All published articles of this journal are available on ScienceDirect.

Enhancing Dental Carving Skills of Preclinical Dental Hygiene Students Using Online Dental Anatomy Resources
Authors Info & Affiliations
Abstract
Background:
A key role of dental carving is enhancing manual proficiency and dexterity of dental hygiene students. Yet, utilizing Supplementary Online Dental Anatomy Resources (SODAR) as a supportive teaching approach has demonstrated the ability to improve carving skills.
Objective:
This study aims to examine the effectiveness of SODAR training in improving the quality of dental carving skills and knowledge among preclinical Saudi male students in Saudi Arabia.
Methods:
A basic double-blinded randomized controlled trial of 30 preclinical Saudi dental male students was conducted between January and April 2019. Participants were classified into an experimental group that received SODAR training (n = 15) and a control group comprising students who did not receive SODAR training (n = 15). The t-test and Fisher’s exact test were performed to assess differences in theoretical knowledge between the two groups. While Cohen’s d test, t-test, and Pearson correlation were conducted to evaluate differences in students’ dental carvings.
Results:
Students with SODAR training performed better on practical carving sessions than those without intervention (P-value < 0.001). However, SODAR intervention had no significant effect on the theoretical knowledge evaluations in both the groups.
Conclusion:
SODAR training demonstrated its ability to support students learning in practical carving sessions; however, no effect on theoretical knowledge was observed. Future research should focus on factors that impact carving teaching strategies, including the quality and depth of online learning content, students’ perceptions of online learning, and experiences of teachers who run the online resources.
1. INTRODUCTION
Dental carving skills are key elements of practical preclinical dental anatomy sessions in the curriculum of Saudi Arabian dental education. Mastering those skills requires massive amount of time and experienced senior dentists. Moreover, integrating several pedagogical resources and multimodal teaching strategies have demonstrated effectiveness in teaching modern anatomy modules [1]. Likewise, undergraduate dental health students should acquire proper theoretical knowledge, and cognitive and psychomotor skills for forming and analysing the shape, function, and aesthetics of each human tooth. Evidence has demonstrated that dental students’ clinical performances in the last years of their dental program could be foreseen from their own dental carving scores at their practical sessions in the preclinical year [2]. Consequently, designing proper learning outcomes, teaching strategies, and assessment methods of dental anatomy modules may play a major role in improving students’ theoretical knowledge and practical dental carving skills.
Several teaching strategies have been used to improve preclinical dental students’ psychomotor skills using the dental anatomy module. These strategies include, but are not limited to, using interactive group discussion, computer-animated graphics, wax block carving, patient scenario-based wax-up sessions, natural teeth, and photorealistic 3D images [3]. However, the most widespread technique for teaching teeth anatomy and morphology in dental faculties worldwide is the use of wax blocks in dental carving [4]. Although using digital media such as DVDs and geometrical dental models has been shown to be an effective learning strategy [5], there has yet been no suitable validated assessment technique that has proven the effectiveness of such teaching strategies on the proper acquisition of dental anatomical knowledge and psychomotor skills for dental students [6].
Saudi dental students’ perceptions towards computer-based and online learning have been shown to be highly preferable [7]. Students may today be more technology-savvy than in the past. Online learning teaching strategy has been shown to make students’ learning experience more enjoyable, interactive, innovative, and clinically applicable [8]. Furthermore, the easy accessibility of online learning for both students and teaching staff and the provision of several online tools have been associated with successful aspects in operating online learning [9]. Therefore, it might be the case that if online learning strategies were properly designed and easily accessed, they would improve dental course learning outcomes and student learning experience.
Using online dental resources as a supportive teaching strategy may improve students' dental carving skills in the dental anatomy and morphology module [4]. This might be particularly true if we consider the amount and quality of time that would be spent on other aspects of academic teaching and research undertaken by both students and teaching staff. The aim of this study, therefore, is to examine the effectiveness of 12 contact hours of Supplementary Online Dental Anatomy Resources (SODAR) training on improving the quality of dental carving skills and knowledge among preclinical, male, Saudi dental hygiene students in Albaha, Saudi Arabia. In other words, do students receiving SODAR training perform better in dental carving sessions and knowledge evaluations than students without SODAR training?
