All published articles of this journal are available on ScienceDirect.

Is Ultrasonography Efficient for the Detection of the Zygomatic Arch, Nasal Bone and Cartilage Fractures?
Authors Info & Affiliations
Abstract
Background:
The high incidence of nasal and zygomatic arch fractures highlights the need for an accurate imaging modality for their detection. The superimposition of structures is a major problem in conventional radiography. Ultrasonography is a low-cost imaging modality with a wide range of applications, that does not employ ionizing radiation. This study aimed to assess the efficacy of ultrasonography for the detection of the zygomatic arch and nasal bone fractures.
Materials and Methods:
This study was conducted on 16 sheep heads. Artificial fractures were created in some parts of the zygomatic arch, dorsum and lateral wall of the nose, and nasal cartilage. All sheep heads underwent Cone-Beam Computed Tomography (CBCT) to ensure the presence of a fracture. Next, the lateral nasal and submentovertex radiographs were obtained, and ultrasonography was performed with a 12-15 MHz linear probe. Ultrasonography and radiography were repeated after 1 week to assess their reproducibility by calculating the kappa coefficient. Data were analyzed using Stata 11 software and Chi-square test.
Results:
The specificity and sensitivity of ultrasonography ranged from 87% to 100%, and 50% to 75%, respectively. The specificity and sensitivity of radiography ranged from 87% to 100%, and 62% to 87%, respectively. The differences between the two imaging modalities were not statistically significant (p>0.05). The kappa coefficient ranged from 46% to 100% for ultrasonography and 44% to 87% for radiography.
Conclusion:
Ultrasonography seemed useful for the detection of displaced bone and cartilage fractures. For non-displaced fractures, US is not recommended.
1. INTRODUCTION
Clinicians may use several imaging modalities for accurate diagnosis and treatment planning in patients with signs and symptoms of facial bone fractures. The complexity of facial bones highlights the need for an accurate imaging modality for their radiographic examination [1]. Among the facial bones, the nasal bone is particularly vulnerable to injury and fracture due to its prominence [2]. The symptoms suggesting nasal bone fracture include deformity of the nose, edema, epistaxis and periorbital bruising; while, crepitus and mobility of part of the nose strongly suggest nasal fracture [2]. Factors such as the direction and magnitude of force applied to the nose, the nature of trauma, the patient's age and some other patient-related factors can affect the type of damage to the nasal bone and cartilage [2]. Displacement of fracture pieces usually takes place in young individuals while the bone is often crunched in the elderly due to osteopenia. Cartilage and greenstick fractures are more common in children due to incomplete ossification of nasal bone [2]. Thin nasal bones beneath the intercanthal line and humpy noses are more susceptible to fracture compared with thick nasal bones, which are at the bottom of this line [2]. Misdiagnosis of nasal fracture can cause complications such as external deformity, nasal obstruction, nasal septum perforation and even chronic sinusitis in the long-term. Correct management of nasal fractures would minimize such complications as well as the need for reconstructive surgical procedures such as delayed septorhinoplasty [3]. A nasal fracture is diagnosed by clinical examination and conventional radiography. Imaging plays a critical role in correct diagnosis and management of bone fractures. In some cases, conven-tional radiography may have limitations in the diagnosis of nasal fracture due to the high rate of false-positive results and the inability to distinguish old fractures from new ones. Computed tomography (CT) can be used in case of severe trauma and suspected damage to the nose and its adjacent structures to determine the extent of injury [2].
Conventional radiography is often used as the first diagnostic tool. However, it has some shortcomings, such as the use of ionizing radiation and the need for specific patient positioning during radiography; whereas, sonography does not employ ionizing radiation and is easy to use in trauma patients [4].
