All published articles of this journal are available on ScienceDirect.

Accuracy in the Marginal Adaptation and/or Internal Adaptation of Full-coverage Fixed Prostheses Made with Digital Impressions and Conventional Impressions: A Systematic Review
Authors Info & Affiliations
Abstract
Aim:
The study aimed to verify compliance of the systematic reviews with the requirements established by the scientific community and demonstrate the validity and reliability of the systematic reviews conducted on the accuracy (marginal adaptation and/or internal adaptation) of the full-coverage fixed prostheses made with digital impressions versus conventional impressions.
Methods:
A search was performed for systematic reviews in three electronic databases, PubMed, Scopus, and Web of Science, as well as in the gray literature. In the search strategy, medical subject heading (MeSH) words were used in PubMed, and free terms were used for the titles and abstracts of each article. Each keyword was separated by the Boolean operator OR and later combined with the Boolean operator AND. Six systematic reviews were included for qualitative synthesis. To assess the methodological quality of the included systematic reviews, the AMSTAR 2 tool was used.
Results:
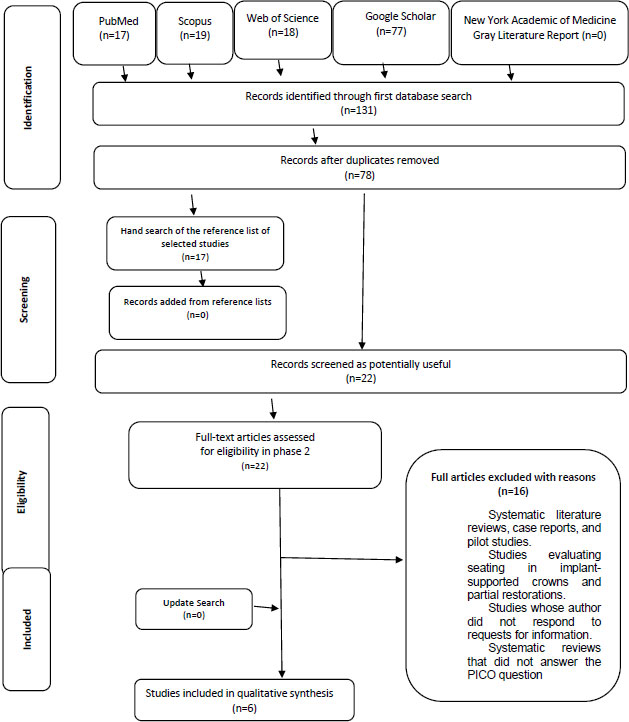
The search yielded 131 studies, of which 78 remained after removing duplicates. The title and abstract of each chosen study were assessed, and 22 articles were included for full-text reading. Finally, six studies were included, of which three studies were considered to have low confidence, while the other three were considered to have critically low confidence. In addition, the six SRs evaluated the adaptation or marginal fit, while only three studies measured internal adaptation.
Conclusion:
The use of digital impressions in single fixed prostheses maintains a marginal level within the limit of clinical acceptability; however, the methodological quality of systematic reviews is poor, according to the AMSTAR 2 tool.
1. INTRODUCTION
“Computer-aided design and manufacturing” (CAD/CAM) has been used in the preparation of dental restorations, especially crowns and ceramic fixed prostheses, since the 1980s [1-4]. It is believed that fixed dental prostheses, fabri-cated from intraoral digital impressions, have several notable advantages over those obtained through conventional impressions [5-9]. For instance, digital impressions better prevent errors of accuracy in the restoration margins than conventional impressions [10]. In addition, the general operating cost of the procedure and the clinical work time are reduced compared to conventional impressions [11-16].
A growing number of fixed prostheses are made using intraoral digital impressions, so this technique has become a fundamental part of digitalization in prosthodontics [17-21]. A good-quality fixed prosthesis that ensures treatment longevity depends on the marginal accuracy and internal fit between the abutment and the restoration [9, 22, 23]. The most common indicators of poorly adjusted restorative margins [24-31] are cement dissolution, plaque retention, periodontal problems, such as increased gingival inflammation and probing depth [32], dental hypersensitivity, and caries [33, 34]. The use of intraoral scanners has been introduced to minimize microadaptation errors and subsequent problems that conventional impression techniques can cause [35, 36].
