All published articles of this journal are available on ScienceDirect.

Degree of Concordance Between Cone Beam Computerized Tomography (Cbct) And 2d Digital Radiography System Used for Caries Diagnosis: An Observational Study
Authors Info & Affiliations
Abstract
Background:
Caries is a disease with a high prevalence, which may be due to the lack of adequate methods for its early diagnosis, becomes difficult to detect initial caries lesions in posterior teeth due to the occlusal anatomy of these and because on many occasions they start in the interproximal zone below the contact areas.
Different techniques have been used for the diagnosis of caries, such as visual-tactile inspection, radiography, tomography, and transillumination, but none of them seems to have complete sensitivity or specificity.
Aim:
This study aims to establish the degree of agreement between radiographic diagnosis with 2D intraoral digital radiography in relation to cone beam computed tomography in extracted carious and healthy posterior teeth, practicing the CariesCare International ™ practical guide as a reference.
Materials and Methods:
A total number of 117 teeth with or without carious lesions were selected. Digital images of all teeth were obtained from 2D digital radiographs (instrumentarium ™ films) obtained with Kavo focus equipment and CBCT scanner I-CAT ™ model 1719, ISI (imaging science international), Pennsylvania (blue sky plan 4 software).
Observers evaluated the images for the detection of carious lesions. The sensitivity and specificity ratio between the systems was determined using the area under the curve statistical tool ROC (Receiver Operating Characteristic).
For the statistical analysis, the statistical program STATA IC/16 was used, in which the calculation of absolute and relative frequencies for each category of CariesCare international in CBCT and radiography was performed, in addition to the Friedman and post-hoc Wilcoxon test by pairs; the distribution according to the classification of CariesCare international was contrasted between the CBCT slices. The calculation of weighted Kappa and dichotomous Kappa and the calculation of validity (sensitivity and specificity) and prediction (predictive values and predictive ratios) were performed.
The distribution according to CariesCare international classification was contrasted between the CBCT slices.
Results:
The results of the present study confirm that diagnosis of caries with the 2D digital radiographic method, initial caries lesions tend to go undetected relative to CBCT.
Conclusion:
2D digital radiographs showed low sensitivity for caries detection and high specificity relative to CBCT for caries lesions in vitro. Diagnosis with 2D digital Rx is considered non-discriminative in identifying initial caries lesions.
1. INTRODUCTION
Dental caries is one of the most prevalent chronic diseases among children, affecting approximately 621 million children worldwide [1], and one of the reasons for the high prevalence is the difficulty in early diagnosis, which allows caries to develop [2].
Early diagnosis of dental caries has always been one of the essential objectives of dentistry, although caries is a multi-causal disease, lesions develop where biofilms are allowed to mature and remain for a prolonged time. Carious lesions in posterior teeth initially develop in the occlusal areas, especially during the eruption period, and on the interproximal surfaces below the contact areas [3].
Early diagnosis of caries is a challenge for clinical dentists; although different diagnostic methods exist, none have been found to have the highest sensitivity or specificity [4], a widely accepted method is the visual-tactile inspection proposed by the International Caries Detection and Assessment System (ICDAS) [4]. However, this method alone has proven to be insufficient to detect the extent of caries or lesions in the interproximal area [5], so it must be accompanied by other methods such as periapical radiography, transillumination, and fluorescence [4].
Occlusal caries is the most common form of caries in primary and permanent teeth since the complex occlusal anatomy favors plaque accumulation, which makes a diagnosis based solely on visualization difficult; moreover, radiographic diagnosis is effective, especially in advanced stages of caries [6].
Interproximal caries is difficult to diagnose due to its location below the contact zone which prevents visualization. The indicated method for this is bitewing radiography, which is more sensitive than visual inspection [7], however, for occlusal caries to be detected with a bitewing radiograph, the lesion must have affected the middle third of the dentin [8].
Clinical diagnostic methods usually rely on radiographic methods, especially when interproximal lesions are suspected; despite this, radiographic imaging also has limitations related to the difficulty of identifying early lesions, as it is reported that 30-40% loss of enamel mineral is necessary for radiographic detection to be possible [6].
Despite major advances in the field of digital radiology, these images are still two-dimensional representations of a three-dimensional structure, and no significant differences have been found when comparing conventional methods with digital radiography for the detection of interproximal caries [9].
