All published articles of this journal are available on ScienceDirect.

Alveolar Antral Artery Isolation During Sinus Lift Procedure with the Double Window Technique
Authors Info & Affiliations
Abstract
The sinus lift technique, introduced in 1976 by Tatum and subsequently described by Boyne in 1980, is nowadays considered a safe and reliable procedure for the rehabilitation of the atrophic upper posterior maxilla.
The alveolar antral artery (AAA) is anastomoses between the posterior superior alveolar artery (PSAA) and the infraorbital artery (IOA) and may be present in the sinusal antrostomy. The haemorrhage of this vascular bundle represents the second intra-operatory complication in term of frequency during sinus lift procedure.
Purpose of this study was to illustrate and describe a new technique allowing the AAA isolation during sinus lift procedure in cases in which the artery is clearly present inside the surgical area, detectable through CT scan exam. Presence, course and possible identification of the alveolar antral artery are also discussed, according to the studies present in the literature.
INTRODUCTION
Sinus lift procedure with lateral approach is now a safe and predictable technique for the reconstruction of the atrophic maxilla and the subsequent placement of osseointegrated implants. However, several potential complications may arise during this procedure. The perforation of sinus membrane and interruption of the alveolar-antral vascular bundle are the two most frequent intra-operative complications. The alveolar antral artery (AAA) is an anostomoses between the posterior superior alveolar artery (PSAA) and the infraorbital artery (IOA) and may be present in the sinusal antrostomy sinusal. According to various studies [1, 2] this bundle is always present within the vascular wall of the maxillary sinus but location, diameter and course can vary, as well as the distance from the alveolar ridge that necessarily depend on the amount of maxillary bone atrophy. Knowledge of the vascular supply responsible for perfusion of the maxillary sinus and sinus membrane is therefore essential to avoid bleeding complications.
The maxillary sinus floor elevation increases the maxillary sinus internally. It aims to increase the vertical dimension of the upper jawbone allowing an implant and prosthetic rehabilitation where previously not possible.
This procedure was designed and introduced in 1976 by Tatum in Birmingham, Alabama [3, 4]. The first publication was by Boyne in 1980, followed by the same Tatum [3-5, 6]. The classical sinus lift procedure consists of the preparation of a bone window on the sidewall of the maxillary sinus. This window is separated from the remaining part of the maxillary bone and turned over inside. It lifts with the Schneiderian membrane into a horizontal position, this is consistent with the top of the osteotomy created in the lateral wall of the maxillary sinus. The space created beneath the sinus membrane is filled with grafted material, derived from autologous, heterologous, alloplastic materials or a mixture of these. This ensures sufficient bone height for placement of osseointegrated implants. Implants can be inserted simultaneously with sinus lifting procedure if the height of residual alveolar ridge is no less than 4 mm, otherwise the implant phase need to be performed during a second time, once the graft healing has occurred. The literature listed a number of works on long-term survival of implants placed in the grafted sinus using both the techniques and using different types of grafting material [5-9].
The purpose of this work is to illustrate an innovative, predictable and repeatable technique allowing the AAA isolation during a surgical procedure. It also seeks to avoid emergency due to bleeding complications, especially when this artery represents a vessel of considerable size (>2mm) with a full intra-bone course.
MATERIALS AND METHODS: DESCRIPTION OF A NEW TECHNIQUE
The technique here proposed is a variation of the original as concerned to the window bone design. In the procedure described by Boyne it had a cylindrical shape with rounded corners and sized approximately 10 x 20 mm, with the longest side in the horizontal direction (Fig. 1). The original technique remains the main model and first choice except when there is a need to prevent the progression of a vascular plexus. The alveolar antral artery (AAA) is an anastomoses between the posterior superior alveolar artery (PSAA) and the infraorbital artery (IOA). It has a relapse rate of 100% [1, 10] and its size can vary from<1 mm to more than 2 mm [2, 11]. Its course is horizontal and can be completely intra- bone. This can be done inside the sidewall partly or completely outside of the breastbone, passing between the internal periosteum and the sinus membrane [12]. The ability to identify the alveolar antral artery with a second-level X-ray (CT scan) depends on the set of these factors, namely the vascular lumen of the canal and its position in the intra- or extra-bone. Once identified the AAA (Fig. 2), its position is transferred to the bone wall by using a plastic stant and highlighted by a surgical pencil (Fig. 3). The antrostomy is then performed using the same drill sequence of the classical procedure; starting with a tungsten carbide round bur for the first part of the osteotomy and using then a ball diamond bur for the last phase. The design of the window will take the form of a double window in which the top and bottom are separated by the long course of the AAA. It is left covered in length by the maxillary sinus lateral bone wall (Fig. 4). Once the window is obtained the sinus membrane is detached and the bone graft material is filled inside the cavity following the classic procedure (Fig. 5). The implant placement can be performed at the same time of the sinus grafting or in a second phase, after the healing of the graft. The double windows technique doesn’t cause any kind of modification on the original one or two stage sinus lift protocol as concerned the implant placement (Fig. 6).

