All published articles of this journal are available on ScienceDirect.

The Restoration of Severe Generalized Dental Erosive Wear using Direct Composite: A Case Report
Abstract
Introduction:
This case report describes a conservative restorative approach in the management of severe generalized tooth wear.
Case report:
The male, aged 57 years, was mainly concerned with the poor appearance of his teeth with short and discolored upper incisors. History revealed that he suffered from gastric reflux for 25 years, for which he was prescribed Ranitidine and was advised to self-medicate with cider vinegar. Furthermore, he divulged that he ground his teeth at night and during the day and had a high intake of carbonated cola drinks. On examination, dentine was exposed in several areas, and to a significant extent, on the incisal aspects of the lower incisors, the palatal surfaces of the upper incisors, and the occlusal surfaces of the molars. Mandibular tori were present.
The primary diagnosis was erosive tooth wear with elements of attrition and abrasion. The intervention included dietary advice and restoration with direct composite resin at an increased occlusal vertical dimension of 1.5mm on the retruded axis. The patient reported no functional problems and was pleased with the aesthetic result.
Conclusion:
Vinegar is promoted to have health benefits, especially with respect to glucose response, but the dental implications are overlooked. This paper reviews the literature on vinegar as a medicament and considers its role as a co-factor for erosion in this case. The clinical steps used to restore the eroded dentition by direct composite are described. The use of this approach is a safe, conservative and successful treatment option without recourse to complex and biologically costly conventional alternatives. The application of direct composite in tooth wear cases meets the European consensus requirements.
1. INTRODUCTION
Tooth wear is described as the loss of dental hard tissues from the surfaces of the teeth caused by factors other than dental caries, trauma, and developmental disorders [1]. Attrition (direct tooth to tooth contact wear), abrasion (mechanical rubbing wear), and erosion (acid dissolution excluding bacterial acidic metabolites) can all lead to tooth wear, having a multifactorial etiology. It can be presented as generalized throughout the dentition or localized to the incisor and canine teeth [2]. The prevalence of tooth wear, according to the most recent UK Adult Dental Health Survey (2009), found 77% of the adults with wear in the anterior region, whilst 15% had moderate wear, and 2% had severe wear [3]. Tooth wear is more commonly seen in males than females in the ratio 2.3:1 [4].
In severe tooth wear cases, the teeth become short with compensatory tooth eruption and alveolar bone growth,which maintains contact with the opposing dentition or without compensation [5]. Conventional management of tooth wear, such as tooth preparation, to create interocclusal space for the crowns, may compromise the vitality of the pulp. Furthermore the teeth are already clinically short, which, in turn, reduces the resistance and retention form of the crown. Hence, restorative management of these cases is challenging [6].
The European expert consensus in 2017 proposed that indirect restorative interventions, such as crowns and veneers, should be delayed for as long as possible, and recommended an additive direct minimally invasive approach, such as direct composite restoration [7].
2. PATIENT INFORMATION AND RELEVANT HISTORY
This case report follows the CARE guideline [8]. A 57-year-old British male presented to Hamdan Bin Mohammed College of Dental Medicine, who was concerned about the appearance of his teeth. The only relevant medical history was that he suffered from Gastro-Esophagealreflux Disease (GORD) for 25 years, for which he self-medicated with Ranitidine for 10 years, a histamine H2 antagonist. He took 300mg, the normal daily dose, regularly without medical supervision. Further questioning revealed that the patient had a high intake of carbonated cola or fizzy cola drinks as he had previously worked for a drinks manufacturing company for 25 years. He also admitted to bruxism. After the examination and on further questioning regarding diet and habits, the patient stated he drank apple cider vinegar after listening to a healthcare expert on the radio stating the health benefits of apple cider vinegar and that it reduced gastric reflux. Thereafter, the patient started diluting apple cider vinegar with water and drank a glass every morning over the previous 2 years.
