All published articles of this journal are available on ScienceDirect.

Telemedicine for a Multidisciplinary Assessment of Orofacial Pain in a Patient Affected by Eagle’s Syndrome: A Clinical Case Report
Authors Info & Affiliations
Abstract
Background:
Orofacial pain has a broad range of origins and a multidisciplinary approach occupies a relevant role.
Objective:
The aim of this study was to review the literature regarding the evolution of telemedicine and orofacial pain related to a case report of a patient affected by Eagle's syndrome.
Materials and Methods:
Two authors (RJM and SG) independently reviewed the literature up to March 2020. A case report was developed by including the interdisciplinary assessment and initial treatment of orofacial pain in a 38-year-old female patient affected by Eagle’s syndrome. The patient was interviewed by two different specialists (from Rome, Italy and Los Angeles, California) through an online meeting platform in order to evaluate her complex situation, demonstrating the possibilities that telemedicine offered during the COVID-19 pandemic.
Conclusion:
An interdisciplinary approach can be performed for future follow ups on patients as various advantages were found by the patient and by the clinicians themselves.
1. INTRODUCTION
Orofacial pain may be defined as pain localized in the soft and hard tissues of the head, including the face, neck, oral cavity and temporomandibular joints [1, 2].
The etiology of facial pain can be multifactorial [1]. In fact, it has a broad range of etiologies: dental, non-dental, intraoral, facial pain with/without intraoral pain and headache related facial pain [2, 3].
Intraoral pain with a non-odontogenic cause can possibly be associated with trigeminal neuropathic pain or soft tissue pathologies [2]. Facial pain with or without intraoral involvement can be related to temporomandibular dysfunction [4, 5], Trigeminal Neuralgia (TN) [6, 7], Eagle’s syndrome [8], headache-related facial pain and migraine (including neurovascular orofacial pain) [2].
Facial pain requires a multidisciplinary approach that, unfortunately, cannot always be achieved due to the difficulty in finding a facility where all specialists are present and work in teams. Dealing with such a complex disease is difficult. Being able to use a digital platform that allows clinicians to assess a patient in the presence of different specialists is certainly very important and facilitates the diagnosis and the therapeutic approach.
Despite the great potential of telemedicine, before the COVID-19 pandemic, these communication networks remained at an early adoption stage. The use of telemedicine was infrequent compared to face-to-face visits [9, 10]. The pandemic caused by the coronavirus SARS-CoV-2, which spreads via droplets and has a 1%–2% estimated mortality rate, presented an urgent need for an expansion in the use of telemedicine to minimize the risk of disease transmission [10].
The aim of this study was two-fold: 1) to review the evolution of telemedicine, specifically before and during the COVID-19 pandemic and 2) to review the current literature on orofacial pain, especially related to Eagle’s syndrome. To tie both topics together, exploring the advantages of telemedicine for a multidisciplinary approach to pain management, we reported the case of an online assessment and treatment session of a patient affected by Eagle’s syndrome.
For this reason, and for a facilitated multidisciplinary approach, we used telemedicine through the platform Zoom© Meetings with two different specialists for the assessment of a 38-year-old female patient suffering from craniofacial pain for the last four years, possibly related to Eagle’s syndrome.
2. MATERIALS AND METHODS
Two authors [RJM and SG] independently reviewed the literature up to March 2020.
Initially the project was supposed to be a systematic review but after meeting the patient who was part of the study, the project became a literature review in order to find out how telemedicine could be used to help this particular patient. The present search was limited to English articles.
The articles were divided into relevant and non-relevant according to the following inclusion criteria: 1) studies that analyzed telemedicine before and during COVID-19. 2) Studies focused on orofacial pain to analyze the symptoms of the case report of the patient presented in this article. Studies that analyzed orofacial pain not related to the symptoms of our patient were excluded from this research.
