All published articles of this journal are available on ScienceDirect.

Effects of the Ferrule Design on Fracture Resistance to Endodontically-Treated Teeth Restored with Fiber Posts: A Systematic Review
Authors Info & Affiliations
Abstract
The ferrule is considered to be a key element in teeth preparation when restoring using a fiber post. It helps to resist occlusal forces, maintain cement tightness and minimize stress concentration on restoration using posts.
Aim:
The aim of this review is to determine the influence of the ferrule design in endodontically-treated teeth using fiber posts on their fracture resistance.
Materials and Methods:
The electronic databases examined were Medline, Scopus, and PubMed from April 2019 to October 2019. The studies were selected using well-established inclusion criteria.
Results:
In total, 79 articles were identified, 16 of which were selected after considering the titles and abstracts. After reading the full-text articles, the total number of articles included in this review was 7 with a low risk of bias.
Conclusion:
A full ferrule with a maximum height is the best design for resistance to fractures in all groups of teeth, but if it is impossible to provide this condition, the ferrule height from the palatal/lingual wall of the tooth should be increased.
The PROSPERO ID: 153543.
1. INTRODUCTION
Endodontically-treated teeth have a higher risk of biomechanical failures compared with healthy teeth [1-4]. The survival rates of such teeth are affected by various parameters, which may be partially dependent on the dentist experience, the post system [5], the presence of a ferule [6-8] and the final restoration [9, 10].
There are a number of studies focused on what material to use for the post manufacture [11]. Currently, materials used for the post include gold alloys [12], stainless steel [13], titanium [14], zirconium dioxide [15] or more “flexible” fiber materials, with similar dentine physical properties [16].
It is suggested that fiber posts improve the mechanical properties of composite build-ups. However, the use of fiber posts does not improve their tensile strength [17, 18].
The amount of residual coronal tissue has been reported as an important factor affecting the biomechanical behavior of teeth restored using fiber posts after endodontic treatment [19]. At present, a technique has been described in which the “outer ring” is retained when creating parallel walls of the dentin along the crown to the preparation shoulder. This feature is called ferrule or ferrule-effect [20, 21], which protects the root from fractures, reducing the stress concentration created by the masticatory function [21, 22]. For example, Magne et al. [23] concluded that strengthening the tooth using fiber posts does not increase the bearing capacity and durability of all-ceramic crowns, and the fiber post itself does not compensate for the absence of a ferrule.
At present, there is a controversial opinion regarding the effect of the ferrule design when restoring endodontically-treated teeth using fiber posts [24-30], and a recent meta-analysis showed that the role of the ferrule in these situations is still not fully understood [31].
Thus, the aim of this literature review is to determine the effect of a ferrule design on endodontically-treated teeth using fiber posts on their resistance to fractures.
2. MATERIALS AND METHODS
2.1. Eligibility Criteria
Publications that met the following selection criteria were included:
- Full-text articles in English, not older than 10 years.
- In vitro and in vivo studies on both human and animal teeth.
- Studies having data on the design of the ferrule.
- Teeth after endodontic treatment restored using fiber posts and dental composite.
Publications that were not related to the topic of the study, case reports, literature reviews, as well as articles that did not have sufficient and specific data for the analysis were excluded.
2.2. Information Sources
The electronic databases examined were Medline, Scopus, and PubMed. There was no restriction regarding dates and search in the gray literature. A manual search of the references cited in the included publications was also performed. It was not necessary to contact the authors to access the articles. The search started in April 2019 and ended in October 2019.
2.3. Search and Selection of Studies
A search in English with no time limit was performed by three independent people. The following search query was used: [crown ferrule AND fiber post AND endodontically-treated teeth]. The studies were filtered and selected in several stages. Firstly, they were evaluated by titles. Secondly, individual documents at the first stage were additionally assessed by reading the abstracts and full-text articles. The difference in the choice was resolved through discussion among the readers.
2.4. Risk of Bias Assessment
The assessment of the risk of bias was undertaken during the data extraction process. For the included studies, it was conducted using the Cochrane Collaboration’s two-part tool for assessing the risk of bias [32, 33]. Overall risk of bias was then assigned to each trial, according to Higgins et al. [33]. The levels of bias were classified as follows: low risk, if all the criteria were met; moderate risk, when only one criterion was missing; high risk, if two or more criteria were missing; and unclear risk, if there were very few details to make a judgement about a certain risk assessment.
