All published articles of this journal are available on ScienceDirect.

“Canine First Technique”, An Innovative Approach in Maxillary Impacted Canines: A Case Report
Authors Info & Affiliations
Abstract
Background:
Maxillary canine impaction is one of the most challenging issues in orthodontics. The best treatment protocol in these cases is still debated. The purpose of this study is to describe the management of maxillary canine impaction in an adult female patient with the “Canine First Technique”.
Case Report:
A 21-years-old female attended our dental unit seeking orthodontic treatment. Clinical examination revealed a class II relationship, the persistence of both upper deciduous canines. The panoramic X-ray and Cone Beam Computed Tomography showed bilateral palatal permanent canine displacements and close proximity between crowns of impacted canines and roots of lateral incisors. The canines were disimpacted by means of two cantilevers inserted directly in two Temporary Anchorage Devices placed palatally and when canines were near the crest, the fixed orthodontic treatment was started.
Results:
At the end of the treatment, canine Class I relationships with torque correction of canines, normal overjet and overbite, and good alignment of dental arches were achieved. The radiographic evaluation showed ideal root parallelism and preserved periodontal health in the canine region.
Conclusion:
The Canine First Technique could provide some advantages compared to conventional approaches in terms of biomechanics, esthetics, oral hygiene, and risk reduction of root resorption of upper lateral incisors.
1. INTRODUCTION
The permanent canines are the key to an aesthetic smile and functional occlusion [1]. Maxillary canine impaction incidence in the population is 1- 3% [2], and in 85% of cases, the impacted canine is palatal [3]. The etiology of maxillary impacted canine is still unknown, but a multifactorial and genetic origin was hypothesized [4]. As Becker and Chaushu suggested [5], the causes of impacted canines can be divided into 4 categories: local pathology, genetic and hereditary factors, local obstruction, and anomaly of the normal eruption of lateral incisors.
Considering the patient’s age, an intraoral clinical examination is the first step in formulating a correct diagnostic hypothesis. Indeed, some clinical signs could give the suspicion of the presence of an impacted canine: i.e., the permanence of deciduous canine beyond 14 to 15 years old of age, the absence of a canine bulge or its palatal appearance, and a deviation of the normal tip of the lateral incisors [6]. The palpation of alveolar bone is made on both the palatal and buccal side of the alveolar process in the canine region. The absence of a palpable bulge is considered abnormal and the presence of a little concave contour of the alveolar bone mesial to the deciduous canine can reveal an anomaly of eruption [7].
In addition to the clinical examination, radiographs are very important to perform a correct diagnosis [8]. Panoramic radiographs are suggested for early prediction of maxillary impacted canine from 8 years old and are also recommended in older children (>11yr) without erupted canines if the canine’s bulge is impalpable [9]. The use of cone beam computed tomography allows a more effective evaluation of the position of impacted canines and leads to the development of more efficient biomechanics [10, 11].
A multidisciplinary approach is necessary for the treatment of the impacted canine. In the literature, different treatment options for maxillary canine impaction are available [12-14]. However, there is still no absolute consensus on the best treatment protocol for these cases. The aim of this study is to describe a case treated in our department with an innovative surgical-orthodontic approach called “Canine First Technique”.
The Canine First Technique consists of an innovative surgical-orthodontic approach for the impacted canine. This procedure provides the disimpaction of the canine moving the crown away from the roots of adjacent incisors with a cantilever and a skeletal anchorage. This technique was developed in recent years in the School of Orthodontics at the University of Naples “Federico II”, so there are no other papers in the literature describing it.
2. CASE REPORT
A 21-years old female attended our department seeking an orthodontic treatment referred by her general dentist. She complained about the absence of permanent maxillary canines and expressed the will to possibly receive an esthetic orthodontic treatment to solve this problem.
