All published articles of this journal are available on ScienceDirect.

Relationship of Self-perceived Stress and Expression of Salivary Cortisol in Relation to Gender and Academic Levels among Dental Students
Authors Info & Affiliations
Abstract
Purpose
Although cortisol is commonly regarded as the body's stress hormone, it also has a range of other effects on other biological functions. The aim of this prospective cohort's study was to examine the link between self-perceived stress and salivary cortisol expression in relation to gender and academic levels in a subgroup of dental students.
Material and Methods
151 students (79 males and 72 females) who provided written consent took part in this study. To explore the causes of self-perceived stress and divide the participants into Mild, Moderate, and High-stress categories, a self-administered stress questionnaire was employed. The enzyme-linked immunosorbent assay (ELISA) was utilized to quantify the level of cortisol present in saliva samples. Salivary cortisol levels, self-perceived stress, and demographic data, including age, gender, and educational attainment, were recorded for every participant. Chi-square and two-tailed Student's t-tests (0.05) were employed to analyze group comparisons.
Results
Female students responded more stressfully (P<0.05) to questions on decision-making issues, academic dishonesty, a hectic course load, a lack of downtime, the transition from the pre-clinic to the clinic, and the challenge of mastering fine manual dexterity. For male and female subjects, the mean & standard deviation of levels of cortisol were 1.54+0.41 and 1.28+0.45, respectively (p=0.000). At preclinical and clinical levels, the mean & standard deviation of levels of cortisol were 1.48+0.44 and 1.37+0.45, respectively (P=0.150).
Conclusion
Female students appeared to have a higher self-assessed stress level. Male students had significantly higher levels of salivary cortisol in comparison to female students. No significant differences were found for the levels of salivary cortisol at the preclinical and clinical academic levels.
1. INTRODUCTION
Stress is characterized as a living organism's generalized adaptive response to a disturbance. There are a number of stressors that have been recognized; they may be real or imagined, psychological or physiological [1]. Physiological stressors alter blood pressure, heart rate, waist-hip ratio, and body fat percentage, among other bodily functions. Tumor necrosis factor-alpha, cortisol, catecholamines, HDL, total cholesterol:HDL ratio, triglycerides, glycosylated hemoglobin, glucose levels, fibrinogen, D-dimer, and C-reactive protein are among the other biochemical concentrations [2]. While psychological stress may indirectly cause the onset or worsening of mental health disorders, hypertension, an elevated risk for cardiovascular disease, obesity, type 2 diabetes, worsening of chronic obstructive pulmonary disease or asthma, and increased risk of ulcerative colitis, among other things, as well as the deterioration of skin disorders like psoriasis [3].
Stress plays a significant part in the lives of many young adults and frequently leads to the experience of a variety of emotional problems [4]. Students are frequently under a lot of stress since they have to establish themselves in professional institutions and make decisions about their futures [5]. Their psychological and mental health is frequently directly impacted by the stress these young people go through. Stress levels can be influenced by a variety of circumstances, including family life, sexuality, moving, accidents and illnesses, autonomy, high self-expectations, competitive learning environments, and financial worries. All of these factors, particularly parental attachment style and family dynamics, have the potential to affect a person's performance and daily activities in addition to their physical health [4-6].
According to reports, learning environments in dental schools are very rigorous and stressful [7]. Since the curriculum for the dental profession, in contrast to that of the medical profession, requires students to master multiple domains of theory as well as psychomotor and clinical proficiencies as well as patient communication and management protocols, this results in a demanding lifestyle that negatively affects dental students' physical and mental health [8]. Additionally, it decreases learning effectiveness. According to recent studies, dental students who must manage all the pressures may find studying to be quite difficult. In dentistry, stressors include things like one's home environment, character traits, academic environment, and clinical considerations [7, 8]. It has been observed that dental students who are in training experience severe stress-related symptoms. In comparison to the general population, dental students also exhibit higher levels of stress, sadness, OCD, and interpersonal sensitivity [9]. According to a prior study, students in the clinical years (fourth, fifth, and sixth) experienced more stress than those in the preclinical years. Furthermore, female students were more stressed than male students [10].
