All published articles of this journal are available on ScienceDirect.

COVID-19 and Infection Control in Dental Clinics; Assessment of Public Knowledge, Attitudes and Practices in Several Regions of Saudi Arabia
Abstract
Background:
The recent outbreak of the Corona Virus Disease (COVID-19) has affected millions of lives in different countries including the Kingdom of Saudi Arabia. Due to the characteristics of dental practice settings, there is a high risk of infection transmission between patients and dentists.
Objectives:
The aim of this study was to assess the level of public knowledge, attitude and practice regarding COVID-19 and infection control when visiting a dentist.
Methods:
In April 2020, a web-based cross-sectional survey was distributed randomly among the public through social media platforms. A validated anonymous questionnaire was used to assess knowledge about COVID-19 and participants’ attitudes toward extra measures to prevent the spread of infection.
Results:
Among the completed questionnaires (N=521), the mean age of the participants was 36.24 years, 68.3% were women, 87.5% held a university degree, and 81% were from the Makkah region. Most of the participants (99%) obtained a good knowledge score regarding COVID-19. Women were more likely than men to have more knowledge (p<0.05). Nearly all of the participants (99.6%) demonstrated good attitudes towards precautionary measures in dental clinics.
Spearman’s rho test showed a statistically significant correlation between age and attitude score, suggesting that attitude score increased with age (p<0.05). Overall, 73.3% reported that they would maintain good hygiene practices when visiting a dentist during this pandemic.
Conclusion:
Most Saudi residents with a high education level are knowledgeable about COVID-19, hold promising attitudes, and have appropriate practices towards precautionary measures needed while visiting a dental clinic during the virus outbreak.
1. INTRODUCTION
In January 2020, the Chinese Center for Disease Control and Prevention announced the emergence of a novel coronavirus (COVID-19) in Wuhan, China [1]. The resulting COVID-19 pandemic has become a global public health crisis, with 15,296, 926 cases and 628,903 deaths worldwide [2]. As of 24 July 2020, the Kingdom of Saudi Arabia reported the second largest number of cases in the Eastern Mediterranean region, where over 260,394 cases were reported, with a recovery rate of 81.9% and around 1% mortality rate [2, 3].
COVID-19 is an acute respiratory syndrome which can cause fever, dry cough, shortness of breath, fatigue, and other atypical symptoms such as muscle pain and headache [4]. It spreads more rapidly than the Severe Acute Respiratory Syndrome (SARS), and the rates of human-to-human transmission were generally higher when compared with the Middle East Respiratory Syndrome (MERS) [5]. Researchers suggest that transmission occurs between individuals via airborne droplets and contact with an infected person or contaminated surface [5, 6].
Given the nature of dental practice, there is a high risk of infection transmission between patients and dental practitioners due to the formation of a large number of droplets and aerosols during treatment [7]. The standard protective measures in daily clinical work are not sufficient to prevent the spread of COVID-19, therefore, strict and urgent infection control protocols are needed [7]. For example, the World Health Organization (WHO) recommends that dental clinics institute routine pre-appointment triaging, temperature measurement, detailed health status investigation, and checking of COVID-19 risk factors including recent travel and contact with an infected person [8]. Elective dental treatments should be deferred for at least 2-3 weeks for patients who present with fever and/or respiratory symptoms. However, when dental treatment is needed, dentists are required to follow more strict guidelines on infection prevention and control when dealing with suspected or confirmed cases of COVID-19. It is currently recommended that dentists use disposable hand instruments, frequently disinfect surfaces with chemicals approved for COVID-19, and minimize or avoid procedures that produce droplets [7]. Moreover, they should wear protective equipment including face shields, gowns, and N95 masks [7]. A previous study has issued specific guidelines and recommendations to deal with infectious diseases, such as the use of low or high volume saliva ejectors, which can reduce the production of droplets and aerosols [9]. With the increasing demand for dental care among individuals, patients should be aware of extra precautions to minimize the spread of infection. Patients should wear a surgical mask, cover their mouth and nose, and perform frequent hand hygiene [10].
As there is no current treatment, prevention and increasing awareness of extra precautions during this pandemic outbreak of COVID-19 are essential for protecting people. Efforts have been undertaken by the Saudi government through massive media campaigns to increase the level of awareness of the disease and public adherence to preventive measures to control the spread of the disease. Hence, it is expected that the Saudi population gained awareness and knowledge about the disease and its mode of prevention and transmission.