Zygomatic arch fractures account for 10% to 16% of zygomatic bone fractures [5]. In order to diagnose a zygomatic arch fracture, conventional radiographic modalities such as submentovertex and Waters are first requested. In complex cases, CT may be required as well. At present, CT is used as the imaging modality of choice in midfacial fractures [6]. In the treatment of zygomatic arch fractures, imaging is necessary in order to determine the exact location of the fracture and for proper repositioning of fractured pieces. Submentovertex radiography is also an imaging modality of choice for this purpose [3]. Currently, sonography is used for soft tissue evaluation and diagnosis of orbital fractures due to its availability, simplicity, non-invasiveness, and no use of ionizing radiation, which make it an ideal diagnostic modality particularly for pregnant women and children [1, 4]. Cone-beam computed tomography (CBCT) is a relatively new imaging modality, which was first used for angiography and then for the midfacial area in 1982. It uses a cone-shaped x-ray beam three-dimensionally with a detector to create multiplanar images, which are obtained only by full-rotation scanning around the region of interest [7].
Nezafati et al. showed that sonography was comparable to CT and conventional radiography in sound arches, and had 100% specificity and 88% sensitivity for the detection of fractured arches [4]. Lee et al. compared high-resolution sonography with CT and conventional radiography for the diagnosis of nasal fractures. The results of ultrasonography and radiography were compared with clinical and surgical diagnoses [8]. Thiede et al. compared sonography and conventional radiography for the diagnosis of nasal fractures. They showed that ultrasonography was more accurate than conventional radiography in the diagnosis of lateral nasal wall fractures, while radiography was more accurate for the diagnosis of nasal dorsum fractures [9]. Since nasal bone and zygomatic arch fractures are common facial bone fractures, this study aimed to compare the diagnostic accuracy of sonography and conventional radiography for the detection of the nasal bone and zygomatic arch fractures.
2. MATERIALS AND METHODS
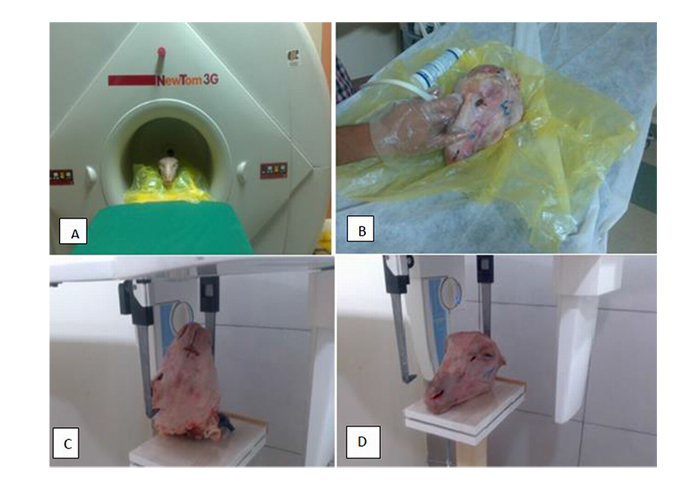
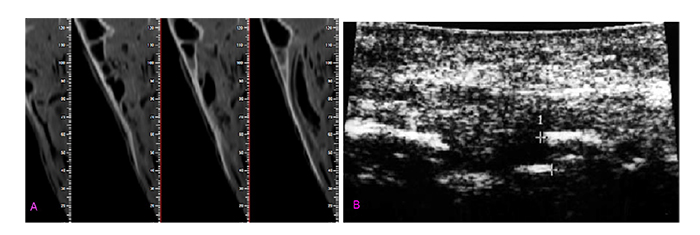
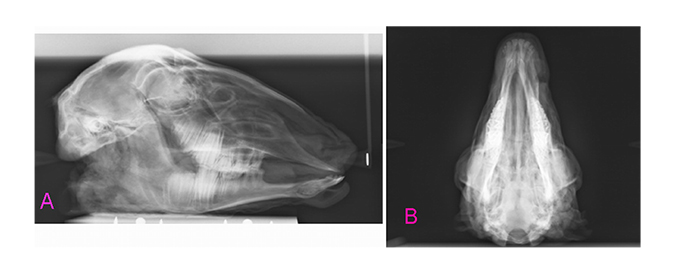
This study was approved by the ethics committee of Hamadan University of Medical Sciences (Res. Project: p/16/35/2215). This study was conducted on 16 sheep heads. Five zones, namely the nasal dorsum, lateral nasal wall, upper lateral nasal cartilage, and left and right zygomatic arches, which are more prone to fracture in accidental trauma, were evaluated. A total of 80 zones were evaluated, out of which 40 zones remained intact to serve as control sites. Fractures were induced using a 1-kg metal hammer. After the creation of the fractures, CBCT scans were obtained to ensure the presence of fracture zones and identify the areas of unwanted fractures. All CBCT scans were obtained by the NewTom 3G volume scanner (QR SRL, Verona, Italy) with the exposure settings of 110 kVp, 2.8 mA, 3.6 s time and 12-inch field of view (Figs. 1A and 2A). Next, ultrasonography (Medison, Samsung, Suwon, South Korea) was performed with a 12-15 MHz linear probe (Figs. 1B, 2B), and submentovertex and lateral nasal radiographs were obtained by Scara II X-ray unit (Planmeca, Helsinki, Finland) with the exposure settings of 68 kVp, 10 mA and 15.3 s time (Figs. 1C, 1D, 3A and 3B).