2.1. Telemedicine
2.1.1. The Evolution of Telemedicine as a Tool for a Multidisciplinary Approach
According to the World Health Organization (WHO), we refer to telemedicine as “the delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for the diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities”. [11] Telehealth is a term that is often used to encompass a broader application of technologies for distance education, consumer outreach, and other applications wherein electronic communications and information technologies are used to support healthcare services [11, 12]. The role of telecommunications in medical care has been around at least since the American Civil War (1861-1865) when the telegraph was used to transmit casualty lists and to order supplies [12]. Currently, telemedicine can be delivered via live Interactive Audiovisual (AV) links, by live streaming video, and by viewing stored educational material, while tele-consultation involves establishing a communication link between doctors who request consultations on patients under their care and experts located in distant medical centers or when there is an impossibility of reaching the doctor’s clinic [12, 13]. Privacy is maintained through point-to-point encryption between the devices involved in the interaction. In fact, virtual private network tunnels are a common method used to facilitate the privacy of the Internet connection used in telemedicine [12]. These evolving technologies also allow patients to receive care remotely even if they are homebound, live in rural or underserved areas, face other impediments that limit their access to care, have rare medical disorders requiring care from distant specialists [13]. In this regard, telemedicine facilitates multidisciplinary assessments performed by several clinicians on many platforms [14]. This is not a new concept in the field of radiology [15] nor in remote robotic surgery, and with new technology and dedicated broadband, these options are going to become even more widespread in health care. In fact, the US Department of Health and Human Services estimates that more than 60% of all health care institutions and 40% to 50% of all hospitals in the United States currently use some form of telehealth [16]. The costs of telemedicine programs vary substantially, depending on the type of interventions used, the hardware at both the originating and distant sites, along with annual depreciation, the software and its updates, information technology support, administration costs, training, licensing fees, equipment and staffing costs and the time available to provide the services of both originating and distant site providers [12, 17]. Although the economic impact of telemedicine is a collaborative and complex process in which different economic, social, and political factors can be involved, most research studies in the literature have concluded that it is still cost-effective. However, among the main limitations of the economic evaluations of telemedicine systems are the lack of randomized control trials, small sample sizes, and the absence of quality data and appropriate measures [17]. Based on a cross-sectional patient satisfaction survey made by Polinski et al. 2016, patients reported high satisfaction with their telehealth experience. Convenience and perceived quality of care were important to patients, suggesting that this modality may facilitate access to care [18]. The impact of telemedicine on everyday practice is significant and must not be neglected since this new form of medical care is continuously evolving. The results of this project strongly depend on the acceptance of the application and of the tele-medicine services too, as well as the training of personnel on how to use the system [19]. Whenever possible, previous written patient’s agreement and consent forms can be employed to use several non-public video communication tools, many of which are free or low cost, including Apple FaceTime©, Facebook Messenger© video chat, Google Hangouts© video, Zoom© and Skype©. If needed, such consent forms can be updated to include the possible use of telehealth. Patients will need access to a smartphone, tablet, or a computer with audio and a camera as well as a data plan or Internet connection [14]. Computer literacy and ease of use of all these platforms may be an obstacle for some patients for which this option may not be available [10].