Ineffective stress management can result in physical and psychological symptoms that put people's health at risk. The effects of ongoing stress on students' health can include decreased performance at the job or in class, incapacity to continue working, trouble interacting with patients, and ultimately depersonalization [11]. The issues brought on by high levels of stress may eventually affect students' academic performance and limit their professional prospects. In order to manage stress and its negative effects, it can be good to evaluate the stress levels and stressors among dentistry students [12].
One of the crucial glucocorticoid hormones that the adrenal cortex releases to control physiological processes in the body is cortisol, which is also regarded as a key biological stress signal in response to emotional or psychological stimuli [13]. Plasma, urine, saliva, and hair samples can all be used to test cortisol hormone levels. Additionally, different levels of salivary cortisol can be measured in relation to external stress stimuli [14].
There has been contention that among young adult university students, there appears to be a connection between stress and salivary cortisol levels. These young people's salivary cortisol levels have been utilized as a gauge for stress and depression [5-7]. It is also unclear if salivary cortisol levels vary among young adult university students studying at various academic levels, despite some prior research demonstrating a positive correlation between stress and these levels [9-11]. In this perspective, the current study aimed to explore the relationship between self-perceived stress and salivary cortisol expression in relation to gender and academic levels, in a subpopulation of dental students, at King Saud University's Dental College in Riyadh, Saudi Arabia. The findings of this study may inspire new approaches for parents, teachers, counselors, and even the students themselves to influence dental students' behavior for improved health.
2. MATERIALS AND METHODS
2.1. Design of the Study and IRB Approval
This prospective cohort's study was conducted between September 2021 and January 2022. First through fifth-year undergraduate dentistry students from King Saud University participated in this study. King Saud University Medical City's institutional review board (IRB) granted its ethical approval (IRB permission # E-20-4834).
2.2. Sample Size Calculation
The G-Power software indicated that the required sample size was at least 140, with 70 in each group, at alpha=0.05, effect size=0.5, and power=0.9.
2.3. Data Collection Procedure
After receiving IRB approval, the principal investigator (PI) requested authorization from the university administration to set up a classroom for the purpose of recruiting study participants. Before completing the questionnaire and delivering the salivary samples, the qualifying individuals gave their written consent. Before beginning to answer the questionnaire's items, participants were given full explanations of the study, the questionnaire, and its purpose while sitting comfortably in a classroom.
2.4. Exclusion Criteria
The study did not include any students who had a history of hormone abnormalities, chronic systemic illnesses, or who were taking hormonal or chronic stress medications.
2.5. Inclusion Criteria
All the students who consented to participate in the study were included in the study except for those under the exclusion criteria.
2.6. Dental Environmental Stress (DES) Questionnaire
The goal of the study tool, the dental environmental stress (DES) questionnaire (Table 1), was to assess the stressors in the dental environment and students' coping mechanisms. The questionnaire had to be succinct and persuasive in order to increase positive feedback while providing the participants with the least amount of fatigue (stress). It was made sure that the study instrument included all relevant areas of interest in relation to the study's goals. There were 31 items relating to stress in the DES questionnaire. 25 items were taken directly from the original DES questionnaire (Garbee et al., 1980) [15], and the final six were added after reviewing modified DES questionnaires that had been published in the literature [16-20]. Self-efficacy beliefs (items 1–8), faculty and administration (items 9–17), workload (items 18–23), patient treatment (items 24-27), and clinical training (items 28–31) were the five areas of potential stressors that the 31 items were grouped into. On a four-point Likert scale with the options “not stressful at all,” “somewhat stressful,” “quite stressful,” and “very stressful,” respondents to the DES questionnaire assessed the items based on their perceptions of the questions posed.
