All published articles of this journal are available on ScienceDirect.

Dental Curriculum's Continuing Improvement in the North American and Gulf Cooperation Council (GCC) Education Systems
Abstract
Background:
Dynamic oral health care needs, alongside a diverse demographic of patients, presents a challenge to dental clinicians as they strive to resolve the ever-increasing demand for quality oral care service. Claims have arisen that the most appropriate way of speeding up the slow change in adopting innovations within the dental practice is by updating dentists' knowledge and skills through improving the undergraduate students' curriculum.
Objective:
This review compares the dental curriculum's continuing improvement processes between the North American and Gulf Cooperation Council (GCC) countries.
Methods:
The process of analysis consisted of identifying, examining, and interpreting patterns and themes within textual data, and then determining how each of these help answer the research questions.
Results:
Efforts to implement the dental curriculum's continuous improvement processes in the North American and GCC countries are evident, but the significant barriers for the dental curriculum's continuing improvement among the North American countries include the consequences of a compressed four-year curriculum, reliance on professional regulations, insufficient focus on patient perceptions, and the lack of a more theoretically robust approach to self-reflection. Conversely, amongst the GCC countries, the available literature states that the most significant factors hindering the dental curriculum's continuing improvement include deficient leadership attributes and low research productivity.
Conclusion:
The North American and GCC regions will benefit from the new dental curriculum and result in producing more competent dental practitioners, with improved leadership and patient-centered care. However, it has been observed that the dental curriculum’s continuous improvement processes are adopted slowly, particularly among the GCC countries.
1. INTRODUCTION
The dental industry is faced with wide-ranging oral conditions and complexities that trigger innovation and research [1-3]. Also, the dynamism of oral health care needs, coupled with a diverse demographic of patients, as seen in North America and the Persian/Arabian Gulf, presents a challenge to dental practitioners striving to meet the demands of a population expecting quicker and higher quality oral care services [4, 5]. As a result, the generation of scientific knowledge and new technologies, and advances in drug production to provide more efficient treatment have increased exponentially. One of the most exciting development trends in the industry is the rise of laser technology [6]. that has caused a drastic shift from traditional routine dental care, which required invasive and painful treatments, to modern laser dentistry. Students in Iran have shown a positive attitude towards incorporating an independent laser credit in their curriculum [7]. whereas in the US, only 24% of dental curricula cover hard tissue lasers [8]. Other important recent technological developments in dentistry include 3D imaging in orthodontics, prosthodontics, endodontics, esthetic, and implant dentistry, with comprehensive digital treatment planning [9-14]. Also, it is recommendable to include radiation-free diagnostic tests (e.g., magnetic resonance imaging (MRI) in dentistry [15]. and furthermore, intraoral impressions and the confection of the dental prostheses have also turned digital with scanning and CAD/CAM, respectively [16-18]. Dental practitioners are repeatedly seen as being slow to adopt emerging technologies, knowledge, treatment modalities, and staying on top of digital trends, whilst the dental industry itself has shown repeated concerns about embracing technology to enhance treatments and oral care services [1, 8, 19, 20]. In other words, only a small fraction of dental practitioners are considered early adopters.
The most appropriate way to rapidly implement the change needed in adopting innovations within the dental curriculum is by generating new knowledge and improving dental students' skills [21]. While stakeholders have accepted this fact globally, it is not surprising that the dental curriculum's improvement process varies significantly across geographical regions.
The explicit focus on quality in dental education is slightly recent. Typically, the continuous quality improvement of programs is closely associated with the curriculum assessment process [22]. and undeniably, health professional programs are more often required to become involved in continuous quality improvement procedures [23]. Promoting a continuous quality improvement philosophy must be the basis of educational accreditation systems. An implemented continuous quality improvement philosophy could guarantee a dental school’s constant self-evaluation and best teaching practices [24].
This short communication mini-review compared the dental curriculum's continuing improvement processes between the North American and the Cooperation Council for the Arab States of the Gulf Gulf (commonly known as Gulf Cooperation Council (GCC) countries. The specific objectives were:
- To identify trends of continuing improvement in the North American and GCC countries' dental curriculum.
- To compare the dental curriculum's continuing progress between North American and GCC countries.
- To identify factors influencing the differences between the North American and GCC countries’ dental curriculum's continuing improvement.
2. METHODS
The present article reviewed dental education literature that reported information on the North American and GCC curricula’s continuing improvement. This study involved a synthesis of quantitative findings stemming from both qualitative and quantitative research studies [25]. As qualitative research data are usually not amenable to counting or measuring [26], quantitative approaches provide numerical and statistical evidence to answer the present research question.
The current article aims to review the interpretations made by different authors of the literature regarding the dental curriculum’s continuing improvement in North American and GCC countries.