| Authors | Field | Objective |
|---|---|---|
| Rao SS et al. | Orthopedic COVID-19 | To highlight the effective use of telemedicine, focused on patient education. |
| Chaet D et al. | AMA CEJA |
To provide broad guidance for ethical conduct relating to key issues in telehealth/telemedicine. |
| Burke BL Jr et al. | Pediatric | To chronicle the use of telemedicine by pediatricians and surgical specialists to deliver inpatient and outpatient care. |
| Combi C. et al. | Developing countries | To define a specific taxonomy that allows a proper classification and a fast overview of telemedicine projects in developing countries. |
| Polinski J.M. et al. | General medical care | To assess patients’ satisfaction with telehealth visits. |
| Tuckson R. et al. | General medical care | To present policy-relevant trends in telehealth adoption and to assist physicians and other health care professionals, identifying key priorities for telehealth research. |
| De la Torre-Díez I et al. | Economic | To review the cost-utility and cost-effectiveness research works of telemedicine, electronic health, and mobile health systems in the literature. |
| Calton B. et al. | COVID-19 | To develop some telemedicine quick tips based on our collective experience at UCSF and Resolution Care Network. |
| Moazzami B. et al. | COVID-19 | To underline the immediate action required for maintaining healthcare providers' well-being. |
| Smith AC. et al. | COVID-19 | To highlight the role of telehealth for global emergencies. |
| Saccomanno et al. | COVID-19 Orthodontics |
To explain how tele-orthodontics represents the only way to perform orthodontics during a period of restriction. |
2.1.2. Telemedicine: An Interdisciplinary Approach During COVID-19
The first case of COVID-19 was identified in Wuhan, Hubei province, China, at the end of 2019. The number of new cases out of China rose rapidly day-after-day. On March 11th 2020, the WHO Emergency Committee declared COVID-19 a global pandemic, affecting all countries on the globe [20]. A month later, indeed, the pandemic was affecting millions of people on every continent. With this emergency condition, telemedicine was catapulted into the role of a critically essential service for patients to help mitigate the spread of this coronavirus disease and preserve valuable personal protective equipment. During crises, when healthcare access is limited and mobility is impaired, telemedicine allows providers to continue delivering quality patient care while avoiding unnecessary risks to themselves, the care team, and their patients [10, 20]. In response to the COVID-19 pandemic, many practices have implemented telemedicine to avoid in-person contact between providers and patients [10, 21].
This virtual platform can be used by smartphones or webcam-enabled computers and allows physicians to effectively screen patients with early signs of COVID-19 before they reach the hospital [20].
The COVID-19 pandemic is not a first and nor will it be the last. For patients, telehealth can help with remote assessment (triage) and the provision of care [22].
Nevertheless, a multidisciplinary assessment by various specialists through telemedicine during this emergency was poorly reviewed, this is one of the main reasons attributed to the originality of this article. A summary of the articles analyzed in this review is provided (Table 1).
2.1.3. Case Report: Orofacial Pain Assessment in a Patient Affected by Eagle’s Syndrome
2.1.3.1. Paresthesia Post-Extraction
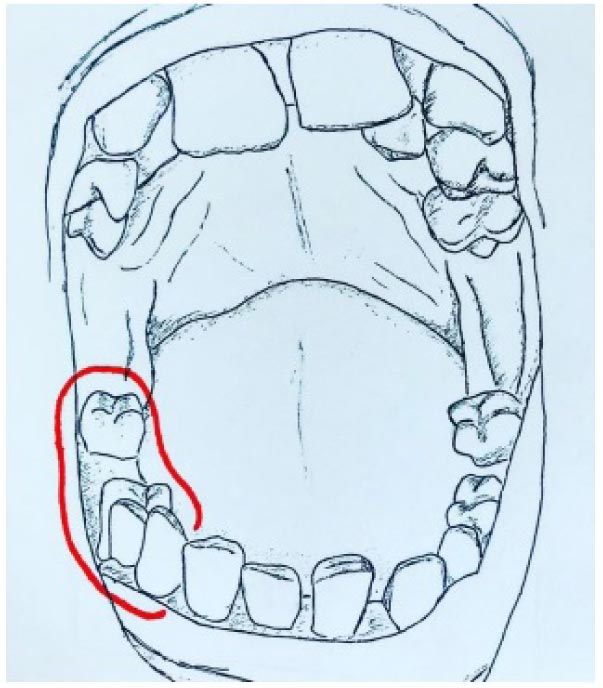
Just before the COVID-19 lockdown in Italy, a 38-year-old woman came in for a consultation and treatment for complex orofacial pain. Following a complicated extraction of the lower right first molar in 2017, she reported persisting paresthesia to the skin of her cheek, the side of the tongue, mandibular and a palatal region. An illustration of the patient’s mouth was done in order to visually represent the dental situation and the site of paresthesia indicated by the patient in a picture that she sent to the clinicians (Fig. 1).