Most of the available studies into knowledge of infection control have investigated dentists and dental students, rather than patients [11, 12]. Therefore, to address this knowledge gap, this study aimed to assess the level of Knowledge, Attitude and Practice (KAP) of the public about COVID-19 and extra precautions needed when attending dental clinics during the outbreak in Saudi Arabia.
2. MATERIALS AND METHODS
2.1. Study Design
During April 2020, we conducted a descriptive cross-sectional survey among adult individuals in different regions of Saudi Arabia. We included individuals who fit the age group (over 18 years old), men or women, of any educational level. We excluded healthcare staff or students, and anyone who refused to participate. The sample size was calculated using OpenEpi online sample size calculator, using an estimated prevalence of 50%, a precision level of 5%, and a confidence interval of 90%, we identified that the minimum number of participants needed for this study was 271. The study was approved by the Faculty of Dentistry Institutional Review Board, Umm Al-Qura University (IRB number 172-2020).
An online survey was created using SurveyMonkey and sent randomly to the public through social media platforms. Due to current official restrictions, the questionnaire was promoted mainly via Facebook, WhatsApp, and Twitter messages by the author, with recipients being asked to share the survey with their connections. All participants gave written informed consent, and participation was voluntary and anonymous. It took approximately 5 minutes to complete the questionnaire. The questionnaire was prepared in Arabic and English formats to correspond with the reading and compre- hension levels of participants with different levels of education.
2.2. Questionnaire
A 20-item questionnaire was developed according to guidelines proposed by the Centers for Disease Control and Prevention (CDC) and WHO [8, 13]. It was based on questionnaire used in a previous study [14], and was divided into four parts. The first part explored the sociodemographic characteristics of the participants. The second part assessed participants’ knowledge regarding COVID-19. It consisted of 9 multiple-choice questions, for each of which a score of 1 was given for the correct answer and 0 for the incorrect or unknown answers. A total knowledge score was calculated, ranging from 0 to 9. Knowledge was classified into three groups according to the total score of each respondent; poor (0-3), moderate (4-6), and high (7-9).
The third part measured participants’ attitudes and opini- ons toward extra measures required to prevent COVID19. This part consisted of 10 statements with which participants indicated their level of agreement using a 3-point Likert scale (a score of 1 being disagreement and 3 being agreement), giving each participant a total score of between 10 and 30 for this section. The fourth part included questions to gauge participants' practice of hypothetical situations, such as accepting dental treatment from a dentist who is not wearing a mask or gloves. It involved 10 yes/no questions. The minimum score was 0, and the maximum was 1, of which a score of 5 and less considered poor practice and score of 6 and more considered as good practice.
The explanatory (independent) variables were the participants’ gender, nationality, region, level of education and working status. The dependent variables of interest were the questions related to the respondents’ knowledge, attitude and practice.
Initially, we consulted two experts to ensure the content and face validity of the questionnaire, one from the Preventive Dentistry Department of Umm Al-Qura University, who had clear understanding of infection control and the COVID-19 guidelines for healthcare workers; and the other with an expertise in questionnaire development. They evaluated the items of the questionnaire for clarity, importance, and relevance. Based on the experts’ feedback, minor changes were made in word choices and sentence structure. The developed questionnaire was then pilot tested on a convenient sample of 25 participants to evaluate the format and sequence of the questions. Participants were encouraged to share their thoughts about the items with the researcher and provide feedback about the content and clarity of the draft questionnaire. The questionnaire was then reviewed, and minor modifications were made (e.g., clarifying the questions). Test-retest reliability was determined where participants completed the questionnaire twice within a one-week interval and Cronbach’s alpha was 0.78.
2.3. Statistical Analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS Version 22.0, Chicago, IL, USA). Descriptive analysis, including frequency (percent) and mean (standard deviation), was performed to present an overview of the findings. Fisher’s exact test was conducted to determine the associations between knowledge and practice scores by demographic. Mann-Whitney U test was used to compare the attitude scores by demographic. Spearman correlation was used to determine the correlation between knowledge, attitude, and practice scores with age. All p-values ≤ 0.05 were considered statistically significant.