2. MATERIALS AND METHODS
2.1. Overview of Dental Anatomy Module
The dental anatomy module is a key component of undergraduate departmental modules in the dental health program at the Faculty of Applied Medical Science in Albaha University, Saudi Arabia. This module focuses on basic dental anatomy and the morphology of teeth and surrounding tissues in a systematic manner. All aspects of dental anatomy and morphology are comprehensively covered in this module, including, but not limited to, development of primary and permanent dentation, supporting oral structures, dental morphology and anatomy, anatomy of periodontal ligaments, oral cavity, and salivary glands.
The module has an overall workload of 60 contact hours distributed equally between theoretical teaching and practical sessions in proper dental labs. Different teaching strategies are employed including theoretical lectures, preparatory reading of textbooks, oral presentations, group discussions, case studies, and practical sessions. Natural teeth and dental models are also used to enhance dental hygiene students’ knowledge before they start practicing dental carving on wax models. The evaluation methods of this module are mainly based on applications of theoretical tests (mid-term, quiz, and final exam); however, two practical tests that assess the quality of students dental carving and correct identifications of anatomical and physiological aspects of dentation, the oral cavity and structures are also administered.
2.2. Participants and Settings
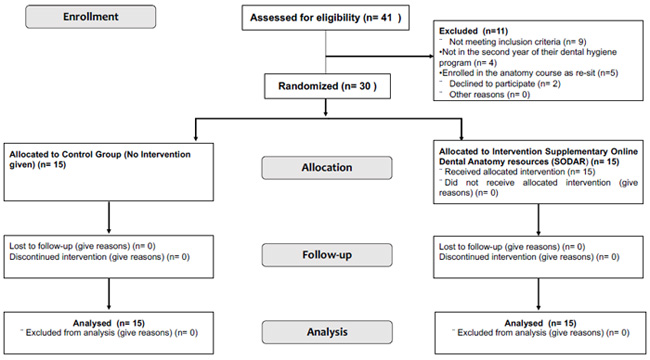
A basic double-blinded parallel-arm randomized controlled trial of 30 preclinical, Saudi, male undergraduate students studying dental hygiene was conducted at the Faculty of Applied Medical Sciences in Albaha University, Saudi Arabia, between January and April 2019. Fig. (1) illustrates the allocation and randomization process of the applicants. All participants met a number of inclusion criteria: 1) They were Saudi male undergraduate students in the third semester (second year) of their dental hygiene program; 2) they were enrolled in the dental anatomy course for their first time and not as a resit; 3) they agreed to contribute to this study and signed the consent forms. Participants were classified into an experimental group, comprising students who received 12 contact hours (12 tutorials) of SODAR training (n = 15), and a control group, comprising students who did not receive SODAR training (n = 15). Herein, the two groups will be referred to as the SODAR group and the control group.
SODAR included watching online videos on proper techniques of carving several teeth, dental morphology and anatomy, and physiological explanations of oral cavity and structures. It could be noted that the SODAR training was designed and validated by the Dental Health Department, Faculty of Applied Medical Sciences, Albaha University in the academic year 2017/2018. All students in the SODAR group did watch the online training together under the similar condition for a single time across four sessions (each session consists of three contact hours). Moreover, a week's time period between the SODAR training and the assessment was implemented and fixed for all students. It should be highlighted that female students were excluded from the study sample because the dental hygiene program was conducted in the male campus, and no females were enrolled in the program throughout the course of the study. Both groups had the same mean age: 20 ± 0.72 years.
2.3. Evaluating Quality of Dental Carving
Two double-blinded examiners assessed the quality of each student’s dental carving in both groups and scored them in a range of 0 to 10 points. It should be emphasized that examiners underwent theoretical training and a standardization process. An intraexaminer agreement was measured using the Intraclass Correlation Coefficient (ICC) and was estimated to be 0.87, indicating great agreement and consistency between the outcomes of the two examiners. The dental carving material used in this study was a green wax carving block with dimensions of 79 x 38 x 28.5 mm and manufactured by Ferris Dental Company, the United States. Carving blocks were randomly numbered and assigned to examiners without them being informed of block numbers.
