
Cone Beam CT-Based Preoperative Volumetric Estimation of Bone Graft Required for Lateral Window Sinus Augmentation, Compared with Intraoperative Findings: A Pilot Study
Abstract
Introduction:
The presence of an atrophic maxilla creates a serious challenge in cases of implant placement, while maxillary sinus pneumatization further complicates the surgery. This pilot study was performed to investigate the validity of two techniques used to estimate the volumes of bone graft material required in cases that included lateral window sinus augmentation.
Materials and Methods:
Cone beam computed tomography was used for preoperative volumetric analysis of the maxillary sinus. The analysis was performed using the manual measurement of sinus dimensions, as well as automated measurements via the segmentation technique. The estimated volumes of required bone graft material were compared with actual intraoperative findings in cases requiring lateral window sinus augmentation. For this pilot study, only 5 patients were selected to be included.
Results:
To achieve 80% power and confidence interval of 95%, the sample size should be 35 patients. The correlation coefficient between the segmented volume and mm3 used was – 0.5332, whereas the coefficient between the manual volume and mm3 used was – 0.6784. Consequently, both results indicate that the two methods have a moderate negative correlation with the mm3 used.
Conclusion:
Performing a similar study with an increased number of patients, according to the calculated sample size, increases the possibility of revealing higher correlation between the methods used to analyze the partial volume of the sinus cavity. The estimated sinus volume of the area of augmentation, obtained by using either manual or segmentation techniques, could be considered as a maximum estimate for the required amount of graft material. Furthermore, the segmentation technique may be valuable in preoperative planning of sinus augmentation, as it reveals the topographic shape and morphology of the sinus.
1. INTRODUCTION
The presence of an atrophic maxilla creates a serious challenge in cases of implant placement, whereas maxillary sinus pneumatization further complicates the surgery. Patients who exhibit both conditions require bone grafting to the maxillary sinus floor to increase the height of the maxillary alveolar bone [1-7]. Lateral window sinus lift or Schneiderian membrane elevation is a common surgical procedure, first published by Boyne and James in 1980, that is used to create a window on the lateral wall of the sinus, as well as a space between the Schneiderian membrane and the sinus walls for the placement of grafting materials. Lateral window sinus lift is an effective procedure to gain bone height to facilitate future implant placement in an atrophic pneumatized posterior maxilla [1].
Preoperative planning includes radiographic assessment of maxillary sinus dimensions. Digital panoramic radiographs have been used [8], but they exhibit no ability to investigate depth. Conventional dental or panoramic radiographs are not suitable for volumetric analysis, as their two-dimensional nature only provides an approximation of sinus graft vertical dimensions. Thus, 3D imaging is required to allow investigation of the presence of bony septa, as well as Schneiderian membrane thickness and residual alveolar bone height [9, 10], thereby allowing the proper design of the lateral wall sinus augmentation.
Several previous studies have used Computed Tomography (CT) as a method for sinus anatomy evaluation and volume calculation [11-14]. Cone Beam CT (CBCT) has also been used with comparable accuracy [9, 15-18].
Generally, the need for decreased postoperative complications at the donor site (during autogenous graft surgeries) necessitates careful preoperative planning of the graft volume to be harvested. The increased cost of allografts leads to further urgency in preoperative planning.
This pilot study was performed to investigate the validity of two techniques used to estimate volumes of bone graft material, required in cases that included lateral window sinus augmentation, through CBCT imaging. The null hypothesis is that there is no statistical significance between the estimated volumes and actual intraoperative findings.
2. MATERIALS AND METHODS
This pilot study included patients who presented to the Department of Periodontology at King Abdulaziz University for the placement of dental implants in the maxillary posterior area. Patients were interviewed and examined to determine their eligibility for the study. Inclusion criteria were as follows: consent for the described procedure as approved by the University’s Institutional Ethical Committee on Human Research, the requirement for lateral wall sinus augmentation prior to dental implant placement, and age ≥18 years. Exclusion criteria were as follows: Ongoing pregnancy, diagnosis with metabolic disorder, immunocompromised status, hemophilia, bleeding disorders, drug or alcohol abuse, treatment with steroids, history of radiation therapy in the head and neck, psychiatric disorders, and/or inability to understand the procedure described in the questionnaire. The statistical tool determined the sample size, which was 35 patients at 80% power and confidence interval of 95%. For this pilot study, only 5 patients were selected to be included.
3D imaging was performed before lateral wall sinus augmentation. CBCT images were acquired using a Next Generation i-CAT scanner (Imaging Sciences International, Inc., Hatfield, USA). A scout (preview) was obtained and adjustments were made to ensure that the patient was correctly aligned in the scanner before acquisition, using the adjustment light beam. The machine was supplied with an Amorphous Silicon Flat Panel Sensor with Cesium Iodide (CsI) scintillator (0.5-mm focal spot size, 14-Bit grayscale resolution) and operated at the following protocol for all the scans of the study: 120 kVp, 37.07 mAs, 8.9 s, 0.4 mm Voxel size, and 13 × 16 cm2 FOV.