Paresthesia can be defined as an altered sensation of numbness, burning, or prickling that may reflect an alteration in the sensation of pain in the distribution of a specific sensory nerve [23]. Mandibular paresthesia can be an unfortunate complication following the extraction of mandibular molars. The damage to the inferior alveolar nerve may occur through a direct or indirect injury during the surgical procedure or during anesthesia. Careful preoperative evaluation with radiographs is important to study the anatomical characteristics of the tooth and its relation to the mandibular canal. The knowledge of the proper anesthetic procedure and anatomical references is essential to avoid injuries to the nerve and structures in that area. When paresthesia occurs, a simple yet thorough mechanism for its documentation is required [24]. The best treatment for a nerve injury continues to be prevention; a CT scan prior to extraction therapy is the gold standard of care. Aggressively debriding granulation/cystic tissue after a tooth extraction is relevant for the removal of bacteria, inducing angiogenesis and the promotion of proper blood clotting [25, 26].
2.1.3.2. Orofacial Pain in the Contralateral Side
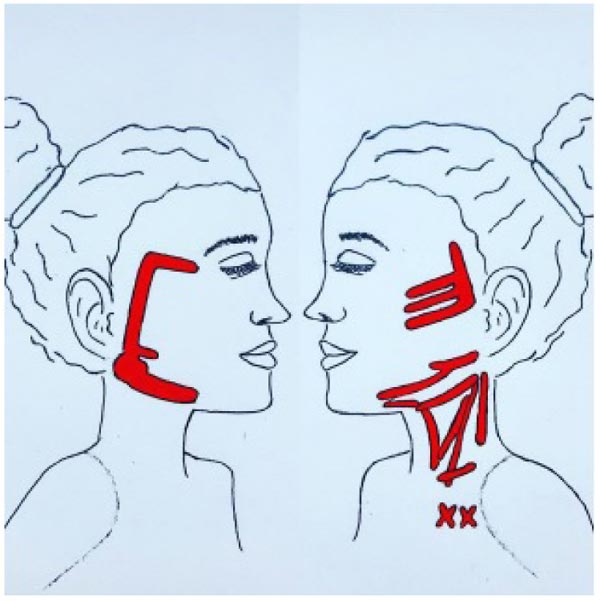
In the months following the extraction, the patient reported a sensation of a knot in the throat, pain in the left ear, strong spasmodic headaches, and muscle stiffness with a neuralgic sensation that extends to the face and neck on the left side. This chronic and disabling symptomatology caused her to withdraw from work and social life. The patient sent in pictures of the pain pattern she traced with lipstick on her face and neck. An illustration of the patient’s pain pattern is provided in Fig. (2).
The patient, due to her syndromic condition, developed several compensatory and non-physiological movements in an attempt to minimize the paresthesia or recover sensitivity but caused, over time, an overload of the muscles on the contralateral side. Following paresthesia, the body initiates a compensatory stimulation process and tries to regain normal sensory-motor function, which causes overloading of the contralateral muscles. This overload, over time, becomes chronic pain and dysfunction with reported emotional and social repercussions. The fact that the patient, additionally, has an unbalanced occlusion further worsens muscular activity, her symptomatology and her quality of life. To try to re-balance this system the patient was instructed to be aware and inhibit those spurious movements with her mandible, cheeks and tongue. At the same time, she was instructed to stimulate a neuroplastic mechanism with correct movements and application of selected tactile stimuli to recuperate the local sensitivity as much as possible [27].
Furthermore, chronic pain is also associated with the parasympathetic action of the vagus nerve [28]. Patients suffering from chronic painful events have a decrease in the vagal tone that is associated with heart rate variability, dizziness [29], an imbalance of the autonomic nervous system, neuropathic, neurovascular or idiopathic cause [30-32].