The maxillary right permanent central incisor (Tooth 11) and maxillary right permanent canine (Tooth 13) were selected for the purpose of evaluating dental carvings of both groups based on the following pre-established criteria and scores. The morphology of Tooth 11 was evaluated by allocating two points for each of the following morphological and anatomical features: 1) presence and outline of the marginal ridge with one mark for each item; 2) presence and shape of lingual fossa and cingulum, one mark awarded for each item; 3) sloping of incisal edge, two marks awarded; 4) convexity of cervical third of labial surface, two marks awarded; and 5) presence and shape of the root, one mark awarded for each item. Similarly, the morphology of Tooth 13 was evaluated by awarding two points for each of the following morphological and anatomical features: 1) the presence and shape of the marginal ridge, with one mark for each item; 2) presence and shape of lingual fossa and cingulum, one mark awarded for each item; 3) presence of incisal edge, mesial and distal slops, and cusp tip, each awarded 0.5, 1.00, and 0.5 marks, respectively; 4) presence and convexity of labial surface, one mark awarded for each item; and 5) presence and shape of the root, one mark awarded for each item.
2.4. Evaluation of Theoretical Knowledge
The theoretical knowledge of all participants was evaluated in both groups by having participants complete a written theoretical questionnaire before and after the SODAR group received the proposed SODAR intervention. The questionnaires consisted of 10 questions, scored them within a range of 0 to 10 points (one point each question), and were designed to focus on identifying different shapes, locations, configurations, characteristics, parts, and tissues of deciduous and permanent teeth; oral cavity anatomy; the alveolar process and its parts; and teeth numbering and coding system. The marks obtained for both groups (control and SODAR) in the dental anatomy module before receiving the SODAR intervention were assessed and compared with the baseline data. Consequently, the SODAR group was asked to fill out the questionnaire after receiving the SODAR intervention, while the control group completed the questionnaire without receiving the SODAR intervention. As mentioned above, although both questionnaires (before and after SODAR intervention) were focused on particular aspects of dental anatomy; they were designed and distributed to students using differently formulated questions.
2.5. Statistical Analysis
Data analysis was performed using Statistical Package for the Social Sciences® software (version 20.0). The t-test was used to compare the means of marks between the control and SODAR groups. Fisher’s exact test was performed to compare the frequency of right answers obtained from both groups in each of the theoretical knowledge questions. Cohen’s d test was also utilized to measure effect sizes between both groups. The correlation between marks achieved prior to the study on the dental anatomy module and marks gained in the carving sessions of this study was conducted using the Pearson correlation test. P-value = 0.05 was considered significant for all analyses.
2.6. Ethical Considerations
Ethical approval was obtained from the Deanship of Scientific Research at Albaha University, Saudi Arabia (approval number, 40142758). It should be highlighted that once the study was completed, the control group was provided with all supplementary online dental anatomy resources that were provided to the experimental group (SODAR) during this trial.
3. RESULTS
3.1. Quality of Dental Carving
A comparison of means and standard deviations of maxillary right permanent central incisor (Tooth 11) carving evaluation marks between the control and SODAR groups revealed statistically significant results (P ≤ 0.0001). Similarly, a significant statistical difference of means and standard deviations of maxillary right permanent canine (Tooth 13) carving evaluation marks (P = 0.001) was observed between the SODAR and control groups. Moreover, the overall dental carving marks of both groups were also significantly different from each other (P ≤ 0.001). These findings demonstrated that the SODAR intervention improved the quality of dental carving among the studied population. In other words, students with SODAR training performed better on practical dental carving sessions than those students who had no SODAR training. Table 1 illustrates the means, standard deviations, and overall marks of dental carving evaluations for both control and SODAR groups.
Effect sizes of dental carving evaluations between the experimental SODAR and control groups were shown to be greater than 1.3 for all values. Hence, this finding in addition to the difference detected by the t-test demonstrated a large effect for the SODAR intervention. Moreover, the Pearson correlation test was used to assess the correlation between marks achieved prior to the study on the dental anatomy module and marks gained in the carving sessions of this study. The Pearson correlation coefficients revealed no significant correlations between the two groups (r = 0.264, P = 0.341), (r = 0.424, P = 0.116) for Tooth 11and Tooth 13, respectively.
3.2. Theoretical Knowledge
The theoretical knowledge evaluations displayed no statistically significant differences in the mean marks of both control and SODAR groups (22.46 ± 5.24; 23.73 ± 4.69, respectively; P = 0.492). However, it should be noted that the SODAR group achieved a slightly higher mean of marks in theoretical knowledge evaluation than the control group. Similarly, no statistically significant differences were observed for the frequency of correct answers obtained from both groups for each of the theoretical questions. Therefore, it can be concluded that the SODAR intervention had no observed significant effect on the theoretical knowledge evaluations for the SODAR groups.