Several studies have analyzed conventional and digital impression techniques, concluding that both procedures are clinically acceptable, and therefore, widely recommended. However, when studying the comparative accuracy of both techniques, results that can still be considered controversial begin to appear. Some authors suggest better results of the conventional technique over the digital technique, and others report better marginal adaptation of the digital technique than the conventional technique, thus confusing the professional who must make a scientifically supported clinical decision to provide high-quality prosthetic work with the greatest possible durability. A systematic review of the scientific literature could help evaluate the accuracy of these two techniques in a more comprehensive manner [37, 38].
For these reasons, this systematic review has been conducted to assess the compliance of the previous systematic reviews (SRs) on the accuracy (marginal adaptation and/or internal adaptation) of full-coverage fixed prostheses made with digital impressions versus conventional impressions with the requirements established by the scientific community in order to reveal the validity and reliability of each of these reviews and paint a clearer picture of clinical applicability when fabricating long-lasting fixed restorations.
2. MATERIALS AND METHODS
2.1. Protocol and Registration
A general protocol was developed based on the “preferred reporting items for systematic reviews and meta-analytical protocols (PRISMA-P) checklist” [39] and has been registered in the “International Platform of Registered Systematic Review and Meta-Analytical Protocols” (INPLASY). The registry is publicly available under the number INPLASY2021100024.
2.2. Eligibility Criteria
To be considered eligible, studies had to meet the following criteria:
- Systematic reviews with or without meta-analysis that have evaluated the accuracy (marginal adaptation and/or internal adaptation) of full-coverage fixed prostheses on natural teeth in clinical studies and on tooth replicas in in vitro studies.
- Systematic reviews with or without meta-analysis that have compared digital impressions made with an intraoral scanner versus conventional impressions taken with any type of impression material.
- Systematic reviews and/or meta-analyses of randomized clinical trials (RCTs) and comparative, prospective, nonrandomized, and in vitro clinical trials.
There were no time or language restrictions.
2.3. Exclusion Criteria
The studies excluded from this systematic review were the following:
- Literature reviews, case reports, and pilot studies
- Studies that have evaluated seating in crowns on implants and partial restorations.
- Studies whose authors did not respond to our requests for information.
- Systematic reviews that did not meet the patient/population, intervention, comparison, and outcomes (PICO) framework parameters.
2.4. Sources of Information and Search Strategy
On July 17, 2020, an electronic search was conducted in three databases (Scopus, PubMed, and Web of Science). The gray literature was also searched through Google Scholar and the New York Academy of Medicine Gray Literature Report. The bibliography of the included studies was manually examined. The studies obtained were exported to the Mendeley bibliographic reference manager (Mendeley Desktop v 1.19.4.0), and duplicate studies were eliminated. The search strategy can be found in Appendix A. A search update was performed on September 22, 2021.
2.5. Study Selection
The selected studies were entered into Microsoft Excel, a software program for data analysis. Initially, two reviewers (M.A.C. and M.C.) independently selected the studies and read all their titles and abstracts to estimate if each article met the inclusion criteria. These two reviewers then read the full text of each remaining article. A third and fourth reviewer (J.A. and Y.A.) were consulted in case of disagreement. Finally, any studies that did not meet the inclusion criteria were excluded.
2.6. Data Collection
The information on the articles was collected using a table previously prepared by two reviewers (M.A.C. and M.C.) independently and combined. The data were compared, and discrepancies between authors were decided by a third and fourth reviewer (J.A. and Y.A.). The information extracted from the selected articles is shown in Table 1.
2.7. Assessment of Methodological Quality
The AMSTAR 2 tool, a measurement tool to assess systematic reviews, was used by two reviewers (M.A.C. and M.C.) to assess the methodological quality of the SRs included, independently and combined. AMSTAR 2 has 16 domains that can be answered with three possible answers: “yes”, “no”, or “partially yes” [40]. Seven of its domains are considered critical, since they can substantially affect the validity of a review and its conclusions. The general confidence (high, moderate, low, and critically low) of the studies was evaluated according to Shea et al. [40] as high: no or non-critical weaknesses; moderate: more than one non-critical weakness; low: a critical defect with or without non-critical or critical weaknesses; and critically low: more than one critical defect with or without non-critical weaknesses. AMSTAR 2 does not generate an overall score, but the purpose of this tool is to identify high-quality systematic reviews.