3. RESULTS
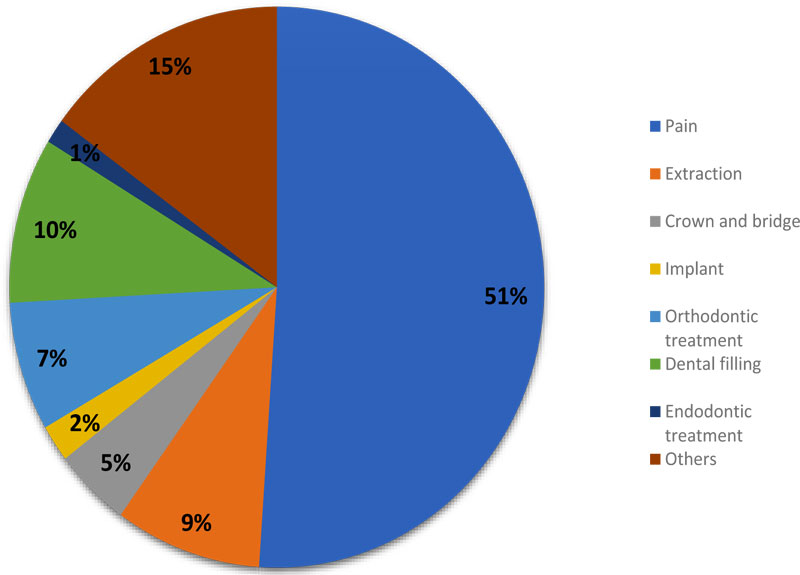
Of the total 521 participants, the majority were women (68.3%, n=356), Saudi nationals (91.0%, n=474), residents from Makkah region (81.0%, n=422), University level of education (87.5%, n=456), and employed (57.6%, n=300) (Table 1). The mean ± SD age of the participants was 36.24 ± 11.41 years, ranging from 18-83 years. Most of the participants reported correct responses to knowledge statements, as shown in Table 2. Notably, 46.8% (n=244) and 49.1% (n=256) reported that COVID-19 is dangerous, and very dangerous, respectively. Most of the participants reported the website of the Ministry of Health (35.7%), followed by social media (27.6%) and TV (19.5%) as their preferred sources of information about COVID-19. Only 8.8% (n=46) reported that they had visited the dentist during the COVID-19 outbreak. Fig. (1) presents the reasons for visiting a dentist.
| - | Mean | SD | |
| Age | - | 36.24 | 11.41 |
| - | n | % | |
| Gender | Male | 165 | 31.7 |
| Female | 356 | 68.3 | |
| Nationality | Saudi | 474 | 91.0 |
| Non-Saudi | 47 | 9.0 | |
| Region | Makkah | 422 | 81.0 |
| Riyadh | 56 | 10.7 | |
| Madinah | 13 | 2.5 | |
| Western region | 23 | 4.4 | |
| Asir | 7 | 1.3 | |
| Level of education | Elementary | 3 | .6 |
| Intermediate | 9 | 1.7 | |
| High school | 53 | 10.2 | |
| University | 456 | 87.5 | |
| Working status | Working | 300 | 57.6 |
| Not working | 221 | 42.4 | |
| - | n | % | |
| What are the symptoms of corona virus COVID-19? | Fever* | 507 | 23.2 |
| Cough* | 447 | 20.5 | |
| Difficulty breathing* | 501 | 23.0 | |
| Fatigue* | 349 | 16.0 | |
| Headache* | 346 | 15.9 | |
| Skin rash | 32 | 1.5 | |
| Who are at higher risk of having COVID-19? | Children | 164 | 15.0 |
| Elderly* | 459 | 41.9 | |
| People with chronic disease* | 463 | 42.2 | |
| I don’t know | 10 | 0.9 | |
| The incubation period of COVID-19 is | 2-7 days | 11 | 2.1 |
| - | 7-14 days* | 452 | 86.8 |
| - | More than 14 days | 53 | 10.2 |
| - | I don’t know | 5 | 1.0 |
| How is COVID-19 transmitted? | Direct contact | 18 | 3.5 |
| - | Indirect contact | 26 | 5.0 |
| - | Both* | 475 | 91.2 |
| - | I don’t know | 2 | .4 |
| Do you think COVID-19 is: | Not dangerous | 21 | 4.0 |
| - | Dangerous* | 244 | 46.8 |
| - | Very dangerous | 256 | 49.1 |
