
Optimizing Non-surgical Endodontic Retreatment: A 3D CBCT Quantification of Root Canal Bioceramic Filling Material Removal
Abstract
Objective
This study aims to quantify and compare the volume of residual bioceramic root canal filling material after different non-surgical endodontic retreatment procedures.
Methods
Fifty single-rooted teeth underwent primary root canal treatment using the ProTaper system and BioRoot RCS. Non-surgical retreatment employs ProTaper files D1, D2, D3, F3 (n=50). For Group A (n=10), retreatment procedures conclude on the X3 file and additional ultrasonic energy (Group B, n=10), the Self-Adjusting File (SAF) system (Group C, n=10), endodontic solvents (Group D, n=10), and chelator (Group E, n=10). Detailed procedures outline each group's retreatment protocol. Residual root canal filling material volumes are precisely evaluated in mm3 using 3D CBCT and specific software.
Results
Significant variations in residual material volume are observed among the groups, with ultrasonic energy demonstrating superior efficacy. Statistical analyses affirm the impact of different methodologies on material removal. The SAF system also shows promise, although limited literature addresses its impact on Bioceramic Sealers. Conversely, no significant advantage is observed with endodontic solvents or chelators.
Conclusion
This in vitro study underscores the efficiency of ultrasonic energy in material removal, supported by the existing literature. The SAF system exhibits promise, contributing to the evolving landscape of endodontic practice. However, endodontic solvents and chelators show limited efficacy in bioceramic sealer removal. The study advocates for the integration of 3D CBCT in endodontic research, offering precise measurements and insights into bioceramic material removal techniques.
1. INTRODUCTION
Endodontic therapy stands at the forefront of preserving natural dentition by meticulously addressing infections within the intricate root canal system [1, 2]. The crux of successful root canal treatment lies in the thorough eradication of diseased pulp tissue and the precise obturation of the canal space [3, 4]. Through the annals of dental history, various materials and techniques have been harnessed for root canal filling, each presenting a unique tapestry of advantages and challenges [5].
Despite the strides in endodontic procedures, the complete removal of root canal-filling material remains an enduring challenge [6, 7]. Lingering residual material within the root canal space poses a perpetual threat to the long-term success of treatment, ushering in the specter of persistent infections, periapical pathology, and diminished treatment outcomes [8, 9]. Traditional radiographic methods, while valuable, grapple with limitations in delivering accurate three-dimensional assessments of the root canal space and the remnants of filling material [10].
In recent times, Cone Beam Computed Tomography (CBCT) has emerged as a transformative diagnostic tool in endodontics. It bestows the clinician with the prowess of three-dimensional visualization of the tooth and its surrounding structures. This technological marvel transcends the confines of traditional radiography, offering unparalleled insights into the spatial distribution of residual root canal-filling material [11]. CBCT empowers clinicians to scrutinize the adequacy of obturation and identify potential concerns that might impede the triumph of the treatment [12].
The remaining obturating materials operate as a mechanical barrier, detaining the intracanal medicaments to access dentinal tubules, lateral canals and isthmi. In order to allow irrigants to reach every part of the root canal system during the retreatment procedure, all the filling remnants should be thoroughly removed [7].
In light of the persistent challenge of complete root canal filling material removal and the limitations of traditional radiographic methods in accurately assessing residual material, there arises a critical need for advanced diagnostic techniques that offer precise three-dimensional visualization. Recognizing this gap in current endodontic scientific literature, researchers seek to find an effective tool, such as automated computer software, for precise and objective evaluation of the volume of residual root canal filling material. Regardless of the scoring system used, if the research method requires human input, it is inevitable that there will be an element of subjectivity and performance bias [ 13 ]. Through this research endeavor, we contribute to the ongoing advancement of endodontic practice.
2. AIM
This study aims to quantify and compare the volume of residual bioceramic root canal filling material after different non-surgical endodontic retreatment procedures.
3. MATERIALS AND METHODS
For this in vitro study, 50 single-rooted single canal teeth (Weine Type 1) were used. Inclusion criteria: freshly extracted caries-free human mandibular premolars with single, straight root canals, curvature <5° were selected on the basis of preliminary CBCT evaluation. Exclusion criteria: teeth with previous root canal treatment, calcifications in canal, dental caries, external and/or internal resorption. Teeth were extracted due to orthodontic reasons from young patients (18-42 years of age) who remained anonymous.