3. RESULTS
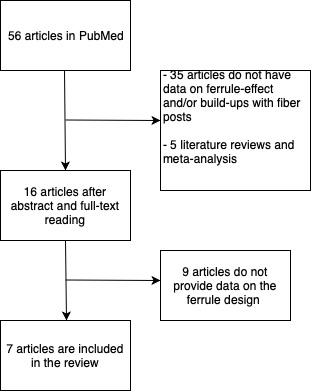
3.1. Selection of Articles
In total, 79 articles were identified, 16 of which were selected after considering the titles and abstracts. After reading the full-text articles, the total number of articles included in this review was 7 (Fig. 1).
3.2. Description of the Studies
The characteristics of the 7 included studies are presented separately in Table 1. These studies were published between 2014 and 2018. All the studies were in vitro conducted on human teeth, with the exception of one study [24], and spanned all groups of teeth. The number of teeth included in the review was 150.
3.3. Results of Individual Studies
This literature review includes various ferrule designs. The designs are described with regards to teeth and teeth sections (sides). The height of the ferrule ranged from 0 mm to 3 mm. The tests were mainly carried out using universal testing machines. More detailed information and conclusions about the impact of design on each study are presented in Table 2.
3.4. Risk of Bias within Studies and Across Studies
Summarizing the risk of bias for each study, most of the studies were classified as an unclear risk. A number of studies were considered as having a low risk of bias. There were several limitations present in the current review, including studies written in English only, which could introduce a publication bias. There were various degrees of heterogeneity in each study design, case selection, and treatment provided among the studies
4. DISCUSSION
There is a generally accepted opinion that ferrule is the most important mechanical factor for the strength of endodontically-treated teeth [1, 7, 21]. The presence of an adequate ferrule reduces the effect of the post system and the final restoration on the survival of endodontically-treated teeth [1].
In all the studies [25-30], except for the study of Figueiredo et al. [24], it was shown that for all the groups of teeth, the larger the circumference of the ferrule, and the more sides involved in creating the incomplete ferule, the greater the resistance of the endodontically-treated teeth to fractures.
| Author | Publication Year | Materials | Number of Teeth | The Group of Teeth | Build-up |
| Figueiredo et al. [24] | 2018 | In vitro; bovine teeth | 50 | Incisors | VIPI Flash self-curing composite, VIPI, Pirassununga, Brazil) and fiber psot |
| Dua et al. [25] | 2016 | In vitro; human teeth extracted for orthodontic indications, no caries lesions | 50 | Mandibular molars | Glassix fiber posts (Harald Nordin sa, Chailly / Montreux, Switzerland) are cemented using RelyX Unicem (3M ESPE, St. Paul, Minnesota, USA) and using a composite material (LuxaCore, Germany). |
| Haralur et al. [26] | 2018 | In vitro; human extracted teeth, no caries lesions | 50 | Mandibular premolars, maxillary canines | Fiber posts (RelyX Fiber post, 3M ESPE, Maplewood, MN, USA), composite resin (RelyX Unicem, 3M ESPE, Maplewood, MN, USA) composite material posterior (Filtek, 3M ESPE, Maplewood, MN, USA). |
| Kar [27] | 2017 |
In vitro; excluded any defects or cracks, fillings or caries and previous endodontic restoration. I |
40 | Mandibular premolars | Fiberg posts (Reforpost, Angelus), double-cured cement RelyX U200, composite material. |
| Meng [28] | 2018 | In vitro; teeth extracted for orthodontic indications | 40 | Mandibular premolars | Fiber posts, cement (cement DUAL-LINK, BISCO, Inc), composite material (Light-CoreTM, Bisco, Inc). |
| Muangamphan [29] | 2015 | In vitro; removed human teeth; any defects or cracks, fillings or caries are excluded | 60 | Maxillary incisors | Fiber posts, composite resin (PermaCem, DMG Inc., Hamburg, Germany), composite material (LuxaCore, DMG Inc., Hamburg, Germany). |
| Zhang [30] | 2014 | In vitro; human teeth removed; any defects or cracks, lesions or caries are excluded | 60 | Maxillary incisors | Fiber posts, composite resin (PermaCem, DMG Inc., Hamburg, Germany), composite material (LuxaCore, DMG Inc., Hamburg, Germany). |
| Author | Year | Ferrule Design | Results |
| Figueiredo et al. [24] | 2018 | - No ferrule - Full 2 mm ferrule - 2 mm ferrule only from the buccal side - 2 mm ferrule from the lingual side - 2 mm ferrule from the lingual and buccal sides |
The ferrule design does not affect the biomechanical behavior of the incisors after endodontic treatment, that were restored using fiber posts, under cyclic loading. |
| Dua et al. [25] | 2016 | - No ferrule - Full 2 mm ferrule - 2 mm ferrule only from the buccal side - 2 mm ferrule from the lingual side 1) from the lingual side 2) – 2 mm ferrule from the lingual and buccal sides with undercuts from the approximal sides. |
The maximum resistance to fractures was achieved in the group with a full ferrule and in the group with a buccal ferule. |