Bony window as described by Boyne 1. The dimension of the antrostomy are aproximally 10 mm x 20 mm.
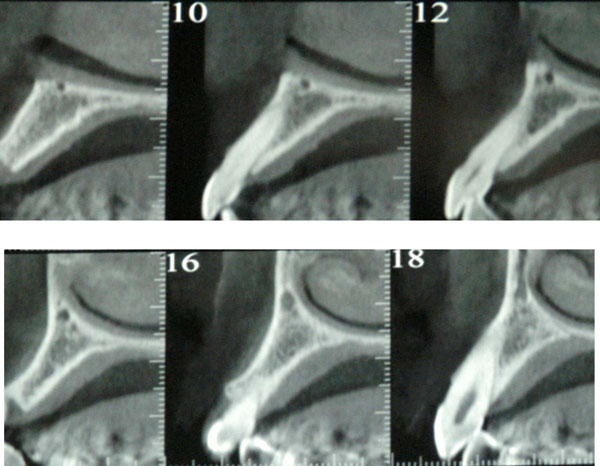
AAA identification through CT scan, cross sections.
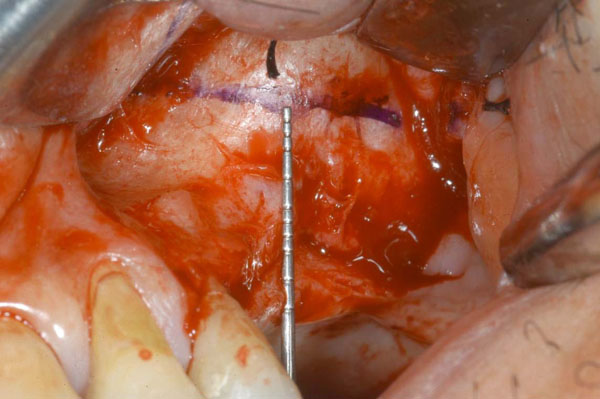
The AAA course is highlined on the lateral wall of the maxillary sinus using a surgical pencil.

Double window design. AAA course remains covered by a bony wall as a protection from possible damages.

Graft material in place surrounding the AAA course.
Implant insertion after 6 months. No complications were reported.

Perforation of the sinusal membrane is the intra-operative complication with the higher frequency.
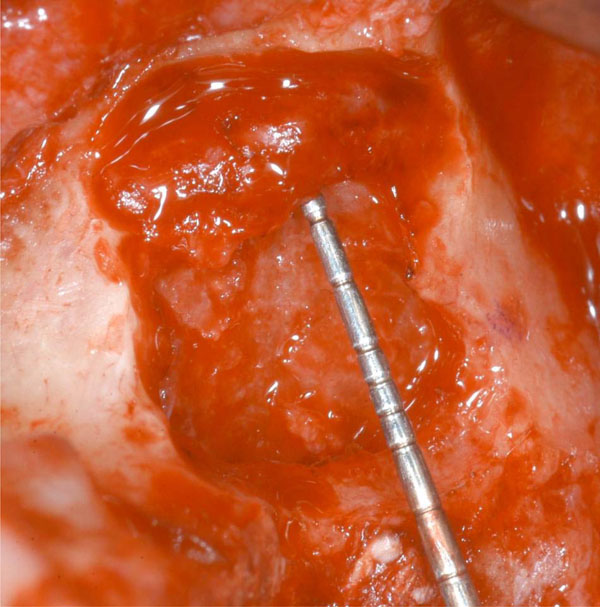

(8 and 9). AAA course in two cases in which the double window technique hasn’t been used. As well seen, the artery is exposed and damages can easily occur.
DISCUSSION
The greatest obstacle to a proper implant and prosthetic rehabilitation is and remains the necessity of adequate bone support, in all its three-dimensional components. Maxillary atrophy, widely spread in the population, caused by periodontal disease, maxillofacial trauma – or by the loss of teeth, constitutes a major obstacle to this type of therapy.