This study was approved by the Ethical Committee of the Medical University of Plovdiv, Plovdiv, Bulgaria (2021_RKNE_078C212D87f_). We confirm that the Helsinki Declaration has been followed.
The number of specimens was based on previous studies [ 7 ]. This study enrolls teeth meeting specific inclusion and exclusion criteria. Inclusion criteria consist of single-rooted teeth with single canals. Prior to primary endodontic treatment, all included teeth underwent crown removal using a diamond separator to obtain 12 mm samples measured from the apex coronally.
Primary root canal treatment was performed starting with preparing a standard endodontic cavity and negotiation of the root canal with K-file #10. The glide path wasprepared with K-files #10, #15, and #20. Shaping of the root canal wasachieved by using the Pro Taper Gold system (PTG), according to the manufacturer’s instructions, until the apical foramen reached twice with the F2 file. Sodium hypochlorite 2,5% wasused for irrigation during the shaping, and 17% EDTA wasused for final irrigation. Lastly, the canals wereflushed with saline and dried using calibrated paper points (PTG). BioRoot RCS (Septodont) endodontic sealer was mixed according to the manufacturer’s instructions and introduced in the root canal using the Lentulo spiral. The calibrated F2 gutta percha point wascoated with a sealer and introduced slowly to the working length. A heated plugger wasused to cut the gutta percha point at the level of the orifice and gently pack it apically. The endodontic cavities were sealed with temporary filling Coltosol F (Coltene). After root canal obturation, specimens underwent X-ray scanning to access root canal filling (Hyperion X9, MyRay®). Teeth were then stored in a thermostat at 370C and 100% humidity for 4 weeks for proper setting of the sealer.
After removal of the temporary filling, root canal retreatment wasperformed using D-files (Pro Taper Retreatment) sequentially until the apical foramen reached with file D3. Then, in order to complete the secondary preparation of the root canal, the F3 file (PTG) wasused until the apical foramen is reached twice. Irrigation was performed only with sodium hypochlorite during the retreatment and saline as a final solution (n=50).
For this experiment, the samples wererandomly assigned into five subgroups, depending on the additional processing of the root canal.
In Group A (n=10), the preparation concluded upon reaching the working length with F3 files (30.09). Each file was discarded after use in five root canals. No supplementary cleaning technique wasused (control group).
For Group B (n=10), after completing the preparation, passive ultrasonic activation of the irrigation solution was performed using ProUltra Endo Tips #6, #7, and #8 (Dentsply Sirona). Sequential activation involved 17% EDTA (for 1 minute) and 2.5% sodium hypochlorite (for 2 minutes), with intermittent irrigation using a saline solution. Finally, the root canals weredried using sterile paper points.
In Group C (n=10), after reaching the working length with an F3 file, additional preparation was performed using a Self-Adjusting File (SAF, ReDent, Nova, Ra’anana, Israel). The SAF file required a preprepared smooth path up to size 20.02 for straight canals and 20.04 for curved canals. If the file didnot reach the working length passively, the smooth path wascorrected. The SAF files were used for 2 minutes in each canal under continuous irrigation with 2.5% sodium hypochlorite at a flow rate of 4 ml/min. The canal wasrinsed with saline solution, and the SAF file was used until reaching the working length.
For Group D (n=10), SAF preparation was combined with chloroform solvent. After 2 minutes of SAF work under continuous irrigation with 2.5% sodium hypochlorite, the canal wasdried, and a drop of chloroform wasintroduced before reinserting the SAF file. The peristaltic pump wasturned off, and simultaneous irrigation was halted. SAF movements weresimilar to Group C, but without simultaneous irrigation. SAF work in the presence of chloroform lasted 1 minute per canal. After the specified time, the canal was rinsed with saline solution and dried.
For Group E (n=10), the methodology wasidentical to Group D, with the only difference being the use of 40% citric acid instead of chloroform as a solvent.
Following the root canal filling material removal procedures, the experimental samples underwent three-dimensional CBCT to measure the volume of residual bioceramic sealer (BCS) in the root canal. Experimental samples (n=50) werearranged on purpose-built platforms constructed from non-radiopaque material (polystyrene). Each platform wassecurely fixed to the computerized cone-beam tomograph Hyperion X9 (MyRay®) and scanned.