Orofacial pain is usually intended as pain within the trigeminal system. The trigeminal nerve supplies general sensory innervation-touch, pressure, temperature, pain and other sensations to face, scalp, and mouth. The trigeminal sensory region is very complex, incorporating the cranium, ears, eyes, sinuses, nose, pharynx, infratemporal fossa, jaw joint, teeth, jaws, salivary glands, oral mucosa, and skin [30]. The International Association for the Study of Pain (IASP) defines trigeminal neuralgia as “a sudden, usually unilateral, severe, brief, stabbing, recurrent pain in the distribution of one or more branches of the fifth cranial nerve”. [31, 33] Also, according to the IASP, neuropathic pain is initiated or caused by a primary lesion or nervous system dysfunction [34]. In a minority of cases, trigeminal neuralgia is secondary to benign or malignant tumors [31].
Continuous Neuropathic Orofacial Pain is a little-known condition among the general population, physicians and dentists. This contributes to a late diagnosis and inaccurate treatments that often involve unnecessary suffering. It is important to inform both the general population and health professionals concerning this painful condition [30, 31].
Trigeminal Neuralgia (TN) is characterized by touch-evoked unilateral brief shock-like paroxysmal pain in one or more divisions of the trigeminal nerve [6]. TN is divided into classical TN (CTN) and secondary TN (STN).
The pain results from specific abnormalities of trigeminal afferent neurons in the trigeminal root or ganglion. Injury renders axons and axotomized somata hyperexcitable. The hyperexcitable afferents will give rise to pain paroxysms as a result of synchronized activity after discharge [7]. Demyelination of primary sensory trigeminal afferents in the root entry zone is the predominant pathophysiological mechanism.
In addition to paroxysmal pain, some patients also have continuous pain [6].
However, there are also other unknown etiological factors, as only half of the CTN patients have morphological changes. Multiple sclerosis or a space-occupying lesion affecting the trigeminal nerve is seen instead to cause STN [6, 7].
2.1.3.3. Visits to Several Otorhinolaryngologists (ENTs)
Following several visits with various specialists, the patient we observed was diagnosed with tonsillar hypertrophy. Adenotonsillar hypertrophy is one of the most common etiologies of Obstructive Airway Disease (OAD), which is caused by excessive lymphoid tissue proliferation in tonsils [35]. This proliferation might lead to an obstruction of the airways, especially to a nasal airway obstruction due to adenoid hypertrophy, which results not only in dentofacial growth anomaly in young ages but also in obstructive sleep apnea and its devastating consequences [36, 37]. The main surgical process of relieving this obstruction is adenotonsillectomy, which involves tonsils being cauterized, curetted, lasered, or otherwise ablated [37]. Thus, the patient’s tonsils were removed with a tonsillectomy without getting the desired results, since her chief complaint was orofacial pain. Since the otorhinolaryngologists who performed the AT surgery suspected a possible lymphoma, a biopsy of the adenoidal tissue was made, with negative results.
Meanwhile, other tests were performed all with negative results: Hematological panel, laryngoscopy, and Positron Emission Tomography (PET).
Other treatments were proposed to the patient to try to reduce her pain but without results: antidepressants and medication for neural pain; physical therapy (made the pain worse); and dental prosthesis.
A polysomnographic evaluation of the patient was done just before this evaluation, but the details of the results were not yet available at the time of this writing.
2.1.3.4. Diagnosis of Eagle’s Syndrome
Four years after the traumatic dental extraction, our patient was diagnosed with Eagle's syndrome, presuming that this was the cause of her discomfort. A facial and neck MRI without contrast was performed, leading to the diagnosis of the syndrome. According to the report, on the right side, in intercuspation, the mandibular condyle is centered in the glenoid fossa. At the maximum opening, an anterior translation of the condyle is observed, which goes beyond the apex of the temporal eminence. On the left side, when the patient closes the mouth, the mandibular condyle is normally centered in the glenoid fossa. The auricular meniscus is minimally posteriorly placed. In the maximum opening, there is the anterior translation of the condyle.
