All published articles of this journal are available on ScienceDirect.

Dental Erosion and Dentin Hypersensitivity among Adult Asthmatics and Non-asthmatics Hospital-based: A Preliminary Study
Abstract
Background:
Asthma is a chronic inflammatory condition affecting the airways leading to spasm and swelling of the airways. The medications taken for the treatment of asthma can result in dental erosion and dentin hypersensitivity.
Objectives:
The aims of this study were to investigate the severity of dental erosion amongst adult asthmatics according to: gender, type and duration of medication taken and to compare dental erosion and dentin hypersensitivity between asthmatics and non-asthmatics.
Subjects and Methods:
Comparative, cross-sectional hospital based study among 40 asthmatics (M=15 & F=25) and 40 non-asthmatics (M=18 & F=22) in the age range of 18-60 year selected purposefully from Al-Shaab Teaching Hospital in Khartoum city. The Basic Erosive Wear Index was used for dental erosion assessment. Dentine hypersensitivity was determined by giving ice cold water and rated using the Visual Analogue Scale. Chi-square and Student’s t-test were used for statistical analysis with P value ≤.05.
Results:
There was an association between severity of dental erosion and presence of asthma (P=0.03), where asthmatics had a higher degree of erosion (moderate and severe) and non-asthmatics a lower degree. No significant association was found between dental erosion and gender, type and duration of medication among asthmatics group. A statistically significant difference was revealed in the degree of dentin hypersensitivity (P=0.00) among asthmatics (35.13%) and non-asthmatics (14.13%).
Conclusion:
Asthmatic patients had a higher degree of dental erosion and dentin hypersensitivity compared to non-asthmatics. Among asthmatic patients there was no association between severity of dental erosion and gender, type and duration medication was taken for.
INTRODUCTION
Asthma is a chronic inflammatory condition affecting the airways leading to spasm and swelling of the airways. An estimated 300 million people worldwide suffer from asthma [1]. It either resolves spontaneously or responds to a wide range of treatment [2]. Some studies have shown that the medications taken for the treatment of asthma can result in dental erosion [1, 3]. Dental erosion is the irreversible loss of tooth surface by chemicals. It can lead to adverse effect such as irreversible loss of tooth structure, poor aesthetics, loss of vertical dimension and functional problems such as impaired mastication [4]. More specifically, is the exposure of the dentin, which leads to the condition known as dentin hypersensitivity, which is characterized by short, sharp pain arising from exposed dentin in response to stimuli, commonly thermal, evaporative, tactile, osmotic or chemical, which cannot be related to any other form of dental defect or pathology [5].
The prevalence of asthmatics in the population has risen in the later part of the last century [2]. This means a great number of individuals are at risk of developing dental erosion. Simple measures can be undertaken to decrease erosion such as referral of the asthmatic patient by the attending physician to the dentist; or education of the patient on the necessary oral hygiene and preventive measures. Since dental erosion is irreversible, early intervention is required before the side effects of asthmatic drugs start to manifest in the oral cavity. Nevertheless, the results of some studies in the literature are still contradictory about the association of asthma medications and dental erosion. Our null hypothesis is that; there is no association between asthma medication and dental erosion. The aims of this study were to investigate the presence of dental erosion amongst asthmatics according to: gender, type and duration of medication taken and to compare dental erosion and dentin hypersensitivity between asthmatics and non-asthmatics.
MATERIALS AND METHODS
Study Design, Area and Duration
A cross-sectional comparative study was conducted at the emergency asthma unit in Al-Shaab Teaching Hospital between the periods of January to March 2013.
Study Population
The study was composed of asthmatics who were admitted to the short-stay unit due to an acute asthmatic attack. They were asked to participate voluntarily after explaining the purposes of the study and were interviewed and examined after they received a written discharge by their attending doctors. The comparative group of non-asthmatic included their relatives, friends or co-patients who fulfilled the required criteria except for being non-asthmatics. The study’s participants consisted of adults over 18 year old (asthmatics group and non-asthmatics). Asthmatics included in the study were under prophylactics medications in the form of dry powder inhalers and/or pressurized aerosol inhalers and have been diagnosed with asthma for at least one year. Excluded asthmatic or non-asthmatics were those who were taking acidic medicaments such as acetylsalicylic acid and vitamin C; medications which cause reduction of saliva secretion as a side effect (psychotropic drugs, antiemetic, and Parkinson’s medication); patients with anorexia or bulimia; diseases of salivary glands such as Sjögren syndrome or due to radiation of the head and neck region; and those with diabetes mellitus and chronic renal failure. In addition, those who consume soft drinks more than twice a week [6] or with symptomatic tooth or teeth due to causes other than erosion (caries, deep pockets) were also excluded.