Following scanning, the acquired images were processed using the dedicated iRys Viewer v8.0 software (MyRay®). For volume measurements of the residual canal filling material, the free version of Horos® (v3.3.6) software was employed. It enabled objective segmentation based on voxel values (density) derived from cone-beam imaging [14]. Upon importing the DICOM directory and switching to a sagittal view from the Region of Interest (ROI) menu, the “Growing Region Segmentation” option was selected. In a subwindow, the appropriate algorithm – “Threshold (lower/upper bounds)” – along with the voxel value for segmentation werechosen.
To differentiate the canal filling material from dental structures, voxel density values weremeasured in various zones. The voxel value representing the weakest shadow (the most saturated black, where no scanned object was present) was”-1000,” and the values corresponding to varying shadow intensity ranged widely. According to ISO 6876:2012, the requirement for root canal filling materials wasto possess radiopacity equivalent to a minimum of 3 mm aluminum [15].
Therefore, a threshold density value must be determined, serving as the boundary between the strong shadows of dentin and the even stronger shadows corresponding to the canal-filling material (Fig. 1).
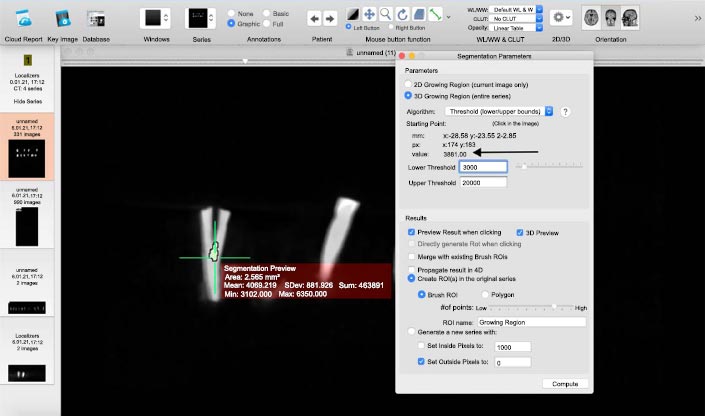
The highest density value for dentin measured in the study was2810, while the lowest density value for root canal filling material was3004. By setting parameters with a lower limit of 3000 and an upper limit of 20000, we successfully segmented only the root canal filling material, excluding dental structures from the measurement.
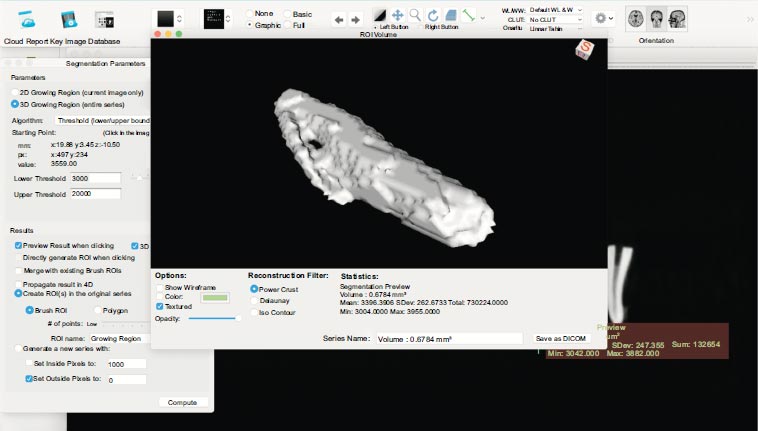
Digital values for the volume (in mm3), mean voxel density in the segmented volume, and standard deviation wererecorded for each sample (Fig. 2). Average values for each group werecalculated, and the data were statistically processed using the Kruskal-Wallis test followed by Dunn’s Multiple Comparison tests.
Statistical analyses ANOVA and Pairwise Comparison Analysis were performed to compare the remaining amount of root canal filling material at a 95% level of confidence, with the significance level established at p<0.05.
4. RESULTS
The mean volume of residual bioceramic root canal filling material after the non-surgical endodontic retreatment procedurefor all samples was1.753856 mm3 (SD = 4,1074812). In the control group (Group A), the investigation revealed the highest amount of residual root canal filling material, with an average of 4.87144 mm3 (SD = 7,2208339).Following closely, the group employing the innovative SAF (Self-Adjusting File) system (Group C) demonstrated the second highest amount of residual material, measuring 2.18957 mm3 (SD = 4,6867511). The introduction of chloroform to the SAF system (Group D) resulted in an improvement in BCS removal - 0.92138 mm3 (SD = 0, 7744598), while the addition of a chelator for Group E demonstrated a mean value of 0.6755 mm3 (SD = 1,0364033). Remarkably, the group subjected to ultrasonic energy (Group B) exhibited the lowest quantitative mean values of residual bioceramic root canal filling material - 0.11139 mm3 (SD = 0,0754987).