Sinus lift procedure has become a common practice nowadays for oral surgeons and is performed regularly in an outpatient setting for the rehabilitation of the atrophic posterior maxilla. This procedure is well described in literature from a clinical point of view [5, 13-16] with the use of different grafting materials, both autologous [14, 17-20], homologues, derived from alloplastic or a mixture of these [21-27].
The surgeon must be aware of possible complications arising from this type of intervention. These complications can be divided into intra- and post-operative (Table 1). Among the intra-operative complications we identify, in order of frequency, the sinus membrane perforation, the alveolar antral artery haemorrhage, and the obstruction of the antral meatal ostium complex. The post-operative complications can be divided into specific and nonspecific: the specific complications such as sinus congestion, haemoptysis, graft mobility, acute sinusitis induced by the graft, cyst formation and over-filling necrosis are typical of a maxillary sinus lift procedure, those non-specific such as swelling, haematoma, wound dehiscence, the sensitivity of adjacent teeth and increase in temperature are typical of any other oral surgery [25].
Intra- and post-operative complications in terms of frequency during Sinus Lift procedure.
| Intra-operative | Post-operative | ||
|---|---|---|---|
| Specific | Non-specific | ||
| I | Sinusal membrane perforation | Sinus congestion | Swelling and Hematoma |
| II | AAA Hemmorage | Graft mobility | Wound dehiscence |
| III | Antral meatal ostium complex obstruction | Acute sinusitis induced by the graft | Hyposensitivity of adjacent teeth |
| IV | Cyst formation and over-filling necrosis | Increase in temperature | |
AAA detection through CT scan according to its caliper and course.
| Extraosseous | Extra/intraosseous | Intraosseous | |
|---|---|---|---|
| Caliber < 2 mm | 5 | 5 | 5 - ✓ |
| Caliber > 2 mm | 5 | 5 - ✓ | ✓ |
✓: detectable; ✗: non detectable; ✗ - ✓: possible detection
List of possible causes of surgical procedure and graft healing failure following AAA hemmorage.
| Interruption Causes of Sinusal Graft Failure and Surgical Procedure Following AAA Hemmorage | |
|---|---|
| Lengthening of operatory time | Excess in bleeding |
| Inability to proper display in the operative field | Perforation of sinusal membrane |
| Lowest bloody supply to the graft | Graft mobility due to bleeding |
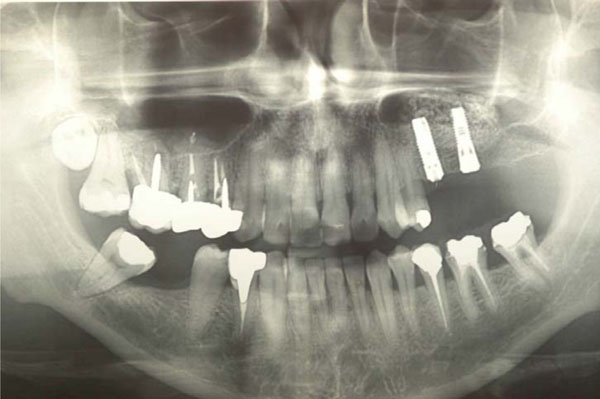
A frequent intra-operative complication is the alveolar-antral artery haemorrhage; second in occurrence, after the perforation of the sinus membrane (Fig. 7). The excision of these intraosseous anastomoses between the upper posterior alveolar and the infraorbital artery should be treated by electrocautery or with bone wax. If not treated, this complication can cause a delayed hemosinus several hours after the end of the surgery when the vasoconstrictor effect of the local anaesthetics is over.
The vascularity of the lateral wall of the maxillary sinus is not standardized and can vary greatly from individual to individual. The vascularisation of the maxillary sinus is in fact guaranteed from the internal maxillary artery, with its four branches: infraorbital artery, sphenoid-palatine artery, posterior superior alveolar artery and descending palatine artery. Posterior-superior alveolar artery has an average size of 2 mm and divides into two branches: the first gum branch runs superficially to the bone wall to supply the premolar and molar area and forms an anostomoses with extraosseous branch infraorbital artery at a distance of 23-26 mm from the alveolar ridge. The second branch, dental, forms an intraosseous anastomoses with infraorbital artery at the level of the anterolateral wall of the maxillary sinus at a distance of 18.9-19.6 mm from the alveolar ridge (Figs. 8-9). It is not always possible to identify this anostomoses, but the terminal branches of IOA and PSAA are always present in the anterolateral wall of the sinus [1] The positions of the extra-and intraosseous anastomoses therefore have a range of variability of 5 to 10 mm which can greatly affect the surgical procedure of the maxillary sinus. This variability depends in most cases by the degree of bone resoption that the alveolar ridge is subject to. In classes I, II and III [26] the literature reports an average distance of the vascular bundle from the most apical point of alveolar ridge of 19 mm [1, 10], and 16.4 mm [2], 16.9 mm [11]. In cases of severe atrophy (in classes IV, V and VI) the distance between the AAA and the crest is greatly reduced. This is shown by the data in the literature, 10.9 mm, 11.25 mm [11, 12].
