All published articles of this journal are available on ScienceDirect.

Meta-Analyses and Orthodontic Evidence-Based Clinical Practice in the 21st Century
Abstract
Introduction:
Aim of this systematic review was to assess the orthodontic related issues which currently provide the best evidence as documented by meta-analyses, by critically evaluating and discussing the methodology used in these studies.
Material and Methods:
Several electronic databases were searched and handsearching was also performed in order to identify the corresponding meta-analyses investigating orthodontic related subjects. In total, 197 studies were retrieved initially. After applying specific inclusion and exclusion criteria, 27 articles were identified as meta-analyses treating orthodontic-related subjects.
Results:
Many of these 27 papers presented sufficient quality and followed appropriate meta-analytic approaches to quantitatively synthesize data and presented adequately supported evidence. However, the methodology used in some of them presented weaknesses, limitations or deficiencies. Consequently, the topics in orthodontics which currently provide the best evidence, include some issues related to Class II or Class III treatment, treatment of transverse problems, external apical root resorption, dental anomalies, such as congenital missing teeth and tooth transposition, frequency of severe occlusal problems, nickel hypersensitivity, obstructive sleep apnea syndrome, and computer-assisted learning in orthodontic education.
Conclusions:
Only a few orthodontic related issues have been so far investigated by means of MAs. In addition, for some of these issues investigated in the corresponding MAs no definite conclusions could be drawn, due to significant methodological deficiencies of these studies. According to this investigation, it can be concluded that at the begin of the 21st century there is evidence for only a few orthodontic related issues as documented by meta-analyses, and more well-conducted high quality research studies are needed to produce strong evidence in order to support evidence-based clinical practice in orthodontics.
INTRODUCTION
During the second half of the last century a large volume of medical literature is published each year progressively, and the clinicians are forced to absorb a large amount of information in order to be able to provide health care efficiently. However, the practitioners do not have the time to read all this available information derived from the thousands of articles published each year. As consequent, during the 1990s, a new process for reviewing scientific evidence emerged in medicine and other health fields, namely "evidence based medicine" (EBM) that relies on systematic approaches to summarize the large volume of literature that health care providers need to integrate into their clinical practice. While the 20th century was considered as the age of science, many researchers and clinicians consider the 21st century as the age of evidence [1].
But what is evidence? According to the Oxford English dictionary the term evidence is defined as "ground for belief; testimony or facts tending to prove or disprove any conclusion" [2]. Consequently, the term EBM can be defined as the process of “systematically finding, appraising and using contemporary research as the basis for clinical practice” [3]. In other words, EBM is "the integration of the best research evidence with clinical expertise and patient values" [4]. Simply stated, EBM is a process that uses systematic approaches to identify the best available research evidence for the optimal treatment intervention for a given patient. This process uses clinical and methodological experts to synthesize all of the available evidence relative to a defined "well-built clinical question". Asking the right question is a difficult skill to learn, yet it is fundamental to the evidence-based decision-making process. This process almost always begins with a patient question or problem. A "well-built" question should include four parts, referred to as PICO that identify the patient, problem or population (P), intervention (I), comparison (C) and outcome(s) (O) [4].
Although this process was originally developed in medicine, its principles apply to all health care fields, including dentistry and orthodontics. Applying EBM principles to dentistry, the American Dental Association (ADA) defined the term "evidence-based dentistry" (EBD) as follows: "EBD is an approach to oral health care that requires the judicious integration of systematic assessments of clinically relevant scientific evidence, relating to the patient's oral and medical condition and history, with the dentist's clinical expertise and the patient's treatment needs and preferences” [5].
The purpose of using an evidence based (EB) approach in clinical care is to close the gap between what is known and what is practiced, and to improve patient care based upon informed decision-making. The use of EB approaches in medicine and dentistry, especially in the beginning of the 21st century, is considered as very significant, since the usually limited human and money resources do not permit to spend money on ineffective treatment procedures. Therefore, the ultimate goal of EB clinical practice is to help health care providers, including orthodontists, to provide the best possible care to their patients by using the best available evidence derived from high quality studies.