The subsequent sections delve into the detailed statistical comparison and provide a comprehensive understanding of the observed variations between the control and each of the experimental groups.
When comparing the volume of residual bioceramic root canal filling material after different non-surgical endodontic retreatment protocols, statistically significant differences were found between the control group (Group A) and Group B; control group (Group A) and Group C and Group B and group C (p<0.05). No statistically significant differences were found between Group D and Group E, nor between each of them and the control group (Group A) (p>0.05). No statistically significant differences werefound when a comparison was made between groups B, C, D and E (p>0.5).
5. DISCUSSION
In this study, all the specimens revealed remnants of root canal-filling material. The comparative analysis of residual root canal filling material across the diverse experimental groups unravels intriguing insights into the effectiveness of various methodologies in non-surgical endodontic retreatment.
In our study, the control group (Group A) emerged as the cohort with the highest residual material, sharply contrasting Group B, where ultrasonic energy wasapplied, exhibiting the least amount. This dissimilarity bears statistical significance (p < 0.05), emphasizing the notable impact of ultrasonic energy on minimizing residual material within the root canal [16].
The successful utilization of ultrasonic energy in endodontic retreatment dates to Wilcox's seminal work in 1989 [17]. Notably, our findings align with Cavenago's observations of cleaner dentin walls with ultrasonic tips, even though their study does not involve Bioceramic Sealers, utilizing only epoxy resin-based AH Plus [16]. Furthermore, our study reinforces Pedullà's findings, indicating a significant difference in BioRoot RCS removal between the ultrasonically activated irrigant group and the non-ultrasound group (p < 0.05) [8].
Group C, employing the SAF system, ranked second in residual material quantity. The SAF file's adaptive shape to the canal contributes to effective BCS removal from the canal walls [18, 19]. A substantial difference was found between the SAF group (Group C) and the control group (Group A) (p < 0.05). While the positive effect of SAF in removing endodontic sealers from the canal walls has been established, notably in our study, no existing literature is found regarding the impact of SAF on the removal of bioceramic endodontic sealers.
A statistically significant difference was identified between Groups B and C (p < 0.05). Group B involved the activation of the irrigation solution through ultrasonic energy, while Group C employed the SAF system without the addition of a solvent. Despite the SAF file adapting its shape to the canal, it proves less effective compared to ultrasonic energy. Ultrasonics induced microexplosions in the fluid within the root canal, transmitting energy to the residual material and facilitating its detachment. This mechanism wasparticularly effective in the straight portion of the root canal, where the ultrasonic tip could directly influence the material on the wall, leading to its dislodgment and effective removal. In the apical zone, beyond the curvature of the canal, the ultrasonic tip's indirect energy transmission through the fluid (irrigant) wasthe sole mechanism [16, 20]. Notably, no other studies comparing the effects of ultrasound and the SAF system on the removal of canal filling material from the canal wall wereidentified in the available literature.
No statistically significant differences werefound between Groups D and E or between either of them and the control group (p > 0.05). The adjuncts, chloroform (in Group D) and citric acid chelator (Group E), demonstrated efficacy in aiding Bioceramic Sealer (BCS) removal, with mean values lower than those of the control group, although lacking statistical significance (p>0.05). The effect of chloroform on the removal of bioceramic sealers has been studied by several authors [21-25]. It proves effective in softening some hybrid sealers containing a resin component, such as MTA Filapex and GuttaFlow, but not towards true bioceramic sealers composed exclusively of calcium silicates. In our experiment, we used a genuine (synthetic tricalcium silicate) bioceramic endodontic sealer – BioRoot RCS (Septodont). The absence of a resin component makes it resistant to organic solvents like chloroform. Yet, the results obtained show a higher degree of removal in this group compared to the control. The addition of chloroform to the SAF system protocol (Group D) did not yield a statistically significant difference compared to the SAF group without a solvent (Group C). This is attributed to the extended working time of the SAF file in the canal. In the group without chloroform, the SAF file is activated for 2 minutes in the canal, while in Group D, after adding chloroform, it is activated for an additional minute. This increased working time of the SAF file in the canal likely contributes to the lower absolute value of residual material in the chloroform group D.