The design of the bone window required for access to the maxillary sinus may fall within the zone of interest of the intra-bone anostomoses. It may also be farther from that, since the average size of a common antrostomy is about 10 x 20 mm. The higher the degree of bone atrophy is pronounced, the higher is the risk of incurring in the vascular plexus during surgery.
Several studies in the literature agree that the anostomoses between the AASP and IOA is present in 100% of cases but in only 50% or 51.4% of the cases can be identified through pre-surgical CT scan [1, 2, 10-12]. The cause of this contradiction is identified in accordance to Mardinger et al. in diversity in terms of diameter in which the artery can be held. According to their study performed on corpses the body bony canal in which the arterial plexus of AAA passes has a diameter <1 mm in 26% of cases. This is between 1 and 2 mm in 22% of cases and > 2 mm in 7% of cases. The authors argue in their work that CT scan can’t identify a canal with a diameter smaller than 2 mm. In the recent study by Rosano, the authors intend to attribute the inability to detect the AAA during the pre-surgical examination to a different course taken within the sidewall of the maxillary sinus. This may in fact be completely or partially intra-bone and completely extraosseous (i.e. running in between the inner wall of the maxillary sinus and the overlying sinus membrane). In the latter case, the authors report the inability to identify the venous plexus with any type of X-ray examination (Table 2). Both studies, however, agree in the consideration that the damage of an artery with a small calibre (less than 2 mm) clearly does not affect the execution of the surgical procedure. When the vascular bundle is bigger, the lesion may also cause the eventual failure of the intervention. Intra-operatory complications, which can occur to the injury of a vessel of this size are in fact the inability to properly display in the operative field, which can result in perforation of the sinus membrane, the lengthening of the operative time, the interference of the bleeding with the positioning of the graft both during and after surgery, while limiting the stability. Not to mention the lowest blood flow to the grafted area caused by the interruption of the vascular anostomoses may cause a failure in the neo-angiogenesis process within the graft itself (Table 3).
Many cases in the literature discuss about the management of possible bleeding of the AAA, through the use of electrocautery, the use of bone wax, or by vascular ligation of the two parties rescinded. However, few if any work were involved in the search for a technique capable to safely avoid this eventuality in a predictable way.
The technique described in this work is focused on the need, namely the ability to perform a customized procedure based on the location of the anostomoses vessel when it is identified in the pre-operative X-ray. As above described, once identified the course with the help of X-ray examinations as Cone Bean CT, it is essential to design a bone window. This is to take the appearance of a double window in which the separation between the first and second parts of the cave is formed from the bone marrow. This marrow covers the passage of the antral alveolar artery itself that therefore remains protected and not exposed to the work of rotary instruments.
This original procedure is very useful in cases where the vascular bundle of the AAA is large, located wholly or partially within the sidewall of the maxillary sinus bone and can thus be identified by examination radiography. If correctly done this technique allows solving what is the second most common complication, in terms of frequency, while performing a sinus lift procedure with technical side. There is significant evidence from the literature that the failure or incomplete haemostasis in case of bleeding of the antral alveolar artery may lead to the onset of a delayed hemosinus, once the effect of vasoconstrictor contained in the local anaesthesia is finished [28, 29].
As in all clinical procedures, and surgeries in particular, the pre-operative planning assume a direct role in determining the treatment plan and tries to take every precaution to avoid possible complications. The importance that our Department of Implantology has given every day for over ten years in the pre-surgical planning has helped to build and develop this surgical technique. This could be useful in every case the surgeon must operate in this type of anatomical situation.
CONCLUSION
The authors of this work want to underline the importance of proper pre-operative analysis and provide the information to perform a new surgical technique. In specific, when the AAA is clearly present in the interested area, the procedure’s safety and accuracy is enhanced. As widely reported in the literature, the sinus lift procedure with side-view technique is now considered safe and predictable. However, there are possible complications that may occur immediately or after the operation. Injury of alveolar antral vascular plexus is one of these possible complications, and every precaution must be taken to ensure that this doesn’t occur. As demonstrated through this report, a complete planning before doing the sinus lift surgery is mandatory for avoiding intra-operatory complications.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