| During COVID-19 outbreak, do you think dental clinics should measure your temperature before seeing the dentist? | Yes* | 505 | 96.9 |
| - | No | 16 | 3.1 |
| During COVID-19 outbreak, do you think dental clinics should ask you about your travelling trips during the past 14 days? | Yes* | 496 | 95.2 |
| - | No | 25 | 4.8 |
| During visiting the dental clinic, do you think you should wash your hands frequently? | Yes* | 515 | 98.8 |
| - | No | 6 | 1.2 |
| During visiting the dentist, do you think you should rinse your mouth before starting dental treatment? | Yes* | 380 | 72.9 |
| - | No | 141 | 27.1 |
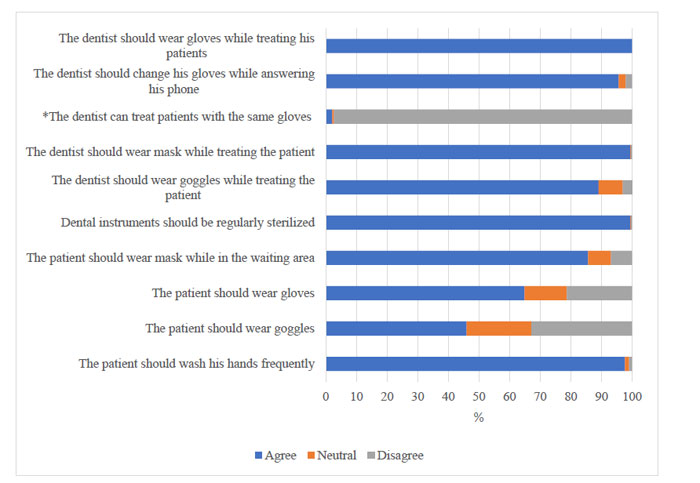
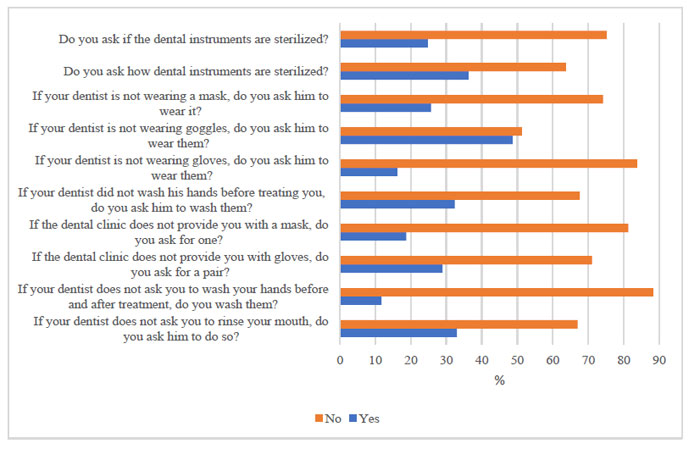
Most of the participants agreed with the statements on their visit to the dental clinic to minimize the spread of COVID-19. The majority disagreed that dentists can treat patients with the same gloves (Fig. 2). Most of the participants reported that they would observe good hygiene practices during a visit to the dentist during the COVID-19 outbreak (Fig. 3).
Fisher’s exact test showed that women were significantly more likely to have a high level of knowledge, and men were significantly more likely to have a moderate level of knowledge (p<0.05). No statistically significant association was found between knowledge and nationality, region, level of education, or employment status (p>0.05). None of the partici- pants had a poor level of knowledge (Table 3). Spearman’s rho test showed a negative correlation between age and knowledge level, suggesting that knowledge level decreased with an increase in age. However, this relationship was not statistically significant (p>0.05).
The Mann-Whitney U test showed no statistically significant difference in the mean ± SD attitude score by demographics (p>0.05) (Table 4). Spearman’s rho test showed a statistically significant positive correlation between age and attitude score, suggesting that attitude score increased with age (p<0.05). Fisher’s exact test showed no statistically significant association between practice score and demographics (p>0.05) (Table 5). Spearman’s rho test showed a positive correlation between age and practice, suggesting that practice score increased with age. However, this relationship was not statistically significant (p>0.05).