3. RESULTS
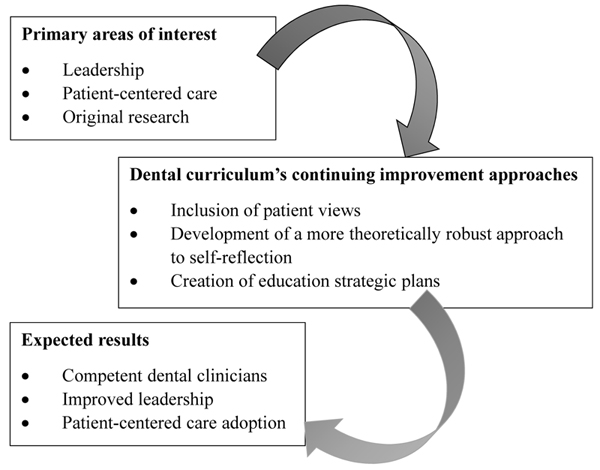
In general, positive trends were identified in both the North American and GCC countries, and it was revealed that numerous efforts had been implemented to secure continuous improvement processes for the dental curriculum. Moreover, Patrick (2017) reviewed the current developments in the delivery of dental ethics education, with a deliberate focus on developing new pedagogies and curricula content in the US, and revealed that the US and its neighboring countries had made great strides towards improving the teaching of ethics in dental education [27]. However, the output is not yet significant; it is necessary to include patient views and develop a more theoretical approach to self-reflection (Fig. 1).
GCC countries have also shown significant efforts in improving the dental curriculum. In a study on the development of dental curriculum for the 21st Century in Saudi Arabia, Al-Madi et al. (2018) presented a recommendation of a contemporary dental curriculum deemed internationally competitive [21]. However, the curriculum focused on the specific needs of the communities living in GCC countries, rather than on an entire country or the region as a whole. The dental department's accepted approach to curriculum development aimed to identify problems, objectives, educational strategies, and needs – both specific and general. The study identified three major areas that required urgent improvement: leadership attributes, patient-centered care, and research.
Different factors influence the dental curriculum’s continuing improvement in North America when compared with the GCC region. According to Patrick (2017), the primary challenge for the ethical development of students and dental curriculum’s continuing improvement in the US includes the consequences of a squeezed curricula and the reliance on professional regulations [27]. Among North American dental institutions, a failure to include patient views, and the lack of a more theoretically robust approach to self-reflection, has also contributed to curriculum’s slow continuing continuing improvement. Additionally, after reviewing the literature, a twofold output in dental curriculum improvement research in North American dental institutions can be highlighted when compared to GCC institutions.
4. DISCUSSION
The study revealed that North American countries have significantly advanced the teaching of ethics in dental education. However, it is too early to decide whether the output is significant. According to Patrick (2017), the dental curriculum improvement procedures among North American countries missed an opportunity to include patient views and develop a more theoretically robust approach to self-reflection [27]. The slow process was linked to certain areas still not addressed by relevant stakeholders, coupled with the numerous challenges facing the improvement process.
The quality of leadership attributes among the GCC countries was a significant barrier to the dental curriculum’s continuing improvement. The rising interest in leadership while developing the curriculum is recognized, although insufficient research is a key reason for the slow dental curriculum’s continuing improvement. Research has numerous benefits in the development of a curriculum. For instance, Al-Madi et al. (2018) observed that cultivating a research-based approach to developing a practice provides evidence to effect change in the teaching process, the classroom, the schools, and beyond [21]. According to the study, there was notably more research productivity in dental curriculum development in the North American region compared to the GCC region.
CONCLUSION
Numerous efforts have been made in North American and GCC dental institutions to adopt and maintain the dental curriculum’s continuous improvement processes. The two regions consider the new dental curriculum to enhance dental practitioners' competency, improve leadership, and efficiently promote patient-centered care. However, it has been observed that the dental curriculum’s continuous improvement processes are slowly adopted, particularly among the GCC countries.
Overall, in North American countries, the major challenge in the dental curriculum’s continuing improvement includes:
- A crammed curriculum
- Over-reliance on professional regulations
- A minimum focus on patient-reported outcome measures (PROMs)
- Lack of a more theoretical approach to self-reflection.
Conversely, the primary reported factors hindering the dental curriculum’s continuing improvement among dental institutions in GCC countries include suboptimal leadership attributes and low research productivity.
AUTHORS' CONTRIBUTION
Henry Ghanem also performed validation, visualization, writing of the original draft, and review & editing. Kelvin Ian Afrashtehfar contributed to conceptualization, formal analysis, investigation, project administration, validation, visualization, and original draft preparation. Jose Calvo took part in editing.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