Low to moderate sensitivity, slightly better specificity, and high observer variability have been reported for the detection of occlusal and interproximal surface lesions [10]. On the other hand, it has been shown that radiography could result in false positive diagnoses, leading to unnecessary intervention [11]. With the introduction of cone beam computed tomography (CBCT), interest in this field has increased due to its advantages, such as improved image quality, three-dimensional reconstruction, a 1:1 ratio allowing reliable measurements, the possibility of craniofacial visualization and lower radiation doses compared to traditional CT [12]; although few studies report the accuracy of caries detection with this technique, it is considered a promising tool for the early diagnosis of dental caries [13].
Qasem D. et al., 2015 compared images corresponding to conventional, digital, and tomographic radiographs of occlusal caries of 160 posterior teeth, and reported that CBCT images had better sensitivity and digital radiographs had better specificity; however, there were no significant differences between the diagnostic modalities studied [14].
Krzyżostaniak et al, 2014 evaluated the accuracy of cone beam computed tomography (CBCT) in detecting non-cavitated occlusal caries lesions and compared this accuracy with that observed with conventional radiographs; they reported slightly better performance of the CBCT unit in terms of sensitivity; however, the values reported for both methods were low [15].
Beltran et al., 2020 compared the diagnostic accuracy of cone beam computed tomography and three intraoral radiographic systems for the detection of caries lesions in vitro and reported that CBCT I-CAT was a valid technique for lesion diagnosis compared with conventional and digital radiography methods [16].
The aim of this study is to determine the degree of agreement in caries diagnosis between cone beam computed tomography (CBCT) and digital radiography system.
2. METHODOLOGY
In this observational, cross-sectional, descriptive study, 117 permanent molars and premolars with an indication for extraction and without any dental intervention were used; the teeth belonged to the study “Histomorphometric characterization of caries in pits and fissures in permanent teeth” and were taken from different hospitals and dental offices in Cali, Colombia after informed consent during the year 2021. The Kappa index (k) was used to calculate the sample size.
Inclusion criteria: Permanent posterior teeth (molars and premolars) extracted from the study “Histomorphometric characterization of caries in pits and fissures in permanent teeth”; Exclusion criteria: Premolars and molars with some type of restorative or rehabilitative treatment, or endodontic treatment.
Taking into account that the aim is to evaluate the concordance between two diagnostic methods (2D digital radiography and CBCT tomography) and that in the 2D digital radiographic method, a mineral loss of 30-40% must occur for the radiographic detection of enamel caries, the following hypotheses were put forward:
2.1. Alternative Hypothesis (H1)
It is likely that when diagnosing, the initial caries lesions will be detected by CBCT tomography and will not be detected by the 2d digital radiographic method.
2.2. Null Hypothesis (H0)
Detection of initial caries lesions was the same for both methods.
The minimum sample to fulfill the hypotheses was 97 teeth, and 95% standard confidence intervals were obtained [17, 18].
2.3. Tooth Preparation
Once the extractions were performed, the teeth were deposited in containers with buffered formalin for 30 minutes. Subsequently, they were disinfected for 5 minutes by immersion in a solution of povidone-iodine (Povidone iodine solution. Isodine MK- Tecnoquímicos Laboratory. Cali. Colombia). Then, they were washed with running water and a toothbrush and stored in jars with sterile distilled water.
At the time of the clinical examination, the teeth were removed and left to dry in the environment for 36 hours, the diagnosis was recorded according to CariesCare InternationalTM and they were stored in labeled containers for the subsequent taking of radiographic and tomographic images.
Teeth extracted during different treatments and not for the sole purpose of this study were collected with the consent of the patients, following the clinic's ethical protocol. The research was approved by the human ethics committee, IRB approval No. 018-2019.
3. OBTAINING THE IMAGES
The radiographic images were taken with Kavo focusing equipment (Palo DEx Group Oy. Tuusula. Finland) with a power of 70 KV, a current intensity of 7 mA, a total filtration of 2.0 Aluminum and a focal point of 0. 7 mm, photostimulable phosphor plates were used (Dental Instrumentation. Palo DEx Group Oy. Tuusula. Finland), with an exposure time of 0.2 seconds and a distance of 8.5 cm.