3. CLINICAL FINDINGS AND MANAGEMENT
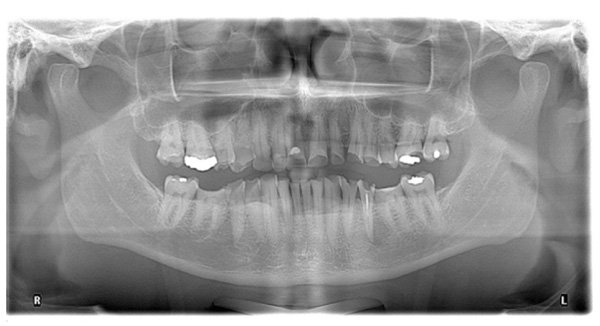
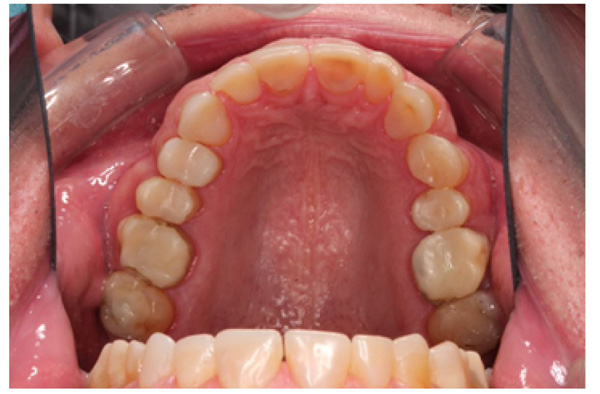
The patient presented with competent lips, an average lip line, normal TMJ function, and a mild Class II Division I incisor relationship with an increased overbite. The preoperative pan-oral radiograph is shown in Fig. (1). Boney exostoses and a large mandibular torus in the lower right mandible were present. The intra-oral presentation of the teeth is shown in Figs. (2-6). The patient had good oral hygiene and a healthy periodontium. The teeth had a glossy, smooth, and glazed appearance, showing cupping of the occlusal surfaces with significant loss of hard tissue and yellow color from the underlying dentine. This presentation was indicative of severe generalized tooth wear with exposed dentine in all sextants. The palatal, occlusal, and incisal surfaces were mainly affected, with lower buccal surfaces exhibiting more wear than the lower lingual, resulting in a reverse curve of Monson. The maximum BEWE score of 18 was recorded, meaning that the tooth with the most severe wear in each sextant had greater than 50% surface loss [9]. Several posterior teeth had amalgam restorations with defective margins (FDI 16, 26, 27, 37, and 47), as shown in Figs. (5 and 6). All teeth responded normally to pulp sensibility tests (cold test). The radiographs did not show any apical pathology to be present, but the pan-oral shows the scooped-out appearance of the lower molars.





The patient was diagnosed with severe generalized tooth wearwith a significant acid erosion component. The multifactorial risk factors included acid erosion from drinking carbonated cola beverages and apple cider vinegar, plus the history of GORD. Stress-related parafunction or bruxism was also present. A detailed explanation of the risk factors and their consequences was given to the patient. The patient was advised to stop the intake of all acidic drinks and was monitored for 3 months. After this period, the patient was keen to proceed with rehabilitation but desired cost-effective care as he did not have private insurance and could not afford expensive treatment. To avoid costly laboratory work, informed consent was, therefore, gained for treatment using direct composite. Upper and lower impressions in alginate (irreversible hydrocolloid) and a facebow record were taken. The casts were mounted andarticulated on a Denar Mark II semi-adjustable articulatorin maximum intercuspation or Centric Occlusion, which in this case coincided with Retruded Contact Position or Centric Relation.A diagnostic wax-up was performed to enable the build-up of the correct contour of the upper and lower teeth to facilitate the restorative rehabilitation (Fig. 7). An increase of 1.5mm in the vertical dimension at the incisors was planned by raising the pin and opening on the retruded axis of rotation to provide sufficient space for adhesivedirect hybrid composite restorations. A vacuum-formed Essix-type stent or matrix was fabricated on a stone duplicate of the diagnostic wax-up. The Dahl approach was not chosen because the wear was not only confined to the anterior teeth, as most of the teeth required build-ups [10]. Treatment planning involved a decision on which teeth to restore first. The first sextant for restoration was the lower anterior, then the upper anterior, followed by the lower posterior ones and finally the upper posterior teeth. This agreed with the recommendation proposed by Dawson to establish anterior guidance first, with the lower incisors in effect being supporting cusps and the upper anterior palatal surfaces being guiding cusps [11]. A single tooth at a time was restored within each sextant.

A low-speed carbide round bur was used to roughen the dentine before acid etching both enamel and dentine for 20 seconds using the total-etch technique [12]. The etched surface was washed, and gently air-dried.The 3M Espe Single Bond Universal adhesive was applied as per manufacturer’s recommendations by rubbing it for 20 seconds, air drying for 5 seconds,followed by polymerization using an Acteon mini LED light cure for 10 seconds. Cotton wool rolls and high-volume suction provided moisture control. After washing and drying, PTFE tape was placed as an interdental separator on either side of the tooth to be built up, followed bythe application of bonding resin and curing [13].
IPS Empress Direct ® (Ivoclar Vivadent, Schaan, Liechtenstein) composite was syringed onto the worn surface and into the stent,which was seated onto the tooth. The composite was cured through the stent for 20 seconds; then the stent was removed, and the composite curing light was used again to ensure afull set for a further 40 seconds. The PTFE tape was removed, the excess composite at the gingival margin was trimmed back with narrow and ultra-fine diamond finishing burs, and a final polish was performed using Shofu Super-Snap Rainbow® discs (Kyoto 605-0983, Japan). The resultsare shown in Figs. (8-10). The slight increase in the vertical dimension is seen when comparing the pre-operative frontal image (Fig. 2) with the post-op image (Fig. 8), where some of the labial surfaces of the lower incisors is now visible, which was planned from the outset.