2.7. Stress Classification
Participants in the study were divided into three groups based on their replies to the DES questionnaire: Mild, Moderate, and High Stress. Each of the four answers to each question was scored as “not at all stressful=0,” “somewhat stressful=1,” “quite stressful=2,” and “very stressful=3.” Each participant's total responses were added together to determine their level of stress, which was then categorized as follows: Low Stress = 0–31; Moderate Stress = 32–62; and High Stress = 63–93.
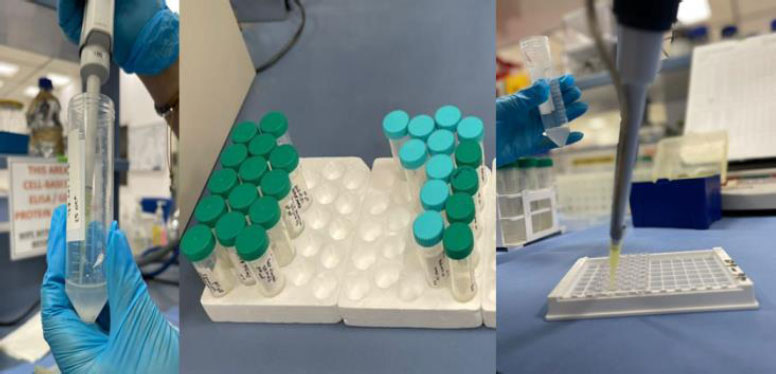
2.8. Salivary Samples’ Collection
Saliva was collected twice from each subject without any stimulation. Participants were told to abstain from food, liquids, and tobacco for at least three hours before saliva was collected. In order to lessen changes in salivary output brought on by the circadian rhythm, each collection was carried out at a specific time of day. Participants were instructed to relax for five minutes while swallowing all of the saliva in their mouths before the saliva was collected. They were told to sit with their heads leaned forward and spit into a graded test tube using a glass funnel. The total volume of the unstimulated saliva was measured five minutes after it was collected. A minimum of 5ml of saliva was collected from each participant (Fig. 1).
| Survey part 1 |
1. | Fear of being unable to catch up if behind |
| 2. | Fear of not being able to join a post graduate dental education program | |
| 3. | Language barrier | |
| 4. | Insecurity concerning lack of employment positions | |
| 5. | Fear of failing a course or the year | |
| 6. | Lack of confidence to be a successful dental student | |
| 7. | Lack of confidence to be a successful dentist | |
| 8. | Lack of confidence in own decision making | |
| Survey part 2 |
9. | Amount of cheating in dental school |
| 10. | Inadequate number of instructors in relation to student | |
| 11. | Getting study material | |
| 12. | Availability of qualified laboratory technicians | |
| 13. | Receiving criticism about work | |
| 14. | Inconsistency of feedback on work between different instructors | |
| 15. | Shortage of allocated clinical/laboratory time | |
| 16. | Lack of input into the decision-making process of school | |
| 17. | Being treated as immature & irresponsible by faculty | |
| Survey part 3 |
18. | Amount of assigned class work |
| 19. | Lack of time to do assigned school work | |
| 20. | Overloaded feeling due to huge syllabus | |
| 21. | Lack of time for relaxation | |
| 22. | Late ending day | |
| 23. | Difficulty of class work | |
| Survey part 4 |
24. | Patients being late or not showing for their appointments |
| 25. | Working on patients with dirty mouths | |
| 26. | Fear of dealing with patients who do not disclose the existence of a contagious disease | |
| 27. | Lack of cooperation by patients in their home care | |
| Survey part 5 |
28. | Responsibility of getting suitable patients |
| 29. | Difficulty in learning clinical procedures | |
| 30. | Transition from pre-clinic to clinic work | |
| 31. | Difficulty in learning precision manual skills required in preclinical work | |
| *The questionnaire items (on a four point Likert scale) divided to 5 parts based on domains. | ||
2.9. Specimen Processing and Testing
Saliva samples were provided to the lab for examination after being kept at 4–8°C in the individual's personal refrigerator for up to 7 days due to cortisol's stability. Materials are either frozen at -20 °C or centrifuged in the lab to obtain a clear supernatant (the analytical sample component), after which they are either immediately examined or kept frozen until analysis. To ensure the cleanest analytical sample was used, the samples were frozen and centrifuged once more before analysis. Following the addition of the commercial immunoassay, the Stratech High Sensitivity Salivary Cortisol EIA kit, and the salivary cortisol buffer with a pH of 8 (200 L), the samples were vortexed in vials. Next, cortisol was found.