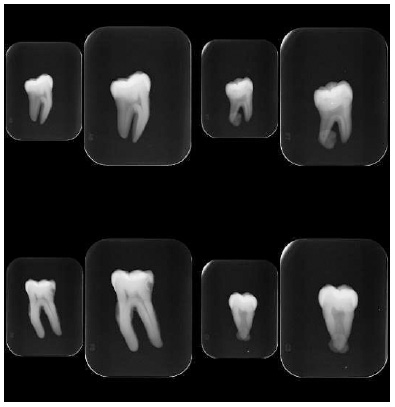
Simultaneous images were taken using a radiographic template, in each template (one series) the radiographic images of four teeth were saved, so a total of 25 templates were made (Fig. 1).
To facilitate the positioning of the teeth for the digital radiographic acquisition, a 5 mm diameter sphere made of pink wax was made to give stability to the teeth and standardize image acquisition to give stability to the teeth and standardize acquisition of the images, which were taken with the parallel technique.
All the images were taken under the supervision of a specialist in oral and maxillofacial radiology.
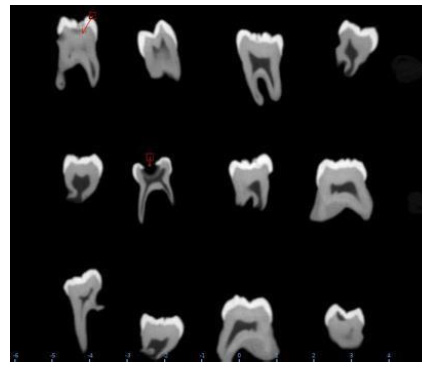
An Imaging Sciences International model 1779 tomograph (Imaging Sciences International, Hatfield, PA. USA), with a voxel size of 0.25mm, power of 120 Kv, current intensity: 5 mA, and exposure: 7 seconds, was used for tomographic examinations.
The tomographic images were captured and transferred to Blue Sky Plan 4 software for analysis (Libertyville, IL USA; Fig. (2) shows an example of the images taken).
The visual inspection of the radiographs and digital tomographies was performed under ideal conditions for the interpretation of the images. The visualization sessions of radiographs and tomographies were carried out considering a visual break of 15 minutes for every 2 hours of work on the computer and, every 20 minutes, there was a break.
3.1. Observer Calibration
Once intraexaminer and interexaminer calibration were obtained, the evaluation of the radiographic and tomographic images was performed by two examiners with experience in caries image evaluation.
The calibration of the observer for the evaluation of the radiographic images was performed by a specialist in cariology and the classification of the tomographic images was performed with the previous calibration of a specialist in oral and maxillofacial radiology. Calibration had the possibility of removing possible differential diagnoses from the diagnostic process that could act as confounders or invalid results. In addition to controlling diagnostic misclassification processes, also removes biases from the diagnostic process.
The classification was based on the CariesCare International radiographic caries categories as follows
3.2. Statistical Analysis Plan
The database was constructed as a spreadsheet in Microsoft Excel and imported into MedCalc 15. The analysis consisted of calculating the absolute and relative frequencies of each CariesCare International (CCI™) category in both CBCT and RX observations. A Spearman correlation test was used to determine the correlation between the two caries assessment systems; The weighted Kappa index was calculated to determine the agreement between the two systems.
The distribution of CariesCare levels between CBCT visualization slices was contrasted with Friedman's and Wilcoxon's pairwise post-hoc tests. Linearly weighted Kappa index (Kappa) was calculated to contrast the CariesCare diagnosis between the different sections and evaluation methods. A Kappa index was also calculated for variables dichotomized according to caries identification or not. Concordance was classified according to Altman (1991) [19, 20].
In addition, the validity parameters (sensitivity and specificity) and predictive (predictive values and likelihood ratios) of the X-ray evaluation were calculated, using the diagnosis obtained by CBCT as a reference value, for initial lesions and possible carious lesions on the coronal and proximal surfaces. The confidence level was set at 95% and the significance level at 5%.
4. RESULTS
Out of one hundred seventeen teeth that were evaluated, most of the teeth evaluated were free of dental caries. The presence of caries was evaluated according to the CariesCare International (CCI™) classification and contrasted with the three visualization slice planes.
When comparing the three visualization slices, it can be seen that the axial slice reports the lowest percentages of detection of caries lesions (initial 12%), (moderate 8%), and (extensive 1%). In contrast, in the sagittal and coronal cuts, higher percentages of detection of caries lesions were reported (Table 1).
In the coronal slice 34% of initial lesions, 8% of moderate lesions, and 1% of extensive carious lesions were detected, while in the sagittal slice 34% of initial lesions, 7% of moderate lesions, and 1% of extensive lesions were reported. Therefore, caries identification was higher in the visualization from sagittal and coronal slices.