The sheep heads were coded as follows: Firstly, the nasal cartilage zones were randomly coded in terms of presence / absence of fracture and then, other zones were coded according to the presence/absence of fractures in the head. The radiologists were not aware of the sound and fractured zones (blind design). Next, the results of radiography and sonography were examined by determining the fracture areas with direct observation as the gold standard. In order to assess the reproducibility of the results, each sheep head underwent ultrasonography and radiography again after 1 week, and all images were evaluated by two oral and maxillofacial radiologists on a 17-inch 32-bit monitor (SyncMaster 740 N, Samsung, Korea) with 1280×1024-pixel resolution in a semi-dark room. The results were recorded in a checklist. The observers were allowed to change the brightness and contrast of the images to obtain ideal visual conditions required for diagnosis. Moreover, to calculate intraobserver reliability, each observer was requested to analyze the same images again 1 week later.
The data were analyzed using Stata 11 software (StataCorp.) and the chi-square test. The level of agreement between the imaging modalities was determined and the intra- and inter-observer agreements for each modality were calculated with a 95% confidence interval for the means using kappa statistics. The sensitivity, specificity and accuracy of imaging modalities were also calculated.
3. RESULTS
The inter-observer agreement between the first and the second observer was calculated to be 0.82, according to Kappa statistics for different radiographic modalities, which indicated excellent agreement between the observers. According to Table 1, the specificity of ultrasonography ranged from 87% to 100%. The sensitivity of ultrasonography ranged from 50% to 75%. The specificity of radiography ranged from 87.5% to 100% and its sensitivity ranged from 62% to 87%. The differences between the specificity and sensitivity of the two modalities were not significant (p>0.05).
Sensitivity (also called the true positive rate, the recall, or probability of detection in some fields) measures the proportion of actual positives that are correctly identified as such (e.g., the percentage of sick people who are correctly identified as having the condition).
As shown in Table 1, the highest correlation between sonography and radiography was observed in the detection of lateral nasal wall fractures. Furthermore, sonography had higher accuracy and reproducibility for the detection of nasal cartilage fractures. The situation was reversed for the diagnosis of nasal dorsum fractures, and radiography was superior for this purpose. The two modalities had almost similar accuracy in the detection of zygomatic fractures.
The P-values for the differences in sensitivity and specificity of sonography and radiography for the diagnosis of fractures in different areas are presented in Table 2. As shown, in all areas, no significant differences were observed between sonography and radiology in sensitivity or specificity (p>0.05). Both modalities showed higher positive predictive values than negative predictive values for all fractures, which means that the probability of subjects with a positive diagnosis of fracture (to truly have the fracture) was greater than the probability of subjects with a negative diagnosis of the fracture (not having the fracture).
4. DISCUSSION
CT, similar to other radiation-dependent techniques, has disadvantages such as high patient radiation dose, and increased risk of cataract, that limit its application in some patients and particularly in pregnant women [4]. Thus, it is imperative to find an efficient alternative to CT for special cases/circumstances (time shortage, unavailability of CT scanner, pregnant women, etc.).