2.10. ELISA Tests
An enzyme-linked immunosorbent test, or ELISA, was used to quantify the quantity of cortisol present in saliva samples. Using microplate readers set at 450 nm (Bio-Rad Laboratories International, Hercules, California, USA), the results of the ELISA test were analyzed. The ELISAs were carried out in accordance with the manufacturer's instructions (The Salimetrics® Cortisol Enzyme Immunoassay Kit, Salimetrics, LLC 101 Innovation Boulevard, Suite 302, State College, PA 16803, USA).
2.11. Statistical Evaluation
Excel sheets were used to record and tabulate each participant's questionnaire replies. Using Chi-square testing, gender comparisons for the questions asked were made. The mean of the cortisol levels from the two salivary collections for each participant was taken as the final reading for that participant. Salivary cortisol levels and participant demographics, such as age and gender, were noted and entered into an Excel spreadsheet. The collected data was entered into software for statistical analysis (SPSS; IBM Corporation) for statistical analysis. We utilized two-tailed Student's t-tests to look at the gender and academic levels wise group comparisons. For all statistical studies, α<0.05 level of significance was chosen.
3. RESULTS
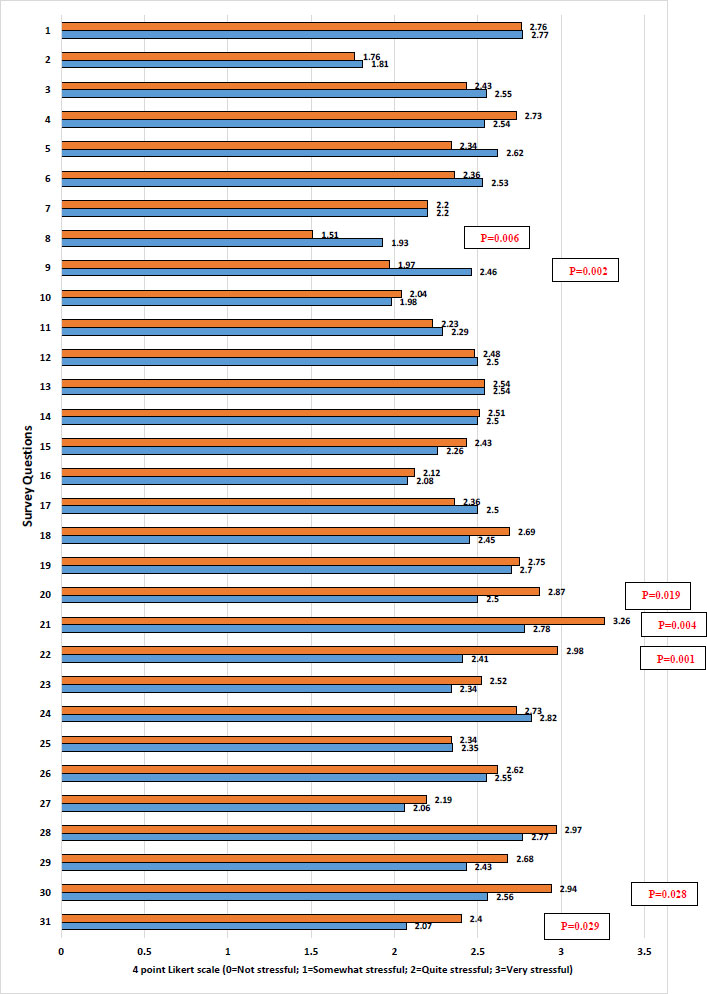
151 students (79 men and 72 women) participated and provided written consent to participate in the study. Fig. (2) displays the replies from the students by gender to the four-point Likert scale questions. For the bulk of the items posed in relation to the stress questionnaire, comparisons of the responses from male and female students revealed a similar tendency. Male and female students’ responses varied, however, for seven items (P<0.05). Question 8 was for the participants to rate their level of confidence in their own judgment. The responses were significantly different (P=0.006), with female respondents evaluating their level of confidence as lower than male respondents.