The differences in the CariesCare classification levels were statistically significant between the axial slice and the sagittal and coronal slices, while this was not the case when comparing the latter two slices.
| - | Axial | Sagittal* | Coronal* | - |
|---|---|---|---|---|
| - | n (%) | n (%) | n (%) | P |
| Healthy | 95 (81.90) | 74 (63.25) | 74 (63.25) | <0.000 |
| Initial | 12 (10.34) | 34 (29.06) | 34 (29.06) | - |
| Moderate | 8 (6.90) | 7 (5.98) | 8 (6.84) | - |
| Extensive | 1 (0.86) | 2 (1.7) | 1(0.859) | - |
To evaluate the diagnostic agreement according to the level of involvement (mild-moderate and severe), the weighted Kappa was taken into account, and the dichotomous Kappa was used to evaluate the presence or absence of caries.
Dichotomous diagnostic agreement between axial vs. sagittal and/or coronal showed moderate agreement (Kappa 0.41 - 0.60), while this agreement was good (Kappa 0.61 - 0.80) when calculated according to the CariesCare International (CCI™) radiographic classification (which classified as mild, moderate, and severe). The agreement was perfect between dichotomized variables and the CariesCare classification between sagittal and coronal views (0.81 - 1.00) (Table 2).
| Slice | Axial | Saggital | Coronal |
|---|---|---|---|
| Axial | - | 0.547* | 0.547* |
| Saggital | 0.673 1 | - | 1* |
| Coronal | 0.673 1 | 0.986 1 | - |
1 Linear Weighted Kappa (CCI TM Classification)
Regarding the location of the carious lesions, the following was found: Adding all the percentages of the lesions in the three stages (initial, moderate, and extensive), the frequency of caries on the occlusal surface was 30.77%, with 88.89% in the initial stage; in proximal, the presence of caries was 2.56% when adding the three stages, with 66.67% in the initial stage (Table 3).
| - | Occlusal | Proximal |
|---|---|---|
| CCITM | n (%) | n (%) |
| Healthy | 81 (69.23) | 114 (97.44) |
| Initial | 32 (27.35) | 2 (1.71) |
| Moderate | 3 (2.56) | 0 (0.0) |
| Extensive | 1 (0.8) | 1 (0.8) |
The concordance between the two methods of proximal caries evaluation showed poor values (Kappa>0.20) in the dichotomous identification and by categories, as well as for the dichotomous evaluation on the coronal surface; for the CariesCare International (CCI™) classification on the coronal surface, the concordance was weak (0.21 - 0.40).
On the other hand, in the radiographic evaluation, occlusal caries was identified in 20.51% of the images when added the initial and extensive lesions since, in this case, no moderate lesions were detected; of all these occlusal lesions, 91.67% corresponded to the initial level; on the other hand, in the proximal surfaces, 6.84% of the teeth presented caries when added the three stages, after being evaluated, 62.50% were in the initial level and 25% in the moderate level (Table 4).
| - | Occlusal | Proximal |
|---|---|---|
| CCITM | n (%) | n (%) |
| Healthy | 93 (79.49 | 109 (93.16) |
| Initial | 22 (18.80) | 5 (4.27) |
| Moderate | 0 (0.0) | 2 (1.71) |
| Extensa | 2 (1.71) | 1 (0.85) |
Caries injuries were mostly located on the occlusal surface, and most were in the initial stage.
Dichotomous Kappa was used to evaluate the presence or absence of dental caries and weighted Kappa was used to evaluate the severity according to the Caries Care International radiographic classification (mild, moderate, and extensive).
When evaluating the concordance between the diagnostic methods CBCT and 2D digital radiography according to the location of dental caries (coronal and proximal), a poor concordance was obtained when evaluating dichotomous Kappa in proximal and a slight concordance in coronal. On the other hand, a slight concordance was obtained for weighted Kappa in coronal (Table 5).
| - | CBCT |Rx | |
|---|---|---|
| Slice | Coronal | Proximal |
| Dichotomized (Presence of caries) | 0.115* | 0.0387* |
| weighted Kappa (CariesCare International) | 0.2041 | 0.02901 |
1Linear Weighted Kappa (RX Classification CariesCare International)
Tomography was considered the gold standard for comparison. Taking this into account, out of a total population of 113 mild caries lesions, when making the diagnosis with 2D digital radiography, 32 were reported with caries and 81 without caries or healthy. Of the 32 diseased teeth with caries, 6 were true positives.