2.8. Data Synthesis
The main results of each SR were categorized into the following topics: type of prosthetic restoration, marginal gap, internal gap, marginal discrepancy, marginal adaptation, and type of impression (Table 1). The data were visually presented as a traffic light plot where green represents the better marginal or internal adaptation, red represents poor marginal or internal adaptation, and yellow indicates no differences between the groups compared. The numerical data, the mean difference, and the relative risk can be found in Tables 2 and 3.
3. RESULTS
3.1. Review of Primary Study
From the search in the electronic databases and the gray literature, 131 references were obtained, of which 78 remained after eliminating duplicates. No articles from reference lists were added. Initially, the title and abstract of each chosen study were assessed, and 22 articles were included for reading the full text.
The search was refreshed, in order to obtain recent information that can be included in the study but no new articles were found. Finally, six SRs were included for qualitative synthesis. The reasons for excluding SRs can be found in Appendix B. The complete process of the identification and selection of studies is presented in Fig. (1).
3.2. Assessment of Methodological Quality
Three systematic reviews [41-43] were considered to have low confidence, while the other three [36, 44, 45] were considered to have critically low confidence. The explanation of the design selection of the included studies, an exhaustive literature search strategy, and the mention of the sources of funding of the studies included in the SRs, corresponding to domains 3, 4, 10, and 16, respectively, were considered critical. None of the SRs met these criteria. One SR partially complied with domain 9 regarding the assessment of the risk of bias in the included studies [43]. More information on the evaluation of the methodological quality is provided in Fig. (1) and in Appendix C.
| Author (Year)/Ref | Population | Interventions and Comparators | Primary Studies | Mention of the following items: 1. PRISMA 2. PROSPERO 3. GRADE 4. Meta-analysis |
Reported Review Limitations/Ref |
| Bandiaky et al. (2022) [41] | Fixed - supported prostheses | Intervention: digital scans Control: conventional impression techniques | Comparative studies, prospective: 2; randomized controlled clinical studies: 14 | 1. Yes 2. Yes 3. No 4. Yes |
Few studies per parameter and few participants included in each study. Evidence level was low for the studies that were otherwise heterogeneous.. [41] |
| Chochlidakis et al. (2016) [36] | Fit of fixed dental restorations | Intervention: digital impression techniques Control: conventional impression techniques |
Clinical studies: 2; in vitro studies: 9 | 1. Yes 2. No 3. No 4. Yes |
Additional cost of purchasing an intraoral scanner and the learning curve for adjusting to the new technology [36] |
| Hasanzade et al. (2021) [42] | Fixed prostheses | Intervention: digital scanning and conventional fabrication and digital scanning and fabrication. Control: conventional impression and fabrication and conventional impression and digital fabrication |
Clinical trials: 8; in vitro studies: 21 | 1. Yes 2. Yes 3. No 4. Yes |
No mention |
| Hasanzade et al. (2019) [43] | Full-coverage restorations | Intervention: digital impression Control: conventional impression | Prospective clinical trials: 8; in vitro studies: 26 | 1. Yes 2. Yes 3. Yes 4. Yes |
Uncontrolled factors may have had a direct influence on marginal and internal adaptation, including scanner type, finish line design, amount of spacer, fabrication technique, measurement of cemented or uncemented restorations, technical error during the laboratory stages, and adjustment of restorations. Subanalysis could not be performed due to the limited number of included studies. Only studies in English were included in the meta-analyses. [43] |
| Tabesh et al. (2021) [44] | Single-unit zirconia crowns | Intervention: digital scans Control: conventional impression |
Prospective clinical trials: 8; in vitro studies: 11 | 1. Yes 2. Yes 3. No 4. Yes |
Heterogeneity of the selected studies, including the different methods of tooth preparation, fabrication of restorations, and evaluation of marginal gaps. [44] |
| Tsirogiannis et al. (2016) [45] | Ceramic restorations | Intervention: digital impression Control: conventional impression | In vitro: 8; in vivo: 4 | 1. No 2. No 3. No 4. Yes |
No mention |
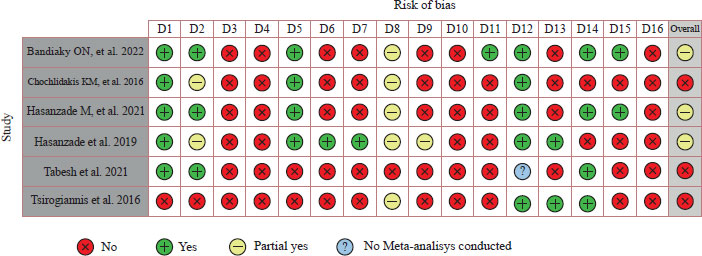
D1 Did the research questions and inclusion criteria for the review include the components of PICO?