The replies from the female respondents were significantly different (P=0.002) from those of the male respondents to question 9, “How much cheating occurs in dental school,” with the female respondents expressing more concern. For question number 20, “Overloaded feeling due to huge syllabus,” the responses were significantly different (P=0.019), with the male students reporting a greater impact from the overloaded syllabus in the dental school than the female students. The replies to question number 21 (Lack of time for relaxation) differed significantly from those of the other questions (P=0.004), with the male students suffering more negatively than the female students from the lack of downtime in the dental school.
The replies to question number 22 (Late completing day) demonstrated a notable difference (P=0.001) between the sexes, with the male students suffering more consequences as a result of the dentistry school's late concluding day. For question 30 (Transition from pre-clinic to clinic work; P=0.028), the responses were significantly different, with the male students reporting greater effects on the transition from pre-clinic to clinic work in the dentistry school than the female students. The responses to question number 31 “Difficulty in learning precision manual skills required in preclinical work”; P=0.029) showed a significant difference, with male students responding significantly more negatively than female students to the challenge of learning precision manual skills needed for preclinical work in the dental school.
The mean values of salivary cortisol levels for the involved students are compared by gender and academic level in Table 2. The male subjects' cortisol levels' mean and standard deviation were 1.54 + 0.41 and the female subjects' mean and standard deviation were 1.28 + 0.45. The comparisons showed that there were statistically significant differences between the cortisol levels of the male and female subjects (p=0.000). The mean cortisol levels of the participating students at the two different academic levels did not differ statistically significantly (P=0.150). 62 and 89 preclinical and clinical students, respectively, were included in the study (Table 2). The cortisol levels' mean and standard deviation were 1.48 + 0.44 and 1.37 + 0.45, respectively, at the preclinical and clinical levels.
According to the participants' rating of stress as Mild, Moderate, or High, Table 3 shows the descriptive statistics and comparison of cortisol levels for male and female students. In comparison to female students (13.88%), more male students (30.37%) fell into the category of mild stress. The percentage of male and female pupils falling under the category of moderate stress was the same (54%). However, compared to their male counterparts (15.18%), female students (31.94%) predominated in the high stress environment. Although the proportion of male and female students experiencing moderate stress was comparable, their salivary cortisol levels were significantly different (P=0.004), while those experienced by male and female students experiencing mild and high stress were not (P>0.05) (Table 3).
According to the classification of stress as being mild, moderate, or high, Table 4 shows the descriptive statistics and comparison of cortisol levels at the two academic levels of the participating students. Compared to clinic students (13.88%), a higher proportion of preclinical students (30.37%) fell into the mild stress category. When compared to students in the preclinical stage (36.70%), the percentage of students in the moderate stress classification was very high (73.61%). Similar to this, a higher percentage of students (36.11%) fell into the high-stress category than did students in the preclinical stage (11.39%). For the participating students at the preclinical and clinical levels of the study, the results showed comparable non-significant (P>0.05) levels of salivary cortisol (Table 4).
