumor in major and minor salivary glands [10, 12, 21, 35].
Bone Pathology
Central giant cell granuloma and ossifying fibroma were the most predominant diagnoses in this group, both of which showed female predilection. These results were similar to studies from eastern Libya [4] and Kuwait [14]. Other studies [10, 12] showed lower frequencies of these lesions and higher prevalence of other pathologies like osteoarthrosis, exostosis and BRONJ.
It has been demonstrated that factors such as smoking, alcohol consumption, socioeconomic status and prosthetic use can be associated with the occurrence of oral lesions [36]. Unfortunately, these factors are not often considered when histopathological evaluation is required. Since this information was not recorded in our laboratory reports, we were unable to evaluate its effect on the pathogenesis of benign oral lesion.
CONCLUSION
The number of investigated benign orofacial specimens reported at Tripoli Medical Centre over 17 years period was 975. Pyogenic granuloma, lichen planus, fibroepithelial polyp and radicular cyst were the most frequent diagnoses. The relative frequencies reported in our results were comparable to similar studies in the literature and to those reported from eastern part of Libya. These results can be used as a baseline for further nationwide population-based surveys of orofacial diseases in Libyan population.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
None declared.