| - | Poor (0-3) |
Moderate (4-6) |
High (7-9) |
p value | |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Gender | Male | 0 (0.0) | 21 (12.7) | 144 (87.3) | 0.029 |
| Female | 0 (0.0) | 24 (6.7) | 332 (93.3) | ||
| Nationality | Saudi | 0 (0.0) | 44 (9.3) | 430 (90.7) | 0.107 |
| Non-Saudi | 0 (0.0) | 1 (2.1) | 46 (97.9) | ||
| Region | Makkah | 0 (0.0) | 41 (9.7) | 381 (90.3) | 0.075 |
| Others | 0 (0.0) | 4 (4.0) | 95 (96.0) | ||
| Level of education | Below University | 0 (0.0) | 8 (12.3) | 57 (87.7) | 0.244 |
| University | 0 (0.0) | 37 (8.1) | 419 (91.9) | ||
| Working status | Working | 0 (0.0) | 26 (8.7) | 274 (91.3) | 1.000 |
| Not working | 0 (0.0) | 19 (8.6) | 202 (91.4) | ||
| - | Mean | Standard Deviation | p value | |
|---|---|---|---|---|
| Gender | Male | 27.8 | 2.3 | 0.173 |
| Female | 28.1 | 1.9 | ||
| Nationality | Saudi | 28.0 | 2.1 | 0.988 |
| Non-Saudi | 28.0 | 2.0 | ||
| Region | Makkah | 28.0 | 2.1 | 0.918 |
| Others | 28.0 | 2.1 | ||
| Level of education | Below University | 28.2 | 2.2 | 0.265 |
| University | 28.0 | 2.0 | ||
| Working status | I work | 27.9 | 2.2 | 0.463 |
| I don’t work | 28.1 | 1.92 | ||
| - | Poor (0-5) |
Good (6-10) |
p valuem | |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Gender | Male | 43 (26.1) | 122 (73.9) | 0.915 |
| Female | 96 (27.0) | 260 (73.0) | ||
| Nationality | Saudi | 130 (27.4) | 344 (72.6) | 0.299 |
| Non-Saudi | 9 (19.1) | 38 (80.9) | ||
| Region | Makkah | 111 (26.3) | 311 (73.7) | 0.706 |
| Others | 28 (28.3) | 71 (71.7) | ||
| Level of education | Below University | 11 (16.9) | 54 (83.1) | 0.071 |
| University | 128 (28.1) | 328 (71.9) | ||
| Working status | I work | 81 (27.0) | 219 (73.0) | 0.920 |
| I don’t work | 58 (26.2) | 163 (73.8) | ||
4. DISCUSSION
Based on the WHO guidelines, as a routine procedure, dental clinics are required to establish a precheck triage to measure the temperature of patients and obtain their travel history in the past two weeks [8]. Dental quality control centers in different cities implemented supplementary measures into their recommendations for dental services to ensure the quality of infection control [7].
In this study, we investigated 521 Saudi residents from different regions of Saudi Arabia and the majority of the respondents were from the Makkah region. This study included participants who had access to the internet. Hence, most of the participants had a higher level of education. To the best of our knowledge, no previous study was conducted on the population residing in Saudi Arabia to assess the KAP about extra precautions required when visiting dental clinics during the COVID-19 outbreak in Saudi Arabia.
Our results indicate that 91.4% of the participants had a high level of knowledge regarding the mode of spread, signs, and symptoms of COVID-19. This finding is in agreement with other studies that showed that the Saudi population was knowledgeable about previous epidemic diseases like MERS [15]. This might be due to the characteristics of our study sample, where 87.5% had university degrees. A study investigating Chinese citizens during the period of the COVID-19 outbreak, reported that 90% of their respondents were knowledgeable about COVID-19 [16]. In the United States, approximately eight weeks after the first case was diagnosed, the average knowledge score for US residents was 9.72 out of 12 (approximately 80%) [17]. The high knowledge levels found in these studies might be due to the time when the questionnaires were distributed. During that period, people may have gained awareness about the disease from television and media to protect themselves and their families from contracting the disease. The majority of our participants gained knowledge about the disease from the Ministry of Health website, followed by social media and television.
It is worth mentioning that the massive ongoing awareness campaign raised by the Saudi Ministry of Health through their website and social media to fight the novel coronavirus might have contributed to a high level of knowledge among Saudi citizens and residents. The Ministry of Health issued a guide to COVID-19 in different languages about preventive measures to minimize the spread of the disease. These efforts made by the Saudi government to early engage the public with preventive and control measures affected their knowledge.