| Comparison | Gender | N | Mean | Sth. Deviation | Sth. Error Mean | *P-value |
|---|---|---|---|---|---|---|
| Gender | Male | 79 | 1.54 | .41 | .04 | 0.000 |
| Female | 72 | 1.28 | .45 | .05 | ||
| Academic Level | Preclinical | 62 | 1.48 | .44 | .05 | 0.150 |
| Clinical | 89 | 1.37 | .45 | .04 |
Table 3.
| Stress Classification | Gender | N | % | Mean Cortisol | Sth. Deviation Cortisol | Sth. Error Mean | *P-value |
|---|---|---|---|---|---|---|---|
| Mild Stress |
Male | 24 | 30.37 | 1.50 | .40 | .08 | 0.226 |
| Female | 10 | 13.88 | 1.30 | .48 | .15 | ||
| Moderate Stress |
Male | 43 | 54.43 | 1.55 | .41 | .06 | 0.004 |
| Female | 39 | 54.16 | 1.28 | .41 | .06 | ||
| High Stress |
Male | 12 | 15.18 | 1.58 | .49 | .14 | 0.127 |
| Female | 23 | 31.94 | 1.29 | .51 | .10 |
| Stress Classification | Academic Level | N | % | Mean | Sth. Deviation | Sth. Error Mean | *P-value |
|---|---|---|---|---|---|---|---|
| Mild Stress |
Preclinical | 24 | 30.37 | 1.50 | .42 | .08 | 0.187 |
| Clinical | 10 | 13.88 | 1.29 | .43 | .13 | ||
| Moderate Stress |
Preclinical | 29 | 36.70 | 1.45 | .46 | .08 | 0.670 |
| Clinical | 53 | 73.61 | 1.41 | .42 | .05 | ||
| High Stress |
Preclinical | 9 | 11.39 | 1.53 | .45 | .15 | 0.355 |
| Clinical | 26 | 36.11 | 1.34 | .53 | .10 |
4. DISCUSSION
Cortisol is a hormone that affects nearly every organ system in the body, including the neurological, immunological, cardiovascular, respiratory, reproductive, musculoskeletal, and integumentary (hair, skin, and nails) [1, 2, 13]. Cortisol, on the other hand, is well known for its role in the neurological system as part of the stress response [21]. The idea that even tiny negative impacts can cause stress and increase cortisol levels, while positive effects have the opposite effect, has been supported by a number of studies employing instantaneous evaluations of stress and salivary cortisol. Stress causes an increase in cortisol levels, which compromises the normal functions of practically all human bodily systems [22]. The results of the present investigation revealed that female students self-assessed themselves as being more stressed, the salivary cortisol levels were considerably higher among male students and there were no discernible variations in salivary cortisol levels at different academic levels.
The link between self-perceived stress and salivary cortisol expression was studied in the current study among a group of dentistry students using a self-administered stress questionnaire and by monitoring the participants' salivary cortisol levels. The study's methodology is unique in that participants was classified as having mild, moderate, or high stress levels based on their responses to the stress questionnaire, and then their salivary cortisol levels were measured and compared based on gender and clinical and non-clinical academic levels.
Salivary cortisol testing has the major benefit of allowing samples to be taken both in the research participant's natural surroundings and particular locations away from the lab [23]. Furthermore, because saliva collection is a noninvasive sampling method, it does not cause additional stress in participants [14]. The research linking salivary cortisol levels to stress in young adults/college students has been inconsistent. According to some, the more the stress, the higher the cortisol levels [23]. Others have discovered that the lower the stress level, the lower the salivary cortisol levels [24]. Others do not see much of a connection [25]. The current study results demonstrated that male and female participants had distinct reactions to the questions, as well as disparities in cortisol levels under different classed stress scenarios.
The group of participants employed in these investigations, which can have an impact on the results of these studies, is a crucial aspect to note and stress here. Income level, parental education, nutrition intake, social lifestyle, physical condition, and academic workload are all factors that influence stress in adolescents [26]. Because the participants in this study were high-achieving students with a heavy academic workload, their stress levels and salivary cortisol levels were likely to be higher [27]. Because of the differences in their socioeconomic backgrounds, this somewhat diversified group of participants may have an effect on their stress levels and cortisol levels.