Data Collection Methods
A structured interview based questionnaire was carried out, which included questions regarding demographic data and medical history. The procedures for assessment were explained to the participants and their cooperation and understanding of examination test was assured. The participants were seated in comfortable upright chair and examination was carried out with aid of portable artificial light followed by measurement of the erosive wear of the teeth using the Basic Erosive Wear Examination (BEWE) [7]. The Basic Erosive Wear Examination is a scoring system, which records the most severely affected tooth surface in each sextant. The teeth are divided into sextants: 1-Upper posterior right 2- Upper anterior 3- Upper posterior left 4- Lower posterior left 5- Lower anterior 6- Lower posterior right. Each surface of the teeth is examined to measure the amount of wear using the criteria of grading erosive wear. The scores range from 0 to 3 where ‘0’ is no erosive tooth wear, ‘1’ is initial loss of surface texture, ‘2’ is distinct defect and hard tissue loss <50% of the surface area and ‘3’ is hard tissue loss ≥50% of the surface area. The highest number scored surface is the one recorded for each sextant. The sum of all of these numbers is added with the possible lowest grade being ‘0’ and the highest being ‘18’. Examination was carried by one of the two researchers to avoid inter-examiner errors. The examiner was trained in normal patients before the study in the diagnosis of tooth wear in order to minimize intra-examiner errors. In cases where doubt arose, the mean of three successive readings were taken.
Dentin sensitivity was then checked using the Visual Analog Scale (VAS). The VAS is a psychometric analysis measuring the intensity of feelings and sensations (such as pain) which otherwise, cannot be measured directly [8]. It utilizes a continuous line drawn in plane A4 paper (usually a 10 cm graduated horizontal line) between two clearly defined end-points; one end indicates that there is absence of pain and the other end indicates that the feeling is at its maximum. The participants were then asked to point at the position in the line, which corresponds to what they are feeling at that moment. In this study, the participants were given ice cold water in paper cups at a temperature of 0°C. A thermometer was used to calculate the temperature. The adjusted temperature of the water was obtained by melting ice until 0°C was reached. By using a disposable syringe, 50cc was measured and given to the participants to sip. They were asked to keep the water in their mouth for 20 seconds. Individuals who could not tolerate the ice cold water were asked to spit it back into the cup. The participants were then asked to rate their perception of the pain using the VAS. An average of two readings was taken for each participant.
Statistical Analysis
The data was analyzed by SPSS version 21 (SPSS Inc., Chicago, USA). Independent Student’s t-test and chi-square test were used to correlate the results of parametric and non-parametric data; with a statistical significance difference set as P value <0.05.
Ethical Considerations
The study was approved by the Ethical Committee in the University of Medical Sciences and Technology and permission from the hospital administration was obtained. The purpose of the study was explained to both patients and control group and they were requested to participate voluntary with a signed written informed consent. Those who refused to participate were excluded. Participants with dental complaints were referred and treated for free by one of the investigators.
RESULTS
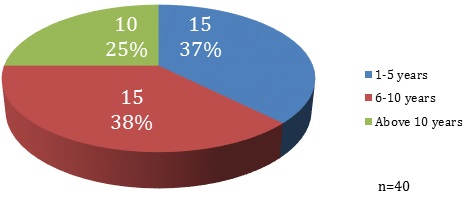
The study consisted of 40 asthmatics (males=15 females=25) and 40 non- asthmatics (males=18 females=22) with a mean age of 40.1±5.1 year for male and 39.8±4.2 year for female. More than half (55%) of the asthmatics were using pressurized metered dose inhaler, 25% were using the dry powder inhaler and 20% used both. Fig. (1) revealed how long the medications were used for. As shown in Table 1 there was no association between the duration of the medication and the severity of dental erosion according BEWE. There was no significant difference between the severity of erosion amongst the males and females as displayed in Table 2. The prevalence of asthmatics having a higher degree of erosion (7-18) was three times that of non-asthmatics as shown in Table 3, however more non-asthmatics had a lower degree of erosion (1-6). According to the means of VAS as displayed in Table 4 there was a significant difference between the dentin hypersensitivity in asthmatics (3.5) and non-asthmatics (1.4), in which the asthmatics had a higher degree of dentin sensitivity. The magnitude of the differences in the means was 2.1 at confidence interval of 95%.
DISCUSSION
The results convened from this study have thoroughly acknowledged the objectives enlisted before carrying out this research. Before proceeding with the interpretation of the findings of this study, it is important to outline the possible limitations. For example, the asthmatics and non-asthmatics were not included randomly from different hospitals; instead, they were selected from the emergency clinic from one hospital in which asthmatics were treated for acute asthma attack. As a consequence, randomization is affected and generalization of the findings is jeopardized. Accompanying co-patients were included in the study as the non-asthmatics control group. Although the mean age of both groups was approximately similar, other confounders may arise like genetic or environmental, which is difficult to control. As a result, internal validity is compromised since there is no way to perceive which factors cause a change. Also due to the small sample size, the sensitivity of the study is too low (type 2 error) and conclusions cannot be withdrawn from the study. Lastly, as tooth wear is a multi-factorial process, it is rather challenging to ascertain whether the resulting dental erosion is due solely to the medications taken or other contributing factors. Regardless of all limitations, the study can be considered as preliminary and the conclusion can be used to carry out further studies to investigate the exact mechanism and association of asthmatic drugs and erosive tooth wear.