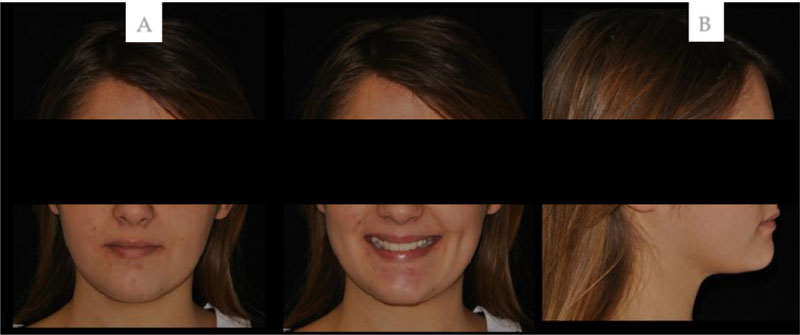
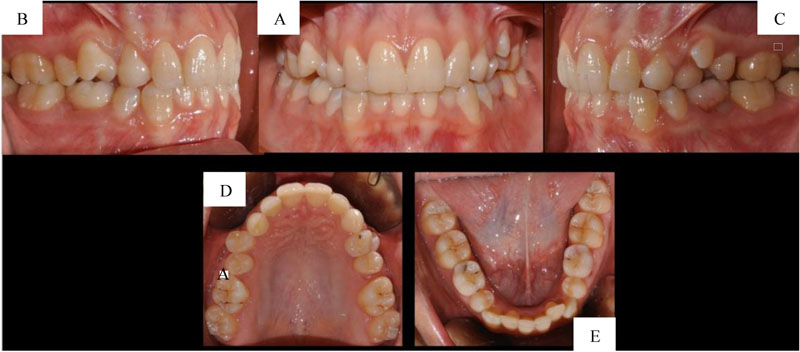
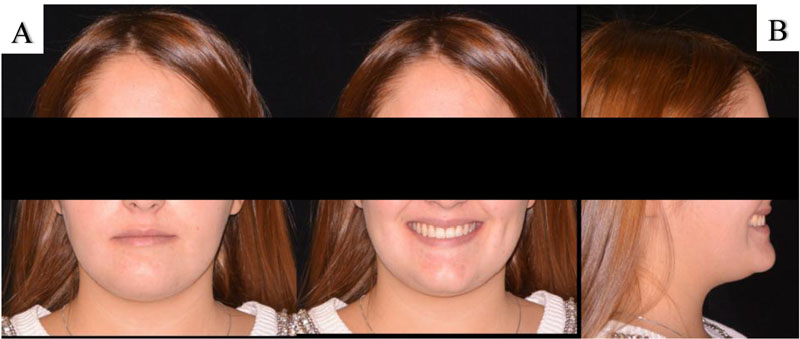
The patient had a symmetric and oval face, a slightly convex profile, and a normal nasolabial angle. Clinical examination revealed edge-to-edge molar Class II relationship, the persistence of deciduous teeth including both deciduous canines, mild crowding of both arches, normal overjet and slightly increased overbite (Figs. 1 and 2). There was a coincidence between the facial and upper dental midline, while the lower dental midline was deviated by 2mm to the left side.
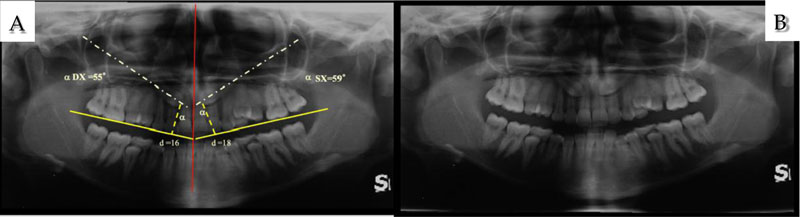
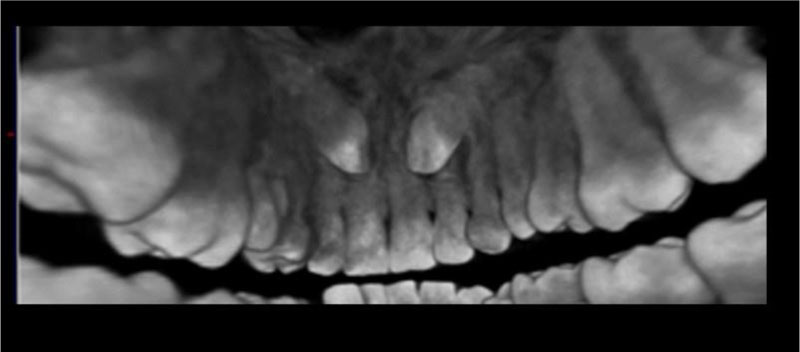
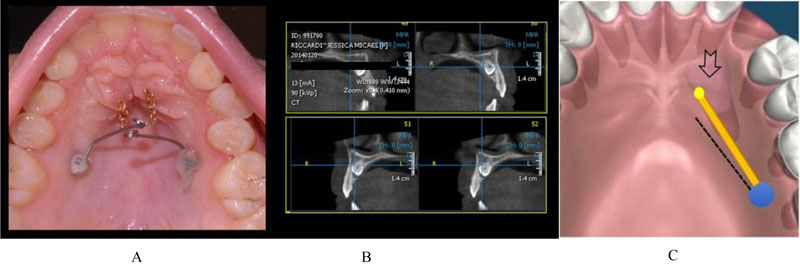
Extraoral and intraoral photographs, study models, intra-oral periapical radiographs, lateral cephalometric radiograph, panoramic radiograph, functional examination and Cone Beam Computed Tomography (CBCT) of the maxillofacial region were conducted. Imaging was provided by the patient and included different protocols of acquisition. The three-dimensional reconstruction of the CBCT DICOM files was performed with dedicated software (Amira, Thermo Fisher Scientific, Waltham, Massachusetts, USA). Models analysis confirmed the clinical findings. Cephalometric analysis revealed skeletal Class I and normal axial inclination of upper and lower incisors. The panoramic X-ray showed bilateral palatal permanent canine displacement in sector four with an alpha angle of more than 45 degrees (Fig. 3) by Ericson and Kurol classification [15]. The CBCT showed bilateral palatal permanent canine displacement and close proximity between the crown of the impacted canine and roots of incisors (Fig. 4).
The rationale of the Canine First Technique is based on the observation of close proximity between the palatal impacted canine and roots of other teeth. Indeed, this technique allows the application of a force statically determinable in magnitude, line of action and direction, which is very important in canine disimpaction. In this case, in fact, the use of a fixed appliance could produce non-predictable reaction forces on the other teeth, increasing the risk of resorption of the roots of the lateral incisors: the placement of brackets on the maxillary lateral incisors could have to lead their roots closer to the canines crowns, in particular when rectangular archwires were inserted and palatal root torque was expressed.