Of the 32 teeth with caries, 26 were false negatives, that is, they had caries and were negative for caries in the diagnostic tests; On the other hand, of the 81 healthy teeth, 14 were reported as positive for caries when in fact they were healthy, and 67 were indeed healthy and were reported as such. Therefore, it is corroborated that the 2D digital radiographic test allows better diagnosis of healthy teeth and not diseased teeth when the lesions are in the initial stage on the coronal surface. We did not have any missing data.
When comparing the validity and degree of prediction of 2D digital radiography versus CBCT for minor lesions on the coronal surface, 2D digital radiography shows poor sensitivity (18.75%) and high specificity (82.72%), the area under the curve confirms that this test is non-discriminative.
About the validity and prediction of 2D digital radiography versus CBCT for any lesion on the coronal surface, 2D digital radiography shows poor sensitivity (Sn) (27.78%) and high specificity (Sp) (82.72%) shows poor sensitivity (27.78%) and high specificity (82.72%) the area under the curve (AUC) confirms that this test is the non-area under the curve confirms that this test is non-discriminative.
Due to the absence of proximal caries in the teeth evaluated, the sensitivity was 0%, indicating 100% false positives, while the specificity was 93.64% when limited to mild lesions and 92.98% when evaluating the entire group with any lesion. Therefore, the identification of mild proximal caries or any lesion by radiography is not discriminatory with respect to CBCT.
When evaluating minor lesions on the proximal surface, 2D digital radiography shows poor sensitivity (0%) and high specificity (93.64%), the area under the curve confirms that this test is non-discriminative. 2D digital radiography has poor sensitivity (0%) and high specificity (92.98%), the area under the curve confirms that this test is non-discriminative (Table 6).
| - | Oclusal (minor) | Oclusal (all) | Proximal (mild) | Proximal (all) |
|---|---|---|---|---|
| - | Value (IC 95) | Value (IC 95) | Value (IC 95) | Value (IC 95) |
| Sn (%) | 18.75 (7.21 - 36.44) | 27.78 (14.20 - 43.19) | 0.00 (0.00 - 70.76) | 0.00 (0.00 - 70.769 |
| Sp (%) | 82.72 (72.70 - 90.22) | 82.72 (72.70 - 90.22) | 93.64 (87.33 - 97.40) | 92.98 (86.64 - 96-92) |
| AUC | 0.51 (0.41 - 0.60) | 0.55 (0.46 - 0.64) | 0.47 (0.37 - 0.56) | 0.46 (0.37 - 0.56) |
| LR+ | 1.08 (0.46 - 2-57) | 1.61 (0.79 - 3.27) | 0.00 | 0.00 |
| LR- | 0.90 (0.81 - 1.19) | 0.87 (0.70 - 1.09) | 1.07 (1.02 - 1.12) | 1.08 (1.02 - 1.13) |
| DP (%) | 28.32 (20.24 - 37.57) | 30.77 (22.57 - 39.97) | 2.65 (0.55 - 7.56) | 2.56 (0.53 - 7.31) |
| PPV (%) | 30.00 (11.89 - 54.28) | 41.67 (22.11 - 63-36) | 0.00 (0.00 - 40.969 | 0.00 (0.00 - 36-94) |
| NPV (%) | 72.04 (61.78 - 80.89) | 72.04 (61.78 - 80.86) | 97.17 (91.95 - 99.41) | 97.25 (92.17 - 99.43) |
LR-: Negative likelihood ratio; DP: Disease prevalence;
PPV: Positive predictive value;
NPV: Negative predictive value.
5. DISCUSSION
The null hypothesis of the present study was that the detection of initial caries lesions is the same in both methods. However, the results of the present study reject the null hypothesis and confirm that when diagnosing caries with the 2D digital radiographic method, initial caries lesions tend to go undetected relative to CBCT.
Regarding the in vitro caries lesion diagnostic ability of intraoral 2D digital radiographic systems, previous studies by Haiter-Neto F et al. in 2008 reported a sensitivity of 0.16 and a specificity of 0.92 in detecting dental caries lesions [21]. This coincides with the results obtained in this study, in which digital radiographs showed low sensitivity for caries detection and high specificity, as 82.72% of healthy surfaces were identified as such on radiographs.