| BEWE | Total | |||||
|---|---|---|---|---|---|---|
| 0 | 1-6 | 7-12 | 13-18 | |||
| Duration medication | 1-5 years | 2 | 9 | 4 | 0 | 15 |
| 6-10 years | 0 | 5 | 10 | 0 | 15 | |
| Above 10 years | 2 | 4 | 3 | 1 | 10 | |
| BEWE | Total | |||||
|---|---|---|---|---|---|---|
| 0 | 1-6 | 7-12 | 13-18 | |||
| Gender | Male | 0 | 8 | 7 | 0 | 15 |
| Female | 4 | 10 | 10 | 1 | 25 | |
| Total | 4 | 18 | 17 | 1 | 40 | |
| BEWE | 0 | 1-6 | 7-12 | 13-18 | Total | |
|---|---|---|---|---|---|---|
| Asthmatic | 4 | 18 | 17 | 1 | 40 | |
| Non-Asthmatic | 5 | 29 | 6 | 0 | 40 | |
| N | Mean | Std. Deviation | ||
|---|---|---|---|---|
| Dentin Hypersensitivity | Asthmatic | 40 | 3.5 | 3.0 |
| Non-Asthmatic | 40 | 1.4 | 2.0 |
The effect of inhalation therapy on the oral cavity has garnered lots of attention due to the increase of asthmatics worldwide as mentioned previously. From the aforementioned studies, it has been concluded that inhalers used for the treatment of asthma cause a decrease in salivary flow and change in composition, which in turn decreases the buffering effect of saliva and consequently, decreased protection against dental erosion [9-11]. In addition to decreased salivary flow rate, inhalers which contain β-agonists lead to dilatation of the lower esophageal sphincter which in turn causes gastro-esophageal reflux [12]. Recent studies [13, 14] have linked the relation between gastro-esophageal reflux and dental erosion proving the role asthmatic drugs have in dental erosion.
In the present study, there was a significant variation between the severity of dental erosion in asthmatics and non-asthmatics. More specifically, asthmatics had a higher degree of erosion (moderate and severe) in comparison with non-asthmatics. This is in conjunction with many previous studies, which proved this association [1-3, 15] but contradicted the result of the study carried out by Dugmore et al. [16]. Their study showed that there was no difference in prevalence of dental erosion between asthmatics and non-asthmatics across all degrees of severity. Nevertheless, due to our small sample size, a conclusion cannot be drawn. On the other hand, a higher number of non-asthmatics had lower degrees of erosion similar to the results of other studies carried out in the general population [17, 18].
Our study showed that there was no statistical significance difference between the type of inhaler used and degree of dental erosion. Similarly; Tootla et al. [19] demonstrated no significance difference in drop of plaque pH caused by the MDI and DPI inhalers. This is particularly interesting since there is a difference in pH between the MDI and the DPI where DPI is significantly lower than the MDI [20]. It is expected that the longer medications are taken for, the greater the severity of dental erosion. However, in this study no association was found between the duration the medication was taken for and the severity of dental erosion. A probable clarification for this could be due to the other etiological factors in dental erosion [4]. Despite the exclusion of patients who take medications that are acidic or known to decrease salivary flow, there are other contributing factors, which could predispose to dental erosion. These include lifestyle habits such as the consumption of acidic food or other acidic drinks and the method through which they are consumed [21]. Moreover, those who suffer from gastro-esophageal reflux are also predicted to have worse degrees of erosion and even the severity of the reflux could play a role [13, 14]. On the other hand, protective mechanisms instituted by asthmatics, whether intentional or not, could decrease the severity of the erosion [9]. These include rinsing the mouth after administration of the medication and not brushing the teeth immediately afterwards; drinking water to decrease the dryness of the mouth (side effect of medication); and chewing sugar-free gum to stimulate salivary flow rate. Saliva and its protective components play an important role in the reduction of dental erosion [22]. The composition of saliva and flow from one person to another differs, which could lead to a difference in degree of erosion between individuals.
Additionally, there was no significant difference in the degree of dental erosion between males and females. This is in contrast to a study conducted in Sweden on school children [23] that demonstrated a significant difference between the levels of dental erosion amongst males and females.
Asthmatic patients in this study had a higher rate of dentin sensitivity compared to the non-asthmatics. This finding was not similar to the study carried out by Sivasithamparam et al. where there was no significant difference between both groups. This could be due to the difference of exposure to the protective mechanisms against dentin hypersensitivity [5], which include the use of toothpastes with desensitizing agents. At the same time, the difference in dentin sensitivity could be attributed to other causes such as the presence of other types of tooth wear and gingival recession exposing the root [24].
CONCLUSION
The findings disclosed within this study reveal that there is no association between severity of dental erosion and gender, type of medication taken and the duration medications were taken for by asthmatics. Furthermore, there is a statistically significant difference in the degree of dentin hypersensitivity between asthmatics and non-asthmatics; asthmatics had a higher degree of sensitivity (p-value=0.00), as well as the presence of an association between the use of asthmatic medications and the severity of dental erosion (p-value=0.03), However, due to the small sample size, these results are not conclusive and it is recommended to carry out the study with a larger sample size.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