In this study, gender was significantly associated with knowledge level, with women obtaining a higher knowledge score than men. This finding is supported by other studies that have found that female and highly educated respondents are more knowledgeable about emerging infectious diseases [15, 18]. Additionally, this could be related to the fact that women are more likely to seek health information and be more curious about their own health than men [19, 20].
Attitudes to precautions to prevent COVID-19 in dental clinics were promising. The majority (99.6%) agreed that the dentist and patient should wear personal protective equipment, such as masks. They also agreed that frequently disinfecting the dental surfaces, along with frequent hand hygiene, will reduce the risk of infection. These preventive attitudes could be attributed to the strict prevention and control measures issued by the Ministry of Health. The measures included closure of schools and universities, suspension of all flights, and obligatory wearing masks in public places and keeping social distance. The positive attitude of the participants could be a result of the good public knowledge about the infectivity of the COVID-19 virus. In line with findings from previous studies, Saudi dental patients have positive attitudes towards dentists using barrier methods to prevent infection during dental treatment [14, 21]. Moreover, the findings revealed that a high attitude score was more common among older people. This may be because older adults are at higher risk of severe illness from COVID-19. The awareness-raising efforts by the Ministry of Health and the strict precautionary measures announced by the Saudi government have likely helped to increase a sense of responsibility and societal awareness.
With regards to self-reported practices, our findings revealed that most of the participants (73.3%) would act appropriately on their visit to the dentist during the COVID-19 outbreak. During this global crisis, the participants of the current study reported that they were more likely to refuse to receive dental treatment from a dentist who is not wearing personal protective equipment. Our result is consistent with previous studies in Saudi Arabia where the participants were aware of the importance of dentists wearing barrier methods to prevent infection during treatment [14, 21]. According to the WHO guidelines, dentists should take strict personal protection measures and avoid or minimize procedures that can produce droplets or aerosols [7, 8]. Only dental emergencies should be treated during this pandemic period, and routine dental procedures should be deferred [7]. That being said, only 8.8% of the respondents reported visiting the dental clinic during the COVID-19 outbreak, and the main reason for their visit was dental pain. The good level of knowledge of proper hygienic practices observed in our sample is re-assuring.
Due to the scarcity of available data, there is no comparable study assessing attitudes and practice among the public regarding COVID-19 in the dental clinic. Most of the recent studies investigated dentists or healthcare workers [22-24]. These studies showed that dentists have a high level of knowledge and appropriate attitudes toward treating patients with COVID-19 [22, 23]. Therefore, this study shed light on an area where limited information is available, and, to the best of our knowledge, it is the first study conducted to assess public awareness of COVID-19 while visiting dental clinics in Saudi Arabia. The aforementioned findings suggest that the ongoing intensive health-awareness campaigns by the local government and the Ministry of Health have been effective in encouraging the community to take appropriate actions to reduce the spread of COVID-19.
This study had several limitations that must be acknowledged. Firstly, the collected data were self-reported by the respondents through an online questionnaire. Self-reported data cannot be independently verified and may be prone to response bias, such as exaggerated or understated responses by individuals. Secondly, the poorly chosen distribution channels through social media can lead to biased data and limit the generalizability of the findings. Finally, most of the respondents were highly educated and from the Makkah region. Vulnerable people in Saudi Arabia, such as rural people with low educational levels, are more likely to have poor knowledge, negative attitudes, and inappropriate preventive practices. Further studies to assess KAP towards COVID-19 dental infection control among these individuals are recommended.
CONCLUSION
During the coronavirus pandemic, highly educated Saudi citizens demonstrated good knowledge and optimistic attitudes towards maintaining safe practices regarding minimizing the spread of COVID-19 in the dental setting. This suggests that the massive public health education programs guided by local government and the Ministry of Health are helpful.
LIST OF ABBREVIATIONS
| WHO | = World Health Organization |
| KAP | = Knowledge, Attitude, and Practice |
| CDC | = Centres for Disease Control and Prevention |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study received approval from the Institutional Review Board of Umm Al-Qura University, Saudi Arabia, with ethical approval number 172-2020.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
All participants signed the consent before participating in the study.
AVAILIBILITY OF DATA AND MATERIALS
The data that support the findings of this study are with the corresponding author, [M. R] and can be made available upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflicts of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The author would like to thank all the participants involved in this study for their cooperation.