The occlusal scheme was created using a mutually protected occlusion with canine guidance. The patient was informed of possible transitory problems, including difficulty in eating or speaking and other possible discomforts. He was reassured that adaptation is usually quick. Alower bilaminar (dual-laminate) night guardof 3mm thickness was provided in order toprotect the composites during bruxism [14]. He was followed up for 4 months after completion of all the restorations to find out at which time he had adapted perfectly well and was functioning normally. He waspleased with the esthetic result but was warned that composites could get stained by foods and drinks such as tea, coffee, and curry (mainly turmeric). However, he was reassured that the surface stain was easily polished off.


4. DISCUSSION
Gastroesophageal reflux disease (GORD) is a common disease worldwide with increasing prevalence, especially in the 30-39 year age group [15]. Oral signs of GORD includes dental erosion, dry mouth, burning sensation, halitosis, erythema of the palatal mucosa and uvula [9]. Dentists can, therefore,be the first healthcare provider to encounter patients with undiagnosed GORD. The relationship between GORD and dental erosion has been thoroughly reviewed by Moazzez and Austin [16]. Although the chief complaint of this patient was poor esthetics and a need to improve the appearance of his teeth, identification, and control of the etiological factors are far more important than restoring the dentition [1]. Patient compliance to stop the damaging habits was essential for the success of treatment.
The role of acetic acid on glucose and lipid metabolism has been investigated but remains unclear [17-21]. Vinegar may delay gastric emptying by acid sensors in the intestine resulting in lower post-prandial blood glucose levelsor by an effect on hepatic endogenous glucose production. Rats given acetic acid had reduced total serum cholesterol and triglyceride despite a cholesterol-rich diet [22]. The patient was informed that vinegar is acetic acid and that both citric and phosphoric acids were present in cola drinks. He was unaware that acids caused dental erosion.The patient was also advised to see a gastroenterologist regarding the GORD.
The dental treatment recommended by the authors was a direct composite restoration in line with the European consensus on management of severe tooth wear [7]. Direct composite has been proposed to be a minimally invasive, reversible, and additive restorative option, hence reducing the biological cost [10]. Moreover, the patient chose direct composite buildups as he was concerned about the high laboratory cost of ceramic crowns and wanted to keep treatment as simple as possible. The application of IPS Empress Direct (Ivoclar Vivadent, Schaan, Liechtenstein) was deemed appropriate as the clinical performance of direct hybrid composite in wear cases was good, and only 6.9% failed over a mean observation period of 3.98 years [23]. Thus, it was concluded that direct hybrid composite restoration at an increased occlusal vertical dimension is a viable treatment option [23]. Furthermore, others reported thatthe failure rate of direct composite restorations was 5.4% and concluded that bruxism and an increase in the occlusal vertical dimension were not associated with failure [24]. Treatment strategies were described according to the extent of loss of vertical dimension as either <0.5mm, <2mm, >2mm or >4mm [25]. For the most severe loss of vertical dimension, direct adhesive methods were advocated [25]. Direct composite restorations for tooth wear are cost-effective and a reversible treatment option supported by several studies [26-29], with only 11.6% of composites placed on worn occluding surfacesneeding re-intervention [30]. In this case report, an additive approach was performed by restoring the tooth surface loss with composite restorations atan increased vertical dimension, thus preventing the need for complex occlusal rehabilitation and minimizing the biological cost.
CONCLUSION
This case report documents the multifactorial nature of tooth wear with several risk factors. Careful history taking is essential in order to identify all the risk factors, followed by a clear and unambiguous explanation of the damaging conditions and/or habits that exist. A change in lifestyle with cessation of habits or erosive diet is preferable prior to restoration, but this cannot always be achieved. In some cases, restoration and improvement in appearance will motivate the patient to cease. The management of generalized severe tooth wear by a conservative approachwas novel in Dubai,as conventional crowning is prevalent. The patient was delighted with the improved aesthetics and function and appreciated the relatively low financial cost.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was evaluated and approved by the Research and Ethics Committee of the Faculty of Dentistry of Pontificia Universidad Javeriana in Bogotá, Colombia (approval # 005/2009).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent form was signed by all patients.
STANDARDS FOR REPORTING
CARE guidelines and methodology were followed.
FUNDING
This project was funded by Pontificia Universidad Javeriana. Call Support for research projects to strengthen research groups ppta # 00004687 - the project # 004480 and Clinical Laboratory and the Department of Radiology (Dr. Luis Felipe Uriza and Dr. Carlos Andrés Corredor) of the Hospital Universitario San Ignacio.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The data are at the custody of the Pontificia Universidad Javeriana (Faculty of Dentistry and Faculty of Medicine) because of the privacy and ethical restrictions.