The human skull of cadaver which was the best for this research was not available to us, and among animals, the monkeys have the best similarity, but because of ethical consideration, we could not use their head, so we used the sheep’s head because of the presence of nasal bone and cartilage and zygomatic arch which is very similar to the human skull. The sheeps’ heads were obtained from the industrial slaughter house of our city.
Akizuki et al. were the first to examine the position of zygomatic arch after surgery in three patients with zygomatic arch fractures in 1990 using ultrasonography. They introduced ultrasonography as a novel technique for the diagnosis of zygomatic arch fractures [10].
In the present study, ultrasonography was performed using a 12-15 MHz high-frequency linear probe. Furthermore, submentovertex and lateral nasal radiographs were obtained from 40 zones with fractures and 40 sound control zones. According to the kappa coefficient, the accuracy of ultrasonography for the detection of nasal cartilage fractures was 75%, which was excellent and means that ultrasonography has acceptable accuracy for this purpose. In addition, its reproducibility was 65%. The specificity and sensitivity of radiography for the diagnosis of nasal cartilage fractures were 87.5% and 62.5%, respectively. Its accuracy was 50% and its reproducibility was 46.67%, which was in the fair-good range according to the kappa coefficient. Statistically, there was no significant difference between the accuracy of ultrasonography and that of radiography (P>0.05). Ultrasonography can be the preferred choice for the diagnosis of nasal cartilage fractures due to its higher accuracy and reproducibility. For the detection of nasal dorsum fractures, there was no significant difference between ultrasonography and lateral nasal radiography in sensitivity or specificity (p>0.05). However, the accuracy of radiography was higher according to the kappa coefficient. The results of the present study are not consistent with the results of Fouad et al [11]. They showed that ultrasonography was superior to radiography for the diagnosis of nasal fractures. In the present study, although ultrasonography was performed with a 12-15 MHz probe (high frequency is superior for revealing the details due to higher resolution), 5 out of 8 zones with nasal dorsum fractures did not have displacement while in the study by Fouad et al. [11], 93% of the zones had crepitus and displacement and thus, ultrasonography had a poorer performance in the mentioned study. It is noteworthy that the displacement of bone fragments did not occur in cases in whom the fractures were not detected by ultrasonography. This finding confirms the statement by Friedrich et al., that reads, “the most important limitation of sonography is its inability to diagnose the damages without displacement”. Friedrich et al. conducted a study on 32 patients with 39 confirmed mandibular condyle fractures. They used a 7.5 MHz applicator and reported that the fractures were diagnosed in only 67% of the cases. Thus, they did not recommend sonography as an alternative for the diagnosis of mandibular condyle fractures [12]. Furthermore, Fouad et al. [11] reported that the only problem of ultrasonography was the lack of possibility of localizing the fractures in the report provided to the doctor [11].
| Studied Area |
Sensitivity of Radiography (%) |
Specificity of Radiography (%) | Accuracy of Radiography (%) | Sensitivity of Sonography (%) | Specificity of Sonography (%) | Accuracy of Sonography (%) | Reproducibility of Radiography (%) | Reproducibility of Sonography (%) | Correlation between Radiography and Sonography |
| Nasal cartilage | 62.50 | 87.50 | 50.00 | 75.50 | 100 | 75.00 | 46.67 | 65.67 | 46.00 |
| Nasal dorsum | 75.00 | 100 | 75.00 | 50.00 | 87.00 | 37.00 | 84.64 | 44.62 | 66.62 |
| Lateral nasal wall | 75.00 | 87.50 | 62.50 | 75.00 | 87.50 | 62.50 | 87.10 | 73.00 | 90.00 |
| Zygomatic arch | 87.00 | 100.00 | 87.00 | 62.00 | 87.00 | 50.00 | 62.50 | 87.10 | 61.29 |
| - | Sensitivity of Radiography (%) | Sensitivity of Sonography (%) | p-value | Specificity of Radiography (%) | Specificity of Sonography (%) | P-value | - |
|---|---|---|---|---|---|---|---|
| Nasal cartilage | 62.5 | 75.5 | 0.704 | 87.5 | 100 | 0.484 | |
| Nasal dorsum | 75 | 50.00 | 0.273 | 100 | 87.5 | 0.484 | |
| Lateral nasal wall | 75 | 75 | 1 | 87.5 | 87 | 1 | |
| Zygomatic arch | 87 | 62 | 0.220 | 100 | 87 | 0.484 | |