Eagle's syndrome is characterized by cervicopharyngeal signs and symptoms associated with the morphological ossification or elongation of the styloid apophysis. This elongation may occur through ossification of the stylohyoid ligament or through the growth of the apophysis due to osteogenesis triggered by a traumatic factor. Reaching a precise diagnosis of the syndrome is difficult and a good medical and radiological assessment must be made because it can be easily confused with other neuralgic facial pain syndromes or non-specific facial pain. Finger palpation of the palatine tonsil increases the pain associated with Eagle's syndrome and helps to confirm the diagnosis.
The elongation of the styloid apophysis or the calcification of the stylohyoid ligament may give rise to intense facial pain, headache, dysphagia or odynophagia, otalgia, buzzing sensations, and trismus [8].
This elongation and calcification may influence the surrounding structures and cause a compression of the nerves and lymphatic and blood vessels [38, 39]. In some rare cases, the compression of the internal carotid artery has been described. It can even compress the sympathetic nerve, causing Horner syndrome [38, 40]. These different hypotheses should take into consideration the styloid process angulation, which is crucial for the surrounding anatomical relationships and excludes common and easily treated odontogenic causes of pain [30]. Some differential diagnosis of pain should include glossopharyngeal and trigeminal neuralgia, migraine, myofascial pain, temporal arteritis, cluster headaches, dysfunction syndrome, pain related to unerupted third molars, cervical arthritis and tumors [40].
2.1.3.5. Vasovagal Syncope
Not long after the online meeting, the patient reported having various moments of dizziness and tachycardia that would appear suddenly. She also reported an episode of vasovagal syncope with a feeling of fainting, drowsiness, nausea and bowel movement probably due to an intense painful episode that led to a drop in blood pressure. It is possible that her new condition of chronic generalized sensitization triggered vaso-vagal responses as well.
2.1.3.6. Lack of Occlusion, Orofacial Pain and TMD
The patient is missing various dental elements, especially on the side of the tooth extraction, and so she does not have a stable occlusion. Her second lower molar does not have a corresponding occlusion and it’s now pressing against the palatal alveolar gingiva. Having no functional occlusion on the right side of her mouth, the right masseter muscle is in dysfunction and now it’s in a constant state of soreness and pain, coupled with the overlaying skin paresthesia. This lack of occlusion contributed to the orofacial pain and overload of the temporomandibular junction. In fact, in a previous study, a non-functional tooth contact was approximately 3 to 6 times more common in patients with TMD than in the healthy subjects [41]. Temporomandibular disorders (TMDs) include musculoskeletal and neuromuscular conditions that involve the temporomandibular joints (TMJs), the masticatory muscles, and all associated tissues [4, 5, 42]. There may be associated clicking, grinding, or locking of the temporomandibular joints. The pain may be intermittent or continuous, and it is usually described as dull, aching, or throbbing, or in the words of patients: “weight on the side of the face getting heavier and heavier,” “pressure feeling,” “an elastic band that is too tight,” or “needles digging in.” [2] TMD has been linked to other psychological and chronic pain conditions, including fibromyalgia, back pain, headaches, chronic widespread pain, and hypermobility [2, 4]. Recent studies have described an association between TMD and headaches. Many patients with TMD also report a headache, and in some cases, a clear relationship between temporomandibular joint-related triggers and a headache onset can be observed. TMD is also common among patients suffering from migraine and those who suffer from a tension-type headache [2]. Headaches are frequent disorders occurring in 18% of women and 6% of men during the most productive years of the individuals affected [43].
Although parafunctional habits have been implicated in TMD, their relationship with headache remains unknown. Of all the parafunctional activities of the stomatognathic system, bruxism is assumed to be the most damaging parafunction and a major risk factor for TMDs [4].
2.1.3.7. Chief Complaints
At present, the patient reported that her chief complaint was the localized symptoms, which have become more severe with time. Thus, she was resolute in solving her orofacial pain, heavily affecting her social and working life.