The value of the area under the ROC curve (Az value) is directly related to the sensitivity and specificity of the tests. In the present study, the area under the curve of Rx versus CBCT coincided with the line of non-discrimination, being close to 0.50, so the 2D digital Rx diagnostic test is considered non-discriminatory in the identification of initial caries lesions, this is consistent when evaluating the presence of any caries lesion.
The above results demonstrate the poor ability of digital and conventional radiographic systems to detect early caries lesions. Carious lesions in their initial stages require a valid clinical diagnosis and the findings suggest a low discriminatory process for this incipient finding.
Beltran J et al., 2020 compared the diagnostic accuracy of cone beam computed tomography and three intraoral radiographic systems for the detection of carious lesions in vitro and reported that CBCT was a valid technique for the diagnosis of carious lesions in vitro compared to digital and conventional radiographic methods, reporting CBCT sensitivity and specificity values of 0.84 and 0.93, respectively, and statistically significant differences between the CBCT system and the intraoral radiographic systems [16].
With this study design, 2D digital radiography shows little likelihood of detecting caries lesions relative to the use of CBCT; considering that this study was conducted in vitro, the sensitivity of digital radiography is likely to be even lower clinically.
Walsh et al. 2021, conducted a systematic review of imaging modalities for the detection and early diagnosis of caries and reported that there is still low-quality evidence suggesting that imaging for early caries diagnosis may have poor sensitivity but acceptable specificity, resulting in a relatively high number of false-negative results with the possibility of progression of initial lesions [22].
This is in agreement with our results; likely, the sensitivity values reported in our study for 2D digital images were low because the vast majority of carious lesions in our sample were incipient.
Initially, we used weighted Kappa to assess diagnostic agreement, taking into account that the level of involvement could be Mild-Moderate and Severe; in addition, dichotomous Kappa was used to assess the presence or absence of caries.
The concordance between the two methods of proximal caries evaluation showed poor values (Kappa>0.20) in the dichotomous identification and by categories, as well as for the dichotomous evaluation on the coronal surface; while for the CARE classification on the coronal surface, the concordance was weak (0.21 - 0.40).
It is important to mention the concordance for dichotomous diagnosis and by category; taking into account that Kappa evaluates concordance beyond chance, and our results were poor and weak for the evaluation of proximal caries. One of the characteristics of our sample was that it was mainly composed of incipient caries lesions, which generated little variability in the data, an aspect that hindered a higher degree of concordance, although intra and interobserver.
This study was performed with images obtained from in vitro teeth, which may result in images of better quality than those obtained clinically; an opportunity for improvement would have been to place the teeth in an arch-like model to establish proximal contacts that could simulate the dental arch [16].
The sensitivity values reported in our study for 2D digital images were low due to the vast majority of incipient caries lesions, which generated little variability in the data.
One of the characteristics of our sample was that it was mostly composed of incipient caries lesions, which generated little variability in the data, an aspect that made it difficult to achieve a higher degree of agreement.
This study was performed with expert-calibrated observers under ideal viewing conditions. Consequently, the results may not apply to all clinical settings, environments, and modalities.
The actual condition of the surfaces tested by histologic examination was not performed as of yet
CONCLUSION
Diagnosis with 2D Digital Radiography is considered non-discriminatory in the identification of initial caries lesions; digital radiographs showed low sensitivity for caries detection and high specificity with respect to CBCT for in vitro caries lesions.
Digital radiography remains the diagnostic tool of first choice for the study of caries after the visual-tactile examination.
The use of digital radiography is ratified even in the absence of a clinical diagnosis of caries due to its high specificity. In healthy patients, it will perform well.
This study highlights the importance of knowing the advantages and limitations of digital imaging systems for caries diagnosis; also, it is the practitioner's responsibility to know in depth the applications and limitations of these tools.
Further research is needed to clarify caries detection with modern radiographic imaging systems.
LIST OF ABBREVIATIONS
| ROC | = Receiver Operating Characteristic |
| ICDAS | = International Caries Detection and Assessment System |
| CBCT | = Cone Beam Computed Tomography |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The research was approved by the human ethics committee, IRB approval No. 018-2019.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were according to the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from the patients.
AVAILABILITY OF DATA AND MATERIALS
All the data and supportive information is provided within the article.
STANDARDS OF REPORTING
STROBE guidelines were followed in this study.
FUNDING
The project carried out was financed as part of a call made by the Universidad del Valle, CI number 1866.
CONFLICT OF INTEREST
The authors declare no conflicts of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