D2 Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol?
D3 Did the review authors explain their selection of the study designs for inclusion in the review?
D4 Did the review authors use a comprehensive literature search strategy?
D5 Did the review authors perfom study selection in duplicate?
D6 Did the review authors perfom data extraction in duplicate?
D7 Did the review authors provide a list of excluded studies and justify the exclusions?
D8 Did the review authors describe the included studies in adequate detail?
D9 Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review?
D10 Did the review authors report on the sources of funding for the studies included in the review?
D11 If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results?
D12 If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis?
D13 Did the review authors account for RoB in individual studies when interpreting/ discussing the results of the review?
D14 Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review?
D15 If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review?
D16 Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review?
3.4. Marginal Fit/Marginal Gap/Marginal Adaptation/ Marginal Discrepancy
The marginal discrepancy was defined by Holmes et al. as the vertical marginal discrepancy measured between the crown and the margins of the preparation under a 3D optical microscope [46].
The six SRs evaluated the adaptation or marginal fit [36, 41-45], and three SRs [36, 41, 45] showed no significant difference in the marginal adaptation of single-unit fixed prostheses between digital and conventional impressions. Three SRs [42-44] showed a better marginal adaptation with digital impressions (Table 2). The mean difference in marginal adaptation between digital and conventional impressions ranged from -0.59 (CI -0.93, -0.24) to -4.2 (CI: -33.0, 24.5) micrometers. One SR [45] reported a mean marginal adaptation of 27.2 micrometers (with a range of -5.3 to 59.7 micrometers) in in vivo studies and -4.2 micrometers (with a range of -33.0 to 24.5 micrometers) in in vitro studies. Chochlidakis et al. [36] performed a quantitative and qualitative analysis of in vitro studies and reported a mean marginal discrepancy of 0.24 (-0.32, 0.79) micrometers, but they only performed a qualitative analysis of in vivo studies due to the small number of included studies.
3.5. Internal Adaptation/Internal Gap
The internal discrepancy was defined by Holmes et al. as the perpendicular distance between the inner surface of the crown and the outer surface of the preparation under a 3D optical microscope [46]. Three studies measured internal adaptation [36, 42, 43]. Two studies [36, 43] reported no significant differences in internal adaptation in single-unit fixed prostheses fabricated with digital and conventional impressions, with a mean of 0.03 (-0.91, 0.96) micrometers and -0.17 (-0.53, - 0.20 micrometers) (Table 3). One study [42] reported an average of 0.32 micrometers (with a range of 0.08 to 0.56 micrometers), showing a better internal adaptation with digital impressions.
4. DISCUSSION
During the last decade, research has evaluated marginal and internal adaptation in single-unit fixed prostheses fabricated from a digital impression or a conventional impression, but the results have been contradictory, and the methods used to carry out these reviews have been unsatisfactory. Therefore, health professionals are basing their clinical decisions on unreliable studies. For this reason, the objective of this systematic review was to evaluate the methodological quality of the SRs currently published about the accuracy (marginal adaptation and/or internal adaptation) of full-coverage fixed prostheses made with digital impressions versus conventional impressions. AMSTAR 2 tool was applied to demonstrate the validity and reliability of each of these reviews.
When assessing the methodological quality of the SRs included in this study using the AMSTAR 2 tool, low reliability and low quality were found, especially in domains 3, 4, 10, and 16 of AMSTAR 2, since none of the SRs explained the selection of the study design, performed an exhaustive literature search, reported the sources of funding of the included studies, or reported the existence of possible sources of conflict of interest, including any funding received to conduct the review, considering these items in future SRs.