Secondary complaints reported were vertigo, feeling unsteady, and otalgia.
Tertiary complaints were related to postural issues, generalized pain and fatigue/malaise, with a localized tingling sensation in one leg.
2.1.3.8. Multidisciplinary Approach through a Zoom© Meeting
In order to perform an interdisciplinary assessment, a Zoom© meeting was scheduled, which included the patient as well.
Zoom© is a software-based video conferencing tool that allows users to meet online, with or without video. It brings video conferencing, online meetings and group messaging into one easy-to-use application.
The Zoom© platform offers several tools to protect meetings from strangers joining in and to ensure privacy due to a required access code. Policies and controls to safeguard the collection, use, and disclosure of information are also present.
The team of specialists in orthodontics was based in Rome, Italy and the speech-language pathologist with competencies in myofunctional sciences and therapy was based in Los Angeles, California.
A clinician (S.S.) visited the patient in person before the pandemic period and was aware of the complexity of the case.
Standard written informed consent was obtained from the patient.
All the clinicians participating in the meetings had prior access to the medical history of the patient.
A screenshot of the meeting reporting the radiological information of the patient is shown in Fig. (3).
2.1.3.9. The Multidisciplinary Objectives for the Online Visit and Outcomes from the Meeting
- The importance of addressing the local anatomo-physiological changes due to Eagle’s syndrome was highlighted and all professionals reached a consensus that a maxillofacial surgeon should treat the localized problems due to Eagle’s syndrome.
- The importance of a multidisciplinary intervention, both pre and post maxillofacial surgery, was underlined. The aim of this phase was to eliminate parafunctions, compensatory movements and reduce the muscle overload that developed following the post-extraction paresthesia on the patient’s right side.
- The relevance of addressing the postural problem was highlighted to reduce local and general neuralgia and overall muscle overload, and a physical therapist or a fascial therapist referral was suggested, despite a past lack of results, as more general muscular decompensation is noted.
- Home assignments were given to the patient with the following goals:
- To increase awareness and control of parafunctions and excessive muscle recruitment, along with a reduction of the constant touching of the areas of paresthesia (both oral and facial), by recording daily on a scale of 1 to 10 how many times she caught herself not making or inhibiting compensatory movements or tactile stimulations.
- To reduce paresthesia and regain some sensitivity by stimulating neuroplastic local repair, the patient will stimulate the paresthetic right side areas with specific tools (cloth, spoon handle and cotton Q-tips©) and on a schedule. To monitor progress, the patient will use, as a reference, a “map” of her facial and intraoral paresthesia that she identified and sketched on a drawing.
- To control the localized swelling and pain on the left area between her neck and jaw, she will apply warm cloth compresses and record a numerical evaluation of the improvement of pain (on a scale between 1-5, 1 being no pain and 5 being very painful).
- To continue motivating the patient, to monitor the improvement of her symptoms and to help her prepare for the future steps in treatment, she will receive weekly follow-ups.
- As soon as possible, dental solutions to restore the patient’s occlusion will be implemented, as a lack of occlusion on the right side is weakening the masseter muscle and causing significant tooth movement, contributing to constant pain and discomfort.
3. DISCUSSION
The current coronavirus (COVID-19) pandemic is reminding us of the importance of using telehealth and telemedicine to deliver care, especially as a means of reducing the risk of cross-contamination caused by close contacts [44]. Although this method was already established, an increased use was reported during the COVID-19 emergency months because multiple clinicians can participate in the same videoconference to assess a single patient, resulting in a more efficient assessment of the various needs and comorbidities of the patient.
The patient’s medical history can be collected during the online meeting [2, 45]. A detailed pain history is crucial in order to rule out causes other than dental reasons for facial pain before invasive dental therapy may be considered [46]. Therefore, a multidisciplinary approach and additional imaging modalities might be necessary to find the optimal treatment for the patient [2, 45].