The different research designs of the published studies differ with regard to the risk of error and bias in their results. When seeking answers to specific clinical questions, some research methods provide better evidence than that provided by other methods. Thus, the validity of the results of the research studies varies significantly as a consequence of the different methods used in these studies [6]. In order to qualitatively access the evidence produced by the different study designs, hierarchies of evidence have been developed to allow research-based recommendations. These hierarchies are used to grade original studies according to their design, indicating the degree to which different study designs are susceptible to bias [7]. Ranking research designs according to their internal validity not only grades the strength of the evidence, but also provides the end-user of research with a tool to judge the strength of available evidence, indicating the confidence the clinician can have in the corresponding findings [6]. Hierarchies of evidence of the different study designs aim therefore to provide a simple way to communicate a complex range of evidence generated by a variety of research methods. However, the exact format and order of rank for research designs within these hierarchies are still a matter of discussion and existing systems have used a variety of different approaches [6].
Best evidence is a term that according to ADA refers to information obtained from randomized controlled clinical trials (RCTs), non-randomized controlled clinical trials (Non-RCTs), cohort studies, case-control studies, crossover studies, cross-sectional studies, case studies or, in the absence of scientific evidence, the consensus opinion of experts in the appropriate fields of research or clinical practice [5]. Clinical decisions, based on EB conclusions, are made with regard to the strength and quality of the above mentioned various study designs [8, 9]. The hierarchy of evidence of the various study designs based on their strength and quality according to ADA is listed on Table 1 [5].
The Hierarchy of the Level Evidence in Descending Order of the Various Study Designs
| Study Design | Level of Evidence |
|---|---|
| Meta-analyses (MAs) |  |
| Systematic reviews (SRs) | |
| Randomized controlled clinical trials (RCTs) | |
| Non-randomized controlled clinical trials (Non-RCTs) | |
| Cohort studies | |
| Case-control studies | |
| Crossover studies | |
| Cross-sectional studies | |
| Case studies | |
| Consensus opinion of experts | |
| Anecdotal reports or testimonies |
According to the hierarchy of evidence, Systematic reviews (SRs) and meta-analyses (MAs) are considered as providing the highest level of evidence because conclusions are made by combining the results of other types of studies presenting already strong evidence, i.e., RCTs. Systematic reviews are designed to answer specific clinical questions. They employ a predetermined clear and precise methodology to comprehensively search for, select, assess, and analyze original research studies [10]. SRs may or may not include formal meta-analyses [11].
MAs is the statistical pooling of the results of studies that are part of a systematic review [10]. They are statistical procedures that integrate the results of several independent studies considered to be ‘combinable’ [12]. This means that similar measures from comparable studies are listed systematically and the available effect-measures are combined, where possible [13]. The term "meta" implies something occurring later, more comprehensive, and is often used to name a new but related discipline designated to deal critically with the original one [11]. MAs present a significant advantage in relation to SRs: they increase the overall sample size to a great degree by combining the data from individual studies, thus increasing the statistical power of the analysis and the precision to assess the treatment effects. Well-conducted MAs allow a more objective evaluation of the evidence, present a more precise estimate of the treatment effect, and may possibly explain the heterogeneity between the individual studies [11, 14]. Consequently, it can be stated that MAs produce the highest quality of evidence achievable in medicine [15, 16].
However, the different study designs used to produce evidence-based clinical decisions, such as MAs, SRs and RCTs, could result in wrong conclusions when the proper attention is not given and are not conducted in an appropriate manner. Consequently, the integration of the produced evidence into clinical practice can be very challenging for the clinician [17]. As with other study designs, the risks and advantages of MAs are still a matter of discussion in the medical research community [14, 18-24]. The weaknesses of MAs include among others the fact that occasionally the results of a research area are oversimplified, [25] there are errors in classifying of the studies or errors in estimating effect sizes, there is only a small number of well conducted studies to be included in the analysis, the primary studies present low quality or small sample sizes, and the primary data included in the analysis present significant heterogeneity [26].
Therefore, when conducting a MA, the development of a precise protocol to be followed through the whole process is of major importance. This should include: (a) definitions of the response variables, (b) methods of literature searching for the inclusion of the primary data in the analysis, (c) measures to identify and address publication bias, (d) inclusion and exclusion criteria for the articles to be analyzed, (e) data extraction procedure, and (f) statistical analysis of the primary data, including quality and heterogeneity analysis [14].