The addition of a chelator (40% citric acid) also demonstrates a certain advantage in Bioceramic Sealer (BCS) removal. The mean value of residual material for the chelator group (Group E) is 0.6755 mm3, lower than the group using only SAF (Group C) and the group with SAF + chloroform (Group D). This difference is attributed to the additional working time of the SAF file and, in part, to the demineralizing action of the chelator. However, this observed difference lacks statistical significance (p > 0.05), leading to the conclusion that chelators, particularly 40% citric acid, do not significantly aid in the removal of bioceramic sealers from the canal wall. This result supports the conclusion drawn by Garrib that chelators are not beneficial in removing bioceramic sealer from the canal wall [26].
The use of chelators as adjuncts in the removal of the smear layer following instrumental treatment of the Root Canal (RC) has been explored extensively. Chelators bind to the calcium ions of the smear layer, maintaining them in a soluble calcium chelate stat [27]. Their effect on the removal of bioceramic sealer (TotalFill BC sealer, FKG) has been investigated by Garrib et al. In a recent study, they propose a conceptually new approach to the removal of Bioceramic Sealers (BCS) from the root canal. They focus on the chemical composition of bioceramic sealers, which are inherently hydraulic cement. In an in-vitro study, they apply a chelator (17% EDTA) and formic acid (HCOOH) in different concentrations (10% and 20%) and observe a positive effect of the latter on the removal of TotalFill BC sealer (FKG), with the best results obtained with a 10% formic acid solution. The authors explain this by the less aggressive action of the lower acid concentration. The use of 20% formic acid resulted in a reduction in dentin microhardness, with an insignificant difference in the degree of material removal between the two concentrations (p > 0.05). They find that 17% EDTA causes surface cracks in the material, but the quantity of detached calcium ions is less compared to 10% formic acid. The authors conclude that the chelator is effective in removing gutta-percha points coated with bioceramic particles but not bioceramic sealer [26].
In our current study, we employed a different chelator - 40% citric acid. In our view, the high percentage of the solution has the potential to bind to the material's calcium ions and thus facilitate its softening. Our working hypothesis was that 40% citric acid, in combination with the SAF system, would aid in the removal of the tricalcium silicate sealer BioRoot RCS from the root canal wall. However, the obtained results reject this hypothesis and support Garrib's conclusion. Although the endodontic sealer we used is different, it shares the same chemical nature - hydraulic tricalcium silicate cement, and the effect of the chelator on it is analogous.
The addition of a chelator (40% citric acid) to the SAF system protocol in the endodontic retreatment procedure is an original methodology not previously tested. Interestingly, in this group, we observe more remaining sealers compared to the ultrasonic group (group B). Despite the SAF file working an additional minute in the RC after the application of the chelator, the amount of residual sealer is greater compared to the ultrasonic group (p < 0.05). These results are attributed to the high effectiveness of ultrasound in the coronal section of the RC, which is typically straight and accessible to ultrasonic tips.
No other experiments combining the SAF system and a chelator in the context of bioceramic sealer removal from the RC wall are identified in the scientific literature.
Our in vitro study may face a weakness, such as direct implementation of the results in clinical practice, while the strengths include novelty, relevance, methodological rigor, comprehensive analysis and clear presentation.
CONCLUSION
Within the limitation of the study, it can be concluded that three-dimensional cone-beam computed tomography (3D CBCT), accompanied by a specialized DICOM software (Horos®), proves to be a viable and effective methodology for objective quantifying of residual root canal filling material in in vitro settings. Although root canal filling material was detected in every specimen, our findings suggest that endodontic solvents (chloroform) and chelators (40% citric acid) do not play a substantial role in influencing the removal of bioceramic sealers from the canal wall during non-surgical retreatment. On the contrary, both the SAF system and the application of ultrasonic energy significantly contribute to the enhanced removal of the studied root canal sealer from the canal wall in the context of non-surgical retreatment of the root canal.
LIST OF ABBREVIATIONS
| CBCT | = Cone Beam Computed Tomography |
| BCS | = Bioceramic Sealer |
| SAF | = Self-Adjusting File |
| PTG | = Pro Taper Gold System |
| EDTA | = Ethylenediaminetetraacetic Acid |
| DICOM | = Digital Imaging and Communications in Medicine |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethical Committee of the Medical University of Plovdiv, Plovdiv, Bulgaria (2021_RKNE_078C212D87f_).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available within the article.

