All published articles of this journal are available on ScienceDirect.

Intraoral Retrieval of a Displaced Impacted Lower Third Molar into Submandibular Space: A Case Report
Abstract
Background
The displacement of the impacted lower third molar into Submandibular Space is a rare complication during impaction surgery. Removal of a displaced impacted molar from the submandibular space can be complicated by poor visibility and limited accessibility.
Objective
This study aimed to evaluate the intraoral approach in the retrieval of displaced impacted lower molar into submandibular space.
Case Presentation
The present case is of a 50-year-old male patient who underwent a surgical procedure to extract the impacted lower third molar about a month ago, which led to its displacement into the submandibular space. The location and angulation of the molar were determined through radiographic examination using panoramic imaging and computed tomography. The displaced molar was retrieved surgically under general anesthesia using the intraoral approach. The patient was followed-up for 1 month regularly. The postoperative symptoms were limited, including pain, swelling, and trismus. No numbness was observed in the tongue.
Conclusion
We concluded that the intraoral approach was a conservative and effective option for retrieval of displaced impacted mandibular third molars into submandibular space.
1. INTRODUCTION
The extraction of impacted lower third molars is one of the most common procedures in oral surgery [1]. However, several complications have been reported to occur intraoperatively or postoperatively [2]. During lower third molar removal, dental elements (tooth or root fragment) can be displaced to adjacent spaces that include submandibular space, sublingual space and ptery- gomandibular space [3, 4]. Such complications are uncommon during extraction, but it is not well-documented in the literature and the information about its incidence and management is limited [5, 6].
Risk factors for the displacement of the tooth into the submandibular space include anatomical factors and operator errors. Anatomical factors include a thin lingual plate and distolingual inclination of the tooth. Operator errors include uncontrolled excessive force, lack of experience, and insufficient clinical and radiographic assessment [6, 7].
The retrieval approaches for displaced impacted molar into the mandibular space depend on the location and severity of the displacement. The retrieval of a tooth that has been displaced into the submandibular space can be a complex process, and it is important to evaluate the appropriate treatment approach for each individual case. We discuss a case of intraoral retrieval of a displaced lower third molar into the submandibular space in this study.
2. CASE PRESENTATION
Written informed consent was obtained from the patient for publication of this study. A 50-year-old male patient reported to the Department of Oral and Maxillofacial Surgery at Tishreen University Hospital after 1 month of an unsuccessful surgical procedure for extraction of the right impacted third molar (Fig. 1). The patient's complaint was pain, swelling at the mouth’s floor, and trismus, which lasted for two weeks postoperatively. The clinical examination via palpation showed the absence of the lingual cortical plate, with the possibility of palpating the displaced molar at the floor of the mouth. The patient was advised an OPG (Fig.2) and CBCT radiography (Fig.3). 3D reformatted images of the CBCT scan showed the absence of a lingual cortical plate with the displacement of the third molar into the submandibular space. The displaced molar was in an inverted position (its crown to posterior) (Fig.3).


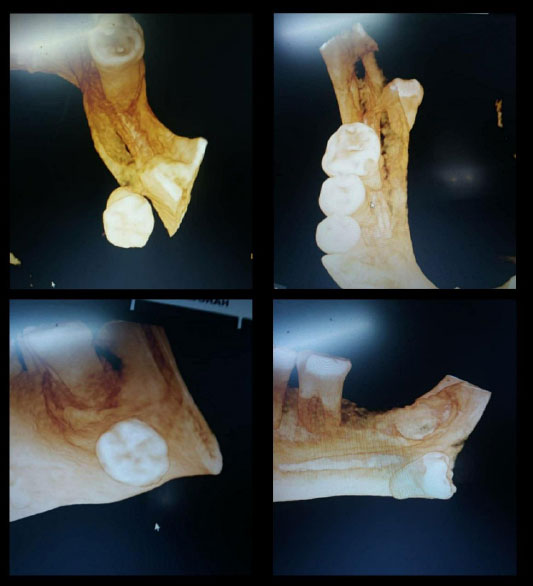

Under general anesthesia, a full thickness buccal flap was raised up to expose the surgical field. An intrasulcular incision was made lingually from the first premolar to the third molar area, and the fibrous tissues were bluntly dissected carefully using mosquito forceps. After the surgical site exposure, the displaced molar was not directly visible. The lingual flap was carefully retracted using a wooden tongue depressor wrapped in gauze to reduce the possibility of lingual nerve damage. The displaced third molar was palpated beyond the mylohyoid muscle, which was dissected to expose it. The molar was carefully removed using mosquito forceps (Fig.4), and the area was irrigated with normal saline. The incisions were closed with 3-0 silk sutures.
The patient was followed-up for 1 month regularly. The postoperative symptoms were limited, including pain, swelling, and trismus. No numbness was observed in the tongue.
3. DISCUSSION
Impacted molar surgery requires adequate clinical and radiographic examination to evaluate the level of difficulty and to avoid potential complications as much as possible. Third molar displacement into the submandibular space is a very rare complication and not easily expected, and sometimes it is difficult to avoid it when more than one risk factor is involved and the surgeon should not underestimate the surgery, no matter how easy it may seem [8, 9].
Displacement of impacted molars cannot be predicted with certainty, but some factors increase the possibility of this complication [6, 7]. In our case, we were informed by the general practitioner who attempted to extract the impacted molar by applying excessive force, in addition to insufficient bone removal from the buccal and distal aspects. It can be said that the anatomical factors (distolingual inclination of the tooth) and the operator errors (uncontrolled excessive force and lack of experience) have combined in our case and led to the molar displacement.
It is recommended to postpone the retrieval surgery for several weeks (unless the fragment is very clearly and easily seen to be grasped) to allow the fibrosis process to occur and stabilize the displaced molar (stabilization of the molar in a fibrous capsule) and prevent a further displacement in the cervical area. [8, 5]. Immediate removal of displaced molars may complicate the condition by moving them into adjacent spaces [10]. However, some authors consider immediate retrieval necessary to prevent the onset of life-threatening infections like cervicofacial infection or Ludwig’s Angina [11].
Determination of the exact location of the displaced molar is essential through clinical and radiographic examination [12]. In our case, Palpation was useful in determining the displaced third molar location and the amount of lingual plate injury. Clinical examination by palpation is also useful in selecting the appropriate retrieval approach [13].
Lingual nerve injury is a possible complication when raising a lingual flap (range between 0.6 and 22%); the incisions and retraction are possible causes of injury to the lingual nerve during mandibular third molar surgery [14]. Lingual nerve injury is usually temporary, and it typically resolves spontaneously within 6 months. To avoid this complication, the authors suggested the extension of the sulcular incision from the distal of the canine to the distal buccal of the mandibular second molar. This approach allows retraction of the lingual flap with minimal tension [15].
CONCLUSION
Based on our findings with the limitations of our case report, we concluded that the intraoral approach was a conservative and effective option for retrieval of displaced impacted mandibular third molars into submandibular space.
ETHICAL STATEMENT
This case report was approved by the Ethics Committee of Tishreen University Hospital, Lattakia, Syria (Ethical Permission No. 115 on 24-6-2023).
CONSENT FOR PUBLICATION
Written informed consent was obtained from the patient for publication of this study.
AVAILABILITY OF DATA AND MATERIALS
The data used to support the findings of this study are included in the article.
ACKNOWLEDGEMENTS
Declared none.