For the complex case of the patient reported in this article, telemedicine represented an optimal option to obtain an interdisciplinary assessment, also given the unusual circumstances. The intense facial pain, which is a characteristic of Eagle’s syndrome [8], and the additional issues that arise, need to be evaluated by different experts, but often the consultations are serial, without much exchange of information between specialists, skewing the process in favor of more testing and less in favor of treatment and long term stability.
Therefore, during the online meeting, some strategies and exercises were proposed to the patient to do before and after any possible maxillofacial surgery to improve her situation and, consequently, her quality of life.
Education, psychological support and self-management strategies are recommended as part of a multidisciplinary approach to the management of orofacial pain. At the end of a lengthy chain of evaluations by different specialists, the importance of a team approach cannot be underestimated. After having undergone operations such as a tonsillectomy without any results, the patient noted the need to be listened to and understood by doctors and not be abandoned or treated as if “it is all in your head”. The patient was prescribed antidepressants and medication for neural pain to deal with the pain itself, which unfortunately did not help the pain caused by paresthesia and did not help with the pain caused by Eagle’s syndrome, since the cause was not yet diagnosed. By following this medication regimen, the patient suffered from significant side effects for a year and a half without benefiting from the treatment that was then discontinued. The patient further stated that all those consultations left her feeling she was wasting money and time without solving the problem. However, it is important to reframe the situation in the eyes of the patient, as finding the cause of a problem is a process with cumulative learning along the way. Having gone through various evaluations and specialists was not a waste of time or money just because the results were negative, because possible case scenarios were eliminated, thus narrowing the field of search.
This online meeting was carried out during a pandemic period. Nevertheless, this multidisciplinary approach method can be performed in the future on the same patient or on other complex cases that require multiple specialists’ evaluation in a team approach as compared to a serial approach. In fact, various practical and emotional advantages were found by the patient and by the clinicians themselves. To meet online as a team, from the comfort of her home, having the time and means to explain her situation and receiving a workable plan of treatment was a novel but a welcome solution for that patient. The clinicians were able to pinpoint diagnostic elements or propose a therapeutic solution that are familiar to them by reason of their own professional and academic background and not necessarily known by other professionals.
The patient was satisfied with this telehealth meeting, although it was the very beginning of a treatment plan, so the actual results of reducing her chief complaints will be pending over time. Moreover, the results from one case report may not produce a similar change in another patient. Thus, the results cannot be generalized, and surely more studies, with additional specialists, should be conducted on the interdisciplinary approach of telemedicine to approach orofacial pain.
CONCLUSION
Related to the first aim of this study, a revision of the evolution of telemedicine was done before and after the onset of the COVID-19 pandemic revealing an increased use of telemedicine was appreciated during the first six months of the pandemic period. Regarding the second aim, an assessment and treatment plan related to the orofacial pain symptoms of the patient affected by Eagle’s syndrome was performed remotely and mostly online. In fact, in complex pathologies such as orofacial pain, where the causes can be multiple, a telemedicine approach can be used and useful, as the same results are difficult to achieve with the classic serial model in which one specialist at a time visits the patient in person. Clearly, telehealth has limitations in its use: many consultations require physical examinations that may be difficult to perform remotely (e.g., auscultation) and diagnostic tools (e.g., imaging, cultures), which cannot be done remotely. The clinicians should highlight the limitations of telehealth and inform the patient about alternative methods of information gathering [22, 44]. On the other hand, the positive aspect is that various specialists can interact through network platforms like Zoom© and work as a team. The specialists can meet in a friendly and constructive atmosphere, and everybody has a stake in trying to find a solution to improve the patient's quality of life.
CONSENT FOR PUBLICATION
All the participants have given informed consent to participate in this study.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors thank Giulia Giancaspro, a graduate in Business Administration and Management at Bocconi University (Milan, Italy) and student of the postgraduate Master of ESCP Business School (Paris, France), for the realization of the illustrations of this article.