Both ultrasonography and radiography showed 75% sensitivity and 87.5% specificity in the assessment of the lateral nasal surface in our study. The correlation between ultrasonography and radiology was 90.1% in the diagnosis of lateral nasal wall fractures. Such a high correlation indicates that radiography can be replaced by ultrasonography for the diagnosis of lateral nasal wall fractures. In the lateral nasal zone, the nasomaxillary suture and the nasociliary nerve play significant roles in creating false-positive results, and decrea-sing the specificity. Similar studies reported higher accuracy of ultrasonography for the diagnosis of lateral nasal wall fractures and explained the reason to be the lower impact of anatomical landmarks on the diagnosis made by ultrasonography compared with radiography [8, 9, 11] According to the kappa coefficient, the correlation between ultrasonography and radiography was 66.1% for the diagnosis of zygomatic arch fractures, which is in the fair-good range and statistically, there was no significant difference between the sensitivity and specificity of the two modalities (p>0.05). This result was consistent with the findings of Nezafati et al. [4], who suggested ultrasonography as a suitable alternative to radiography for the diagnosis of zygomatic arch fractures. However, Friendrich et al. [12] stated that since accurate treatment planning after the diagnosis of a possible fracture is not easily possible, it is imperative to request other radiographies in order to verify the diagnosis and examine the anatomy of the area. However, their study had a number of limitations because ultrasonography was performed by 2 operators and there was a personal error.
McCann et al. [1] evaluated 22 patients with zygomatico-orbital fractures in different zones with different degrees. They concluded that CT is necessary for the diagnosis of the orbital floor and medial wall fractures, and ultrasonography alone is not sufficient for this purpose. According to them, emphysema-induced swelling, pain and tenderness at the site of fracture were responsible for decreased patient satisfaction. They concluded that although sonography cannot serve as an alternative to CT, it is an inexpensive and accurate supplement to conventional radiography in the diagnosis of facial fractures in trauma patients. Moreover, they showed that emphysema and swelling made it impossible to reach the diagnosis of the fracture using ultrasonography. However, this problem was solved in a study conducted by Gulincher et al. [13]. In their study, ultrasound with a frequency equal or less than 7.5 MHz was used to penetrate thick layers of soft tissue. They stated that emphysema did not occur in single zygomatic arch fractures, and emphysema and edema occurred more in direct contact with the sinus wall fractures. Our study was conducted on sheep heads; thus, emphysema and edema (soft tissue swelling) were not present to affect the results. Pain during imaging (which is one of the disadvantages of sonography) was not present either, which may explain the acceptable accuracy of ultrasonography in the diagnosis of zygomatic arch fractures in our study. As a result, ultrasonography with both high (in order to increase the resolution for the diagnosis of fractures with small displacement) and low (in order to overcome soft tissue edema) frequencies and by experienced clinicians can provide acceptable results in the diagnosis of maxillofacial fractures. Finally, it should be mentioned that saving time is one of the advantages of ultrasonography. The time required to completely examine the zygomatic fractures by ultrasono-graphy is about 15 minutes, which is much shorter than the time required for CT (25 minutes) [14, 15].
CONCLUSION
Sonography is useful for the detection of bone and cartilage fractures. Its main shortcoming is its inability to detect non-displaced fractures. While it is useful for displaced fractures.
ETHICS APPROVAL AND CONSENT TO PARTI-CIPATE
This study was approved by the ethics committee Hamadan University of Medical Sciences, Iran, with approval no p/16/35/2215.
HUMAN AND ANIMAL RIGHTS
The work reported experiments involving animals and reported experiments in accordance with the standards of the UK: The Animals (Scientific Procedures) Act 1986 Amendment Regulations (SI 2012/3039).
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS:
All data generated or analyzed during this study are included in this published article.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