| Haralur et al. [26] | 2018 | 1) 1) Full 2 mm ferrule 2) 2) 2 mm ferrule on the buccal side and 0.5 mm on the palatal side 3) 3) 2 mm ferrule from the palatal side and 0.5 mm from the buccal side 4) 4) 2 mm ferrule on the lingual and buccal sides, with a 0.5 mm ferrule on the approximal sides 5) 5) No ferrule |
1) 1) The presence of a 2 mm ferrule significantly improves fracture resistance 2) 2) Teeth with an incomplete ferrule are much more effective in resisting the destruction compared to its complete absence 3) 3) The absence of a ferule in the proximal area, both in the area of the front teeth and in the area of premolars, does not significantly affect the resistance to fracture 4) The absence of a ferule on the lingual side significantly reduces resistance to fractures. |
| Kar [27] | 2017 | 1) Ferule is absent 2) 1 mm ferule 3) 2 mm ferule 4) 3 mm ferule |
Increasing the length of the ferrule can significantly increase fracture resistance. |
| Meng [28] | 2018 | 1) 1) - 0 mm ferrule with buccal and 2 mm from the lingual side 2) 2) - 1 mm ferrule from the buccal side and 3 mm from the lingual side 3) - 2 mm ferrule from the buccal side and 4 mm from the lingual side |
Resistance to fractures in endodontically treated teeth with a high inclined ferrule was the highest, regardless of the type of load. |
| Muangamphan [29] | 2015 | 1) - Full ferule 2) - Ferrul from the buccal side, from the palatal side and from the mesial side. 3) - Ferrul from the buccal side, from the palatal side. 4) - Ferrul from the palatal side 5) - Ferrul from the buccal side 6) - Ferrul is absent |
Incomplete ferrule may affect fracture resistance in the restoration of endodontically treated anterior teeth |
| Zhang [30] | 2014 | Group 1 (as a negative control): 0 mm from the buccal side and 0 mm from the palatal side. Group 2: 1 mm from the buccal side and 0 mm from the palatal side. Group 3: 2 mm from the buccal side and 0 mm from the palatine side. Group 4: 0 mm from the buccal side and 1 mm from the palatal side. Group 5: 0 mm from the buccal side and 2 mm from the palatal side. Group 6 (as a positive control): 2 mm from the buccal side and 2 mm from the palatal side. |
The height of the ferrule on the palatal side can effectively protect the surface of the build-up border, preventing damage from expanding the layer of adhesive cement |
Although the study by Figueiredo et al. [24] was performed on bovine teeth, the dentin of such teeth is generally considered to be similar to human dentin in composition [34, 35]. Due to the lack of availability and large natural anatomical variations of the extracted human teeth (age, size and shape), bovine teeth allow the use of standardized samples, which is of paramount importance and allows minimizing mixed variables and obtaining sensitivity during testing [23]. Thus, in vitro studies on bovine teeth cannot be neglected, and it is important to take into account the limitations of human teeth.
In clinical practice, a full 1.5 mm ferrule [36] was proposed as the main requirement to achieve a good prognosis; however, this literature review showed that the best results were achieved when creating a 3 mm ferrule. Despite the fact that in most studies, the maximum ferrule was 2 mm in height because it was believed that an additional increase in the ferrule height did not have any advantage in terms of resistance to fracture, these studies evaluated the effect of different configurations of the ferrule when Kar [27] evaluated the effects of different ferrule heights in the same configuration.
With a significant destruction of the crown and the difficulties in creating a homogeneous ferrule, teeth with an incomplete ferrule are much more effective in resisting the fractures compared to the teeth with the complete absence ferrule [25-30]; however, there are disagreements in the articles about which side the ferrule should be higher [25, 26, 28, 30]. The masticatory force vector mainly has occlusal-gingival direction and buccal-lingual directions at approximately 45°, thus increasing the height of the palatal wall in difficult situations reinforces the important role of the lingual/palatal wall when creating a ferrule for resistance to fractures.
CONCLUSION
Although most of the studies had limitations, it can be concluded that a full ferrule with a maximum height is the best design for resistance to fractures in all groups of teeth, but if it is impossible to provide this condition, the height of the ferrule from the palatal / lingual wall of the tooth should be increased.
CONSENT FOR PUBLICATION
Not applicable.
STANDARD FOR REPORTING
PRISMA guideline and methodology were followed.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