The studies included in the SRs showed high heterogeneity; some studies reported heterogeneity values above 75%, which is considered high. This can be explained by their use of different types of restorations [47] or laboratory fabrication techniques, types of scanner, amounts of spacer needed, preparation designs [48], and methods of measuring marginal adaptation (optical microscope [46, 49, 50], stereomicroscope, macroscope, or explorer). In addition, the majority of authors [51-56] used the silicone replica technique to measure the marginal fit of the crown before cementation, which is also a non-invasive practice with acceptable accuracy; however, this technique can lead to inaccuracies [43, 57].
Hasanzade et al. [43] performed an SR in 2019 that concluded single-unit fixed prostheses fabricated from a digital impression to show a better marginal adaptation than those fabricated from a conventional impression, while the internal adaptation did not show statistically significant differences between the two techniques. However, in 2020, Hasanzade et al. [42] performed another SR that found marginal adaptation and internal adaptation to be better with the digital approach than the conventional impression. This difference between the two studies can be because the first study did not specify the method used to make the crowns, while in the second study, fabrication was digital, and the scanners, design software, and dental milling machines were optimally combined and used to compensate for the error tolerance of each step [42, 43]
Table 2.
| Systematic Review | DI | CI | Reported Results | Studies for Comparison |
| Bandiaky et al. (2022), France, Journal of Prosthetic Dentistry [41] | -
|
-
|
Marginal fit: MD: -11.1 (C.I. = -32.5, 10.4), P > .05 |
Comparative studies, prospective (2), and randomized controlled clinical studies (14) |
| Chochlidakis et al. (2016), Journal of Prosthetic Dentistry [36] | |
|
Marginal discrepancy: MD: 0.24 (-0.32, 0.79), I2= 82.64%, P < .001 |
Clinical studies (2) and in vitro studies (9) |
| Hasanzade et al. (2021), Iran, Journal of Prosthetic Dentistry [42] |  |
 |
Marginal gap: MD: 0.25 (0.09, 0.59), l2 = 66.5%, P = .006 |
Clinical trials (8) and in vitro studies (21) |
| Hasanzade et al. (2019), Iran, Journal of Evidence Based Dental Practice [43] | |
|
Marginal gap: MD: -0.59 (C.I. = -0.93, - 0.24), l2 = 86%, P < 0.00001 | Prospective clinical trials (8) and in vitro studies (26) |
| Tabesh et al. (2021), Iran, Journal of Prosthetic Dentistry [44] | |
|
Marginal gap: MD: –0.89 (–1.24, –0.54), I2 = 78.2%, P < .001 |
Prospective clinical trials (8) and in vitro studies (11) |
| Tsirogiannis et al. (2016), Germany, Journal of Prosthetic Dentistry [45] | -
|
-
|
Discrepancy marginal in vivo: adjusted MD: 27.2 (C.I. = -5.3, 59.7), P = .084 | 4 in vivo studies |
| Discrepancy marginal in vitro: adjusted MD: -4.2 (C.I. = -33.0, 24.5), P = .763 | 8 in vitro studies |
| Systematic review | DI | CI | Reported results | Studies for comparison |
| Bandiaky et al. (2022), France, Journal of Prosthetic Dentistry [41] | |
|
Internal gap: MD: 0.03 (-0.91, 0.96), I2 = 92.22%, P < .0001 |
Comparative studies, prospective (2) and randomized controlled clinical studies (14) |
| Hasanzade et al. (2021), Iran, Journal of Prosthetic Dentistry [42] | |
|
Internal adaptation: MD: 0.32 (C.I. = 0.08, 0.56), I2 = 0.0%, P = .457 | Clinical trials (8) and in vitro studies (21) |
| Hasanzade et al. (2019), Iran, Journal of Evidence Based Dental Practice [43] | |
|
Internal gap: MD: -0.17 (C.I. = - 0.53, -0.20), l2 = 86%, P < 0.00001 | Prospective clinical trials (8) and in vitro studies (26) |
Tsirogiannis et al. [45] found no significant difference in the marginal discrepancy of single-unit ceramic restorations fabricated after digital and conventional impressions, either in vivo or in vitro studies. However, in the SR performed by Hasanzade et al. [43], they determined no significant differences between the digital and conventional groups in in vivo studies, but in in vitro studies, digital impressions resulted in better marginal adaptation. Mai et al. [58], in their SR, found the marginal adaptation values measured by digital methods to benominally higher but not significantly different from those measured by conventional methods in in vitro studies. Morsy et al. [59] found digital scanning to provide a significantly better marginal fit than conventional impression for fabricating fixed partial dentures of up to four units, either in monolithic form or structures and in any region of the arch.