Following acquisition, data were exported and transferred in DICOM format, then downloaded via a Compact Disk (CD) to a personal computer for volume measurement, where Mimics software (version 15.1; Materialize, Belgium) was utilized.
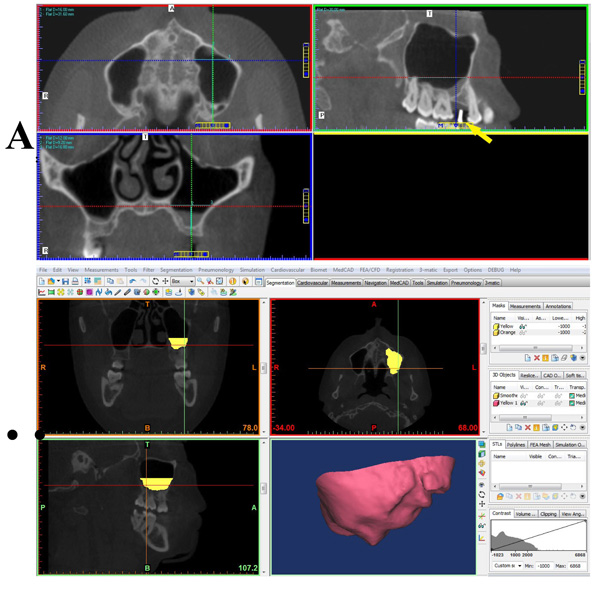
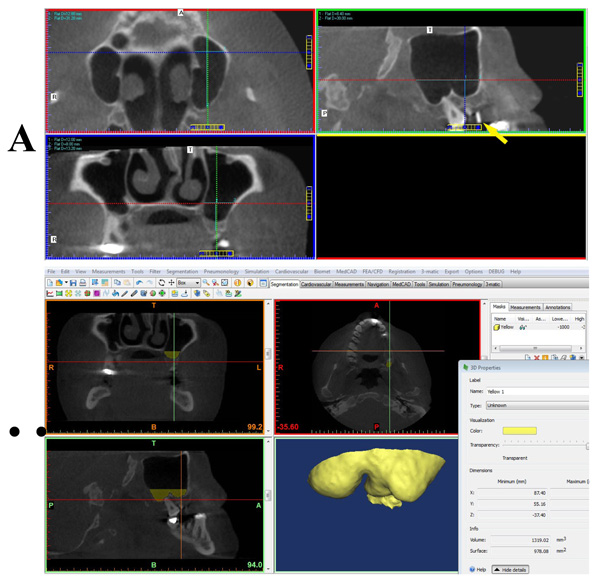
Data were imported into Mimics software; at the coronal view, the edentulous site was viewed, and a 12-mm vertical linear measurement was made from the crest of the ridge upwards (at the area of minimum dimension). Next, the axial reference line was moved to the site at the end of the previous measurement; this level was assigned as the level up to which segmentation of the maxillary sinus space should reach. A certain threshold was assigned to segment the sinus space; then cropping and region-growing tools were used to confine the segmented mask to the maxillary sinus space. Final fine-tuning and clean-up steps were performed at the axial cut sites to ensure the geometry of the segmented mask. After calculating the volume of the segmented mask, the software presented the amount of graft material required to augment the sinus, thereby reaching 12-mm bone height [15].
Additionally, manual measurements were performed of the sinus dimensions and volume calculation. These were dependent on the anatomical fact that the maxillary sinus is pyramidal in shape, with an almost square base that is oriented medially [16]. At the coronal view, the edentulous site was viewed, and a 12-mm vertical linear measurement was taken from the crest of the ridge upwards (at the area of minimum dimension). Next, the axial reference line was moved to the site at the end of the previous measurement; this level was assigned as the level up to which linear measurements will be performed. To obtain the width, length, and height of the sinus, the coronal, axial, and sagittal cuts were sequentially reviewed to acquire maximum sinus mediolateral, anteroposterior, and craniocaudal dimensions.
Finally, radiographic data was compared to intraoperative findings and statistically evaluated by correlation analysis.
This study was approved by the Research Ethics Committee of the Faculty of Dentistry, King Abdulaziz University (No. 009-16).
3. RESULTS
The statistical tool determined the sample size, which was 35 patients at 80% power and confidence interval of 95%.