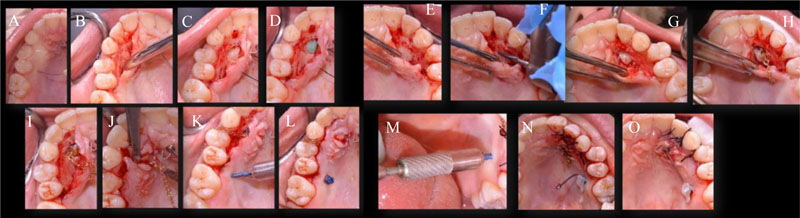
This approach consists first of the surgical crown exposure of the impacted canines by means of a local anaesthetic infiltration and a full-thickness mucoperiosteal flap (Fig. 5). An orthodontic button with a wire chain was bonded on the crown, and then the orthodontic traction of canine was performed exclusively by means beta-titanium cantilever 0.19x.025, inserted into a miniscrew type 11 mm in length, 1.4 mm in diameter (OrthoEasy® Pins, Forestadent Bernhard Förster GmbH, Pforzheim, Germany) placed in a palatal safe zone (Fig. 5) without the need of fixed orthodontic appliance. In this case, the insertion sites of the two miniscrews were about 5mm from the embrasure between the second premolars and first molars. Two cantilevers in TMA wire (Ormco, Glendora, California, USA) were inserted in the miniscrews and activated in distalization and extrusion to ward off the crowns of the impacted canines from the roots of upper incisors because of their close proximity (Fig. 6). These forces were activated monthly and after 5 months, canine bumps were visible in the centre of the palate. At this stage, a second minimal surgical exposure (gingivectomy) was performed and the vector of activation on the cantilever was changed in extrusion and in vestibular direction (Fig. 7). After 8 months from the surgical exposure, only through the cantilever activation, both permanent canines were near the crest; in this phase, deciduous canines were extracted and orthodontic treatment with fixed .022x.028 multibracket appliance (Mini Sprint®, Forestadent Bernhard Förster GmbH, Pforzheim, Germany) was started. Both maxillary canines were bonded with braces having -17 torque prescription to obtain a good torque correction (Fig. 8). Superelastic nickel-titanium (NiTi) and Stainless Steel (SS) archwires (BioStarter® / BioTorque®, Forestadent Bernhard Förster GmbH, Pforzheim, Germany) were used in this sequence: 0.014 NiTi; 0.014x0.025 NiTi; 0.019x0.025 NiTi; 0.019x0.025 SS; 0.021x0.025 SS. When the canines achieved the correct position in the upper arch, there was also a need to use Class II elastics on the 019x025 SS wire to correct the slight molar and canine Class II relationship.