Nagarkar et al. [51] indicated that, in marginal and internal adaptation, there were no significant differences between the impression techniques.
The clinical use of digital impressions is constantly increasing due to their various advantages. This technology eliminates the selection of trays and impression materials and facilitates electronic transfer, the storage of digital files, and in-office milling of final restorations [16]. The limitations of digital impressions include the additional costs related to the purchase of an intraoral scanner, the need to participate in courses and workshops, and the need to constantly update with advancing technology.
When performing this systematic review, it was observed that despite many SRs, there was an urgent need to establish a standardized protocol to improve the quality of their reporting using assessment tools, such as AMSTAR 2. In addition, it is suggested to improve the inclusion and exclusion criteria of future research, with the aim of increasing the methodological homogeneity of primary studies. Likewise, new primary studies (RCTs) should be done with high methodological rigor to yield more reliable results and high-quality SRs.
Future studies should have a standardized protocol regarding the type of restoration, preparation design, conventional impression material, laboratory fabrication technique, amount of spacer needed, type of scanner, and methods used to measure the marginal adaptation so that they can all compare marginal and internal fit in a similar way.
CONCLUSION
From the limitations of the SRs included in the present study, the following conclusions can be drawn.
- The methodological quality of published SRs is poor according to the AMSTAR 2 tool, making for low and critically low confidence. In addition, some reviews used the original MINORS scale to evaluate the methodological quality of their included studies, which has not been validated in terms of content or scoring.
- The studies included in the SRs showed high heterogeneity; the number of clinical studies in the SRs was small, which made it difficult for some SRs to perform a quantitative analysis of them, and some SRs included only studies in English.
- Half of the systematic reviews showed a better marginal adaptation with digital impressions, while the other half showed no significant differences between conventional and digital impressions.
- Internal adaptation was better with digital impressions in one SR, while two SRs did not show statistically significant differences between conventional and digital impressions.
LIST OF ABBREVIATIONS
| CAD/CAM | = Computer-aided design and manufacturing |
| SRs | = Systematic reviews |
| PRISMA-P | = Preferred reporting items for systematic reviews and meta-analytical protocols |
| INPLASY | = International Platform of Registered Systematic Review and Meta-Analytical Protocols |
| RCTs | = Randomized Clinical Trials |
| = PICO | Patient/Population, Intervention, Comparison, Outcomes |
| GRADE | = Grading of Recommendations Assessment, Development, and Evaluation |
| AMSTAR 2 | = A MeaSurement Tool to Assess Systematic Reviews |
| DI | = Digital Printing |
| CI | = Conventional Printing |
| MD | = Mean Difference |
| CI | = Confidence Interval |
CONSENT FOR PUBLICATION
Not applicable.
STANDARDS OF REPORTING
PRISMA guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the Zenodo at https://zenodo.org/record/7746657#.ZBS xxnbMLb0.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
ACKNOWLEDGEMENTS
The authors thank the Faculty of Dentistry of the University of Cuenca, Ecuador.
SUPPLEMENTARY MATERIALS
PRISMA checklist is available as supplementary material on the publisher’s website along with the published article.