4. DISCUSSION
There has been a growing trend of using online dental resources and programs as supportive teaching strategies in medicine and dentistry [10]. These online resources have proven crucial for teaching and motivating dental students [11]. Evidence has demonstrated that online resources and programs may be used as a replacement for traditional lectures in the dental anatomy module, but not as a replacement of practical dental carving sessions [5, 12]. Likewise, teaching dental anatomy theoretically with no carving sessions may not be sufficient to acquire knowledge relating to the anatomical and morphological aspects of each tooth. Although many anatomists have advocated using a multifaceted approach in teaching anatomy modules [13, 14], online learning resources have demonstrated their ability to improve and support student involvement in interactive learning of dental anatomy courses [15, 16].
The results of this study revealed that the SODAR intervention enhanced the practical psychomotor skills related to dental carving among preclinical dental health students. These findings are consistent with other studies that have suggested using online dental resources as a supportive teaching strategy, rather than as a replacement of traditional teaching strategy [17, 18]. However, there are several factors that may have influenced the findings of these studies, including the learning atmosphere, quality and depth of online learning contents, students’ perceptions and thoughts of online learning, and dental teachers' experiences in running online resources. De Azevedo, Da Rosa [5] conducted a recent systematic review comparing the effectiveness of dental carving during the teaching of dental anatomy and concluded that no standardized teaching technique was widely validated as effective for teaching the dental anatomy module; this highlights the importance of comprehensively reviewing the current dental literature with a focus on including factors that influence dental carving teaching methodologies and evolution.
| - |
Control Group (Mean ± SD) |
Experimental (SODAR) Group (Mean ± SD) |
P-value |
|---|---|---|---|
| Tooth 11 | 4.78 ± 1.35 | 7.38 ± 1.52 | <0.0001 |
| Tooth 13 | 4.73 ± 1.66 | 7.36 ± 2.33 | 0.001 |
| Overall | 4.76 ± 1.51 | 7.37 ± 1.93 | <0.001 |
The findings of the current study indicated that there were no significant differences in the mean marks of theoretical knowledge evaluations between the control and SODAR groups. However, the SODAR group achieved slightly better marks in theoretical evaluations than the control group. Such findings are similar to work conducted in the USA by Howerton et al [19] who concluded that there was no difference between using online learning resources and theoretical lectures in dental learning in terms of student learning outcomes. Nonetheless, including problem-solving techniques in the dental anatomy module has demonstrated the ability to improve the abilities of dental hygiene students in applying their theoretical knowledge to preclinical and clinical cases [20]. Consequently, exploring this area of research in terms of its impact on the psychomotor skills and learning outcomes of dental hygiene students may prove reasonable and useful.
There were two key limitations of this study. Firstly, there were no sample size calculations for the outcome of this study. The sample size of this study might not have been sufficient to uncover any significant difference. Hence, further research should be conducted in several stages of dental courses with proper sample sizes that have the ability to detect any statistically significant differences. In other words, the results could be limited for this sample size and study condition; increasing sample size is required in the future study. Secondly, female students were excluded from the study sample because our dental hygiene program was conducted in the male campus, and no female students were enrolled in the program throughout this study. Unfortunately, this might have affected the generalizability of the results of the current study. However, this trial does offer insight into the effectiveness of SODAR on improving the quality of dental carving skills and knowledge among the studied population in Saudi Arabia.
CONCLUSION
SODAR enhanced the quality of students’ dental carving skills and their ability to sculpt teeth. However, SODAR did not improve the students’ knowledge of dental morphology and anatomy. Future research should focus on factors that impact on dental carving teaching strategies and assessment, including quality and depth of online learning content, students’ perceptions of online learning, and the experiences of teachers who run the online resources. Exploring the effectiveness of problem-solving teaching strategies in theoretical knowledge relating to the dental anatomy module and its relationship to preclinical and clinical applications is also recommended.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Ethics Committee of the Deanship of Scientific Research at Albaha University, Saudi Arabia. (Code #. 40142758).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All research procedures on humans were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013. (http://ethics.iit.edu/ecodes/node/3931).
CONSENT FOR PUBLICATION
Informed consent was obtained from the participants who involved in this study.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available upon request form the correspondence author Alzahrani.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