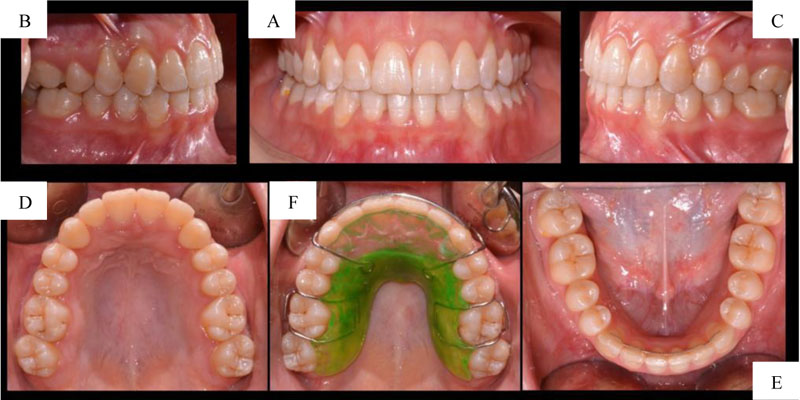
Total treatment duration was 29 months. Post-treatment images showed molar and canine Class I relationships, with normal OVJ and OVB, good alignment of dental arches, torque correction of canines and dental midlines coinciding with the facial midline (Fig. 9). The radiographic evaluation showed ideal root parallelism, preserved periodontium, and bone tissues health in canine region. Retention was provided by upper Hawley biteplate and lower 3-3 bonded lingual retainer (Figs. 10 and 11).

3. DISCUSSION
The aim of this case report was to describe the management of maxillary canine impaction with an innovative approach, the “Canine First Technique”.
The traditional approach with fixed appliances required archwires to align and level the upper arch [16]. This procedure is still widely used by a large number of orthodontists [17] but has several disadvantages and side effects, such as the uncontrolled movement of the apex of incisors when the interaction between braces and rectangular archwire occurs, often resulting in root resorption of the incisors adjacent to the impacted canine [18]. On the other hand, the biomechanics of the cantilever on the Temporary Anchorage Device is determined to force the system, meaning that the forces and the moments can readily be measured and evaluated [19]. Therefore, this allows the canine to be displaced in a predictable and safe movement away from the roots of other teeth before bonding the multibrackets appliance.
Furthermore, the Canine First Technique could provide other advantages. With this approach, it is not necessary to apply the fixed orthodontic appliance until the eruption of the impacted canine, preserving also deciduous canines. This compromises the patient's aesthetics less, which is very important, especially in adult patients with higher demand [20]. In addition, the reduction of time with fixed appliances permits better oral hygiene, preventing the onset or worsening of gingivitis and periodontal disease [21, 22]. Moreover, the absolute anchorage obtained with miniscrews avoids several side effects that may occur with dental anchorage. For example, a cantilever inserted on the buccal side of the upper first molar for canine disimpaction could cause molar flaring, molar intrusion, molar mesial tipping, and tilt of the occlusal plane [23]. These side effects may be even more evident and exacerbated in cases of ankylosis of the impacted canines. The ankylosis of impacted canines is a condition impossible to predict and is more frequent in adult patients [24]. Therefore, in these patients, the use of a skeletal anchorage assumes even greater importance. In conclusion, the use of Temporary Anchorage Devices provides absolute anchorage with a reduction in treatment time and dental undesirable movements, minimum discomfort, high biocompatibility, and better aesthetics [25]. For all these reasons, this technique could improve patients’ compliance.
The limitation of this study was that it is only a case report that can be considered a pilot study to show the characteristics of this technique. A controlled clinical trial would be necessary to validate this protocol. A study with a large sample of patients could add validity to the clinical experience presented in this paper.
CONCLUSION
The Canine First Technique could provide some advantages compared to conventional approaches in terms of biomechanics, esthetics, oral hygiene, and risk reduction of root resorption of upper lateral incisors.
LIST OF ABBREVIATIONS
| CBCT | = Cone Beam Computed Tomography |
| NiTi | = Nickel-Titanium |
| SS | = Stainless Steel |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
The patient gave informed consent for the publication of the study.
STANDARDS OF REPORTING
CARE guidelines have been followed.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the manuscript.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