APPENDIX
| Appendix A.SEARCH STRATEGY | ||
| P | - | - |
| PUBMED | ("posterior fixed" OR "dental porcelain"[Mesh] OR "single-unit" OR "crowns"[Mesh] OR "full-coverage restorations"OR "fixed prosthodontics" OR "fixed dental prostheses" ) |
36.99 5 |
| WOS | TÍTULO: ("posterior fixed" OR "dental porcelain"OR "singleunit" OR "crowns"OR "full-coverage restorations"OR "fixed prosthodontics" OR "fixed dental prostheses" ) |
6.440 |
| SCOPUS | TITLE-ABS-KEY ( "posterior fixed" OR "dental porcelain" OR "singleunit" OR "crowns" OR "full-coverage restorations" OR "fixed prosthodontics" OR "fixed dental prostheses" ) |
164,6 35 |
| GOOGLE SCHOLAR | ("posterior fixed" OR "dental porcelain" OR "single-unit" OR "crowns" OR "full-coverage restorations"OR "fixed prosthodontics" OR "fixed dental prostheses" ) | 939.0 00 |
| NEW YORK ACADEMIC OF MEDICIN |
- | - |
| GRAY LITERATUR E REPORT. |
("posterior fixed" OR "dental porcelain"OR "single-unit" OR "crowns"OR "full-coverage restorations"OR "fixed prosthodontics" OR "fixed dental prostheses" ) | 0 |
| I | - | - |
| PUBMED | ("digital" OR "digital scans" OR "digital impressions") | 148 |
| WOS | TÍTULO: ("digital" OR "digital scans" OR "digital impressions") | 204.3 77 |
| SCOPUS | TITLE-ABS-KEY ( "digital" OR "digital scans" OR "digital impressions" ) | 1 ,186, 959 |
| GOOGLE SCHOLAR | ("digital" OR "digital scans" OR "digital impressions") | 7.160. 000 |
| C | - | - |
| PUBMED | ("conventional impressions" OR "manual impressions" OR "conventional") | 501 |
| WOS | TÍTULO: ("conventional impressions" OR "manual impressions" OR "conventional") | 75.25 9 |
| SCOPUS | TITLE-ABS-KEY ( "conventional impressions" OR "manual impressions" OR "conventional" ) | 1 ,706, 645 |
| GOOGLE SCHOLAR | ("conventional impressions" OR "manual impressions" OR "conventional") | 5.790. 000 |
| O | - | - |
| PUBMED | ("accuracy" OR "adaptations" OR "dimensional accuracy" OR "marginal fit" OR "internal fit" OR "adjustment") |
650.3 26 |
| WOS | TÍTULO: ("accuracy" OR "adaptations" OR "dimensional accuracy" OR "marginal fit" OR "internal fit" OR "adjustment") | 158.2 62 |
| SCOPUS | TITLE-ABS-KEY ( "accuracy" OR "adaptations" OR "dimensional accuracy" OR "marginal fit" OR "internal fit" OR "adjustment" ) | 3 ,108, 658 |
| GOOGLE SCHOLAR | ("accuracy" OR "adaptations" OR "dimensional accuracy" OR "marginal fit" OR "internal fit" OR "adjustment") |
5.970. 000 |
| S | - | - |
| PUBMED | ("systematic review and meta-analysis" OR "systematic review" OR "meta- analysis") | 306.0 94 |
| WOS | TÍTULO: ("systematic review and meta-analysis" OR "systematic review" OR "meta- analysis") | 232.0 01 |
| SCOPUS | TITLE-ABS-KEY ( "systematic review and meta-analysis" OR "systematic review" OR "meta- analysis" ) | 457,2 26 |
| GOOGLE SCHOLAR | ("systematic review and meta-analysis" OR "systematic review" OR "meta- analysis") | 17.80 0 |
| - | - | |
| PUBMED | ("posterior fixed" OR "dental porcelain"[Mesh] OR "single-unit" OR "crowns"[Mesh] OR "full-coverage restorations"OR "fixed prosthodontics" OR "fixed dental prostheses" ) AND ("digital" OR "digital scans" OR "digital impressions") AND ("conventional impressions" OR "manual impressions" OR "conventional") AND ("accuracy" OR "adaptations" OR "dimensional accuracy" OR "marginal fit" OR "internal fit" OR "adjustment") AND ("systematic review and meta-analysis" OR "systematic review" OR "meta- analysis") |