Results obtained from this pilot study done for 5 patients are as follows: Table 1 represents the correlation coefficient between each of the two methods and mm3 used. The correlation coefficient between the mimics volume and mm3 used was – 0.5332, whereas the coefficient between the manual volume and mm3 used was – 0.6784. The resulting linear regression models were as follows:
Estimated mm3 used = – 0.1865 × Mimics volume + 2094.5
Estimated mm3 used = – 0.4162 × manual volume + 2149
| Actual Volume of Material Used (mm3) |
Estimated Volume from Mimics (mm3) |
Estimated Volume from Manual Calculation (mm3) |
|---|---|---|
| 1500 | 2179 | 1030.36 |
| 2000 | 1997 | 396.03 |
| 2000 | 1319 | 1098.24 |
| 1500 | 1693 | 1241.86 |
| 1500 | 3389 | 1628.03 |
| r | -0.5332 | -0.6784 |
The two models above were used to estimate the mm3 used, based on the given Mimics volume and manual volume values. The residual error was measured and normalized to obtain the coefficient of determination (i.e., R2) of the model. The calculated R2 values for the two models above were 0.2843 and 0.4603, respectively.
Figs. (1 and 2) depict snapshots of manual and Mimics volumetric calculations for the patients.
4. DISCUSSION
In this pilot study, CBCT was used for preoperative volumetric analysis of the maxillary sinus. The estimated volumes of required bone graft material were compared with actual intraoperative findings. Although the determined sample size was 35, considering the nature of this study (pilot), number of patients was limited to five.
To assess the ability of the measured volume parameters to accurately predict the actual mm3 used, the correlation coefficient was evaluated between each of the two methods and the mm3 used. Briefly, the correlation generally measures the existence and strength of a linear model between two variables; the correlation coefficient used produces results between +1 (strong positive linear dependence) and -1 (strong negative linear dependence), with 0 indicating no relationship between the two variables. Thus, the closer the magnitude of the correlation coefficient to 1, the more plausible a linear model is to describe the relationship. The results indicate that the two methods have a moderate negative correlation with the mm3 used.
The next step in estimating the validity of the linear model was to perform a linear regression to generate an estimate of the mm3 used, from the value of either the Mimics volume or the manual volume. Furthermore, to check the goodness-of-fit of the resulting linear models, both models were used to estimate the mm3 used, based on the given Mimics volume and manual volume values. The residual error was measured and normalized to obtain the coefficient of determination (i.e., R2) of the model. This metric has a value between 0 and 1, where 1 designates a perfect linear model. Hence, the larger the value of R2, the better the model to accurately predict the data.
The results of this pilot study were more towards rejecting the null hypothesis. Performing a similar study according to the calculated sample size, may reveal a higher correlation between the methods used to analyze the partial volume of the sinus cavity and actual intraoperative findings. However, in this study, the model based on manual volume exhibited a much better goodness-of-fit.
In a previous study [16], manual calculation of the whole sinus used the laws of geometry to give an estimated volume, which significantly correlated with the estimation via segmentation technique. Previous studies also incorporated manual or automated segmentation to assess sinus or grafted bone volume [13, 14, 19, 20]. Uchida et al. [13, 14] investigated the volume of grafted bone required for sinus floor lifting and determined a range of 4.74-7.96 cm3 graft volume, depending on the height of required sinus floor lift, which ranged from 15-20 mm. It has been also reported that the calculated augmentation volume for an augmentation height of 12 mm was 1.7 ± 0.9 cm3 [21]. These ranges reasonably consistent with the results of this study, as the level of lift was set at 12 mm.
The segmentation technique by Mimics provides additional advantages, as it reveals the topographic shape and morphology of the sinus, thereby informing the surgeon of the anatomical limitations expected. However, the inaccuracy of the model’s goodness-of-fit cannot be disregarded. Thus, the estimated volumes should be used only as a guide. The greater value of the Mimics method (or any other segmentation technique) lies in its accurate morphological representation of sinus anatomy. The resulting 3D shapes provide an ideal preoperative guide for the clinician.
CONCLUSION
Performing a similar study with an increased number of patients, according to the calculated sample size, increases the possibility of revealing higher correlation between the methods used to analyze partial volume of the sinus cavity. The estimated sinus volume of the area of augmentation, obtained by using either manual or segmentation techniques, could be considered as a maximum estimate for the required amount of graft material. Furthermore, the segmentation technique may be valuable in preoperative planning of sinus augmentation, as it reveals the topographic shape and morphology of the sinus.
LIST OF ABBREVIATIONS
| CT | = Computed Tomography |
| CBCT | = Cone Beam Computed Tomography |
| CsI | = Cesium Iodide |
| CD | = Compact Disk |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Research Ethics Committee of the Faculty of Dentistry, King Abdulaziz University (No. 009-16).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2008.
CONSENT FOR PUBLICATION
Informed consent was obtained from all patients prior to being enrolled in the study.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENT
The authors would like to thank Prof. Yasser Moustafa Kadah, Professor of Biomedical Engineering, Faculty of Engineering, King Abdulaziz University, for his valuable assistance in the statistical analysis performed in this work. They would also thank Dr. Ahmad Ali Hassan, Assistant Lecturer of Oral and Maxillofacial Radiology, Faculty of Dentistry, Fayoum University, for his valuable assistance in the Mimics program manipulation.