Male and female students' responses to their own perceived stress differed, as documented in earlier studies. Female students appear to have a higher level of self-assessed stress [28]. According to the literature, females are more depressed than males. As a result, they will perceive their stress levels to be higher than men [29]. The majority of the responses to the questions by the participating students of both genders in this current study were similar. However, when asked questions such as “Lack of trust in one's own decision-making” and “How much cheating occurred in dental school,” female respondents expressed greater concern, demonstrating their susceptibility to stress. According to the stress categorization employed in this study, the number of female student participants in the high stress group was double that of their male counterparts. Confirming the tendency of young females to experience self-perceived stress.
Despite the fact that female participants had a higher tendency to stress according to the current study's survey, their mean cortisol levels were significantly lower than male participants. Several studies reported that males had higher levels of cortisol than females, with cortisol concentrations remaining unchanged or decreasing in men [23, 30]. There could be several reasons for males having higher cortisol concentrations than females, ranging from simple day-to-day variations in cortisol levels to more complex physical variations and dietary and social lifestyle differences between the two genders [31]. Thus, the current findings are consistent with previous literature [23, 30, 31] and emphasize the importance of investigating potential gender differences throughout the research process, including design, analysis, and interpretation of results. We suggest more investigation into gender variations in cognitive and/or emotional reactions to upsetting psychosocial events, which may affect cortisol levels, even though the current findings are not conclusive.
The study's limitations should be acknowledged. Because the survey was a typical cross-sectional study conducted on a relatively small number of volunteers, it was not possible to provide “cause or effects analysis,” which helps you identify all of the likely causes of the stress that the participating students may be experiencing, as well as the complex relationships between the various variables investigated. The inclusion of volunteers in the study could only have resulted in a selection bias. Rather than comparing strain and other variables across educational groupings, the study was conducted with people with a specific educational background (Dentistry). Because different educational systems have different challenges/stress markers that may influence the neuro-endocrinal system, the findings cannot be generalized to other populations. These findings cannot be extrapolated to people from various socioeconomic and occupational backgrounds. Future research could look into the relationship between diverse educational backgrounds, stress, and variations in the levels of cortisol at different points of their studies. Nevertheless, the present study provided some very useful information related to the salivary cortisol levels among young university students. The study's sample size was well selected, and it only included healthy participants in a controlled environment, which is a big advantage. Unlike some other research, in which participants may have been influenced by taking different medications and/or suffering from different conditions. The information can be used and helpful in future research studies related to the topic.
CONCLUSION
Within the limitations of the study it can be concluded;
- The responses of the participants revealed that the female students appeared to have higher self-assessed stress levels than their male counterparts, indicating the trend of young female students towards stress was higher.
- Variations existed in the levels of salivary cortisol with male students exhibiting significantly higher amounts of cortisol levels than female students.
- There were no significant changes in the salivary levels of cortisol among the participating students' at the preclinical and clinical academic levels.
LIST OF ABBREVIATION
| PI | = Principal Investigator |
| DES | = Dental Environmental Stress |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
At the College of Dentistry Research Center, King Saud University, Riyadh, Saudi Arabia, the project received approval from the institutional review board (IRB), and its project activities were approved by the institutional committee of research ethics (IRB permission # E-20-4834).
HUMAN AND ANIMAL RIGHTS
No animals were used that are the basis of this study. The 2013 revision of the 1975 Helsinki Declaration was followed when conducting the study.
AVAILABILITY OF DATA AND MATERIALS
Data is available on request from the corresponding author [S.H].
FUNDING
This study was funded by College of Dentistry Research Center (CDRC), College of Dentistry, King Saud University, Riyadh, Saudi Arabia.
ACKNOWLEDGEMENTS
Declared none.