17 |
| WOS | TEMA: ("posterior fixed" OR "dental porcelain"OR "singleunit" OR "crowns"OR "full-coverage restorations"OR "fixed prosthodontics" OR "fixed dental prostheses" ) AND TEMA: ("digital" OR "digital scans" OR "digital impressions") AND TEMA: ("conventional impressions" OR "manual impressions" OR "conventional") AND TEMA: ("accuracy" OR "adaptation s" OR "dimensional accuracy" OR "marginal fit" OR "internal fit" OR "adjustment") AND TEMA: ("systematic review and metaanalysis" OR "systematic review" OR "meta- analysis") |
19 |
| SCOPUS | ( TITLE-ABS-KEY ( "posterior fixed" OR "dental porcelain" OR "singleunit" OR "crowns" OR "full-coverage restorations" OR "fixed prosthodontics" OR "fixed dental prostheses" ) AND TITLE-ABS-KEY ( "digital" OR "digital scans" OR "digital impressions" ) AND TITLE- ABS-KEY ( "conventional impressions" OR "manual impressions" OR "conventional" ) AND TITLE-ABS-KEY (( "accuracy" OR "adaptations" OR "dimensional accuracy" OR "marginal fit" OR "internal fit" OR "adjustment" ) AND TITLE-ABS-KEY ( "systematic review and metaanalysis" OR "systematic review" OR "meta- analysis" ) |
18 |
| GOOGLE SCHOLAR | in title: ("crowns") AND ("digital impressions") AND ("conventional impressions") AND ("accuracy") AND ("systematic review and meta- analysis") |
77 |
| NEW YORK ACADEMIC OF MEDICIN GRAY LITERATUR E REPORT. |
("crowns") AND ("digital impressions") AND ("conventional impressions") AND ("accuracy") AND ("systematic review and meta- analysis") | 0 |
| Appendix B. Articles excluded from the study | |
| Study | Reason for exclusion |
| [Ahlholm P et al. 2018] | 2 |
| [Ahmed WM, et al. 2020] | 1 |
| [Al-Haj Husain N, et al. 2020] | 2 |
| [Arcuri L, et al. 2019] | 3 |
| [Carvalho T, et al. 2018] | 1 |
| [Chandran S, et al. 2019] | 2 |
| [Cicciù M, et al. 2020] | 4 |
| [Gallardo Y, et al. 2018] | 4 |
| [Giachetti L, et al. 2020] | 2 |
| [Kumar H, et al. 2020] | 4 |
| [Kyoung-Rok Kim, et al. 2018] | 4 |
| [Mai H, et al. 2020] | 4 |
| [Nagarkar S, et al. 2018] | 4 |
| [Papadiochou S, et al. 2017] | 2 |
| [Pecciarini M, et al. 2019] | 2 |
| [Svanborg P, et al. 2020] | 2 |
| 1 | Systematic reviews of the literature, case reports, pilot studies |
| 2 | Studies evaluating seating in implant crowns and partial restorations |
| 3 | Studies without response from the author to the information query requested |
| 4 | Systematic reviews that do not meet the PICO question |
| Appendix C. AMSTAR 2 assessment criteria and domains | |||||||||||||||||
| Study | Q 1 | Q 2 | Q 3 | Q 4 | Q 5 | Q 6 | Q 7 | Q 8 | Q 9 | Q 10 | Q 11 |
Q 1 2 |
Q 13 | Q 14 | Q 15 | Q 16 | Overall confiance |
| Bandiaky ON, et al. 2020 | Y | Y | N | N | Y | N | N | P Y | N | N | Y | Y | N | Y | Y | N | Low |
| Chochlidakis KM, et al. 2016 | Y | P Y | N | N | Y | N | N | P Y | N | N | N | Y | N | N | N | N | Critically low |
| Hasanzade M, et al. 2020 | Y | Y | N | N | Y | N | N | P Y | N | N | N | Y | N | Y | Y | N | Low |
| Hasanzade et al. 2019 | Y | P Y | N | N | Y | Y | Y | P Y | P Y | N | N | Y | Y | N | N | N | Low |
| Tabesh et al. 2020 | Y | Y | N | N | N | N | N | N | N | N | N | NM A | N | Y | N | N | Critically low |
| Tsirogiannis et al. 2016 | N | N | N | N | N | N | N | P Y | N | N | N | Y | Y | Y | N | N | Critically low |
| Y | YES | ||||||||||||||||
| N | NO | ||||||||||||||||
| PY | PARTIAL YES | ||||||||||||||||
| NMA | NO META- ANALISIS | ||||||||||||||||