With an increasing rate of publication of EBM articles in professional journals and an increasing access to electronic literature sources, such as PubMed, the Cochrane Library, etc., clinical decision-making is greatly enhanced year by year. Orthodontic literature uses many forms of evidence, such as RCTs, SRs and MAs. However, MAs investigating orthodontic related subjects are very few in comparison to medical literature. More specifically, the number of published MAs in medical research has increased rapidly during the last decades reaching a total of 21617 articles for the period 1966-2008, while only 43 orthodontic-related MAs have been found to be cited in PubMed for the same period (Fig. 1).
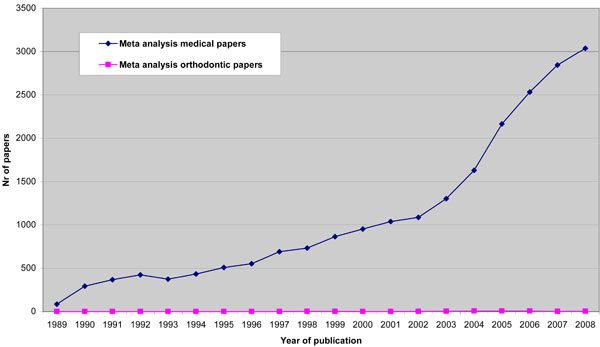
Number of meta-analyses published during the last 20 years (as indexed in Pubmed).
However, it must be mentioned that MAs are quite difficult to perform in orthodontics mainly because (a) there is lack of high quality primary studies to be included in a MAs, such as RCTs, (b) the majority of the primary studies use research designs that are inappropriate for data synthesis [27], and (c) meta-analytical procedures (MAPs) are very complicated and it is questionable if the appropriate statistical approaches have been used by the researchers when conducting MAs. One of the main reasons for the lack of high quality primary studies in orthodontics include the fact that it is ethically close to impossible to perform RCTs with untreated control groups with regards to dental or orthodontic treatment. Control group subjects would also require some kind of treatment, and denying them treatment only for the purpose for a clinical study would infringe upon violating morals and treatment ethics.
Since MAs are considered as studies that provide the best possible evidence when investigating a specific issue, as well as due to the fact that MAs investigating orthodontic related subjects are very few in comparison to medical literature, it was hypothesized that only a few orthodontic topics are supported by strong evidence at the beginning of the 21st century, at least as it is documented by MAs.
Aim therefore of this systematic review was (a) to investigate the topics in the currently existing orthodontic literature which provide the best possible evidence, as documented by MAs, and in addition, (b) to evaluate the methodology used in the published MAs, in order to critically present and discuss their results with the regard to the specific orthodontic subjects that have been investigated so far, as well as (c) to obtain conclusions, which could be applied in evidence-based clinical practice in orthodontics.
MATERIALS AND METHODS
Search Strategy
For the identification of the studies to be considered for inclusion in this SR, detailed search strategies were developed and undertaken for following major electronic databases: MEDLINE (searched via PubMed), EMBASE, Cochrane Database of Systematic Reviews (Cochrane Reviews), Google Scholar Beta, ISI Web of Knowledge (all databases), Scopus, LILACS (searched via Virtual Health Library), Bibliografia Brasileira de Odontologia (searched via Virtual Health Library), Bandolier, Extenza, African Journals Online, Dissertations and Theses (searched via ProQuest), Theses (University of Glaskow), and German National Library of Medicine (ZB MED). These were based upon the search strategy developed for PubMed but revised appropriately for each database to take into account differences in controlled vocabulary and syntax rules. All electronic searches were conducted on July 22, 2009.
The databases searched and the corresponding search strategies per database are presented in detail in Table 2.
The Databases Searched the Search Strategy Used in this Systematic Review (as of July 22, 2009)
| Electronic Databases | Search Strategy (No of Hits Per Database) |
|---|---|
|
MEDLINE searched via PubMed www.ncbi.nlm.nih.gov/sites/entrez/ |
((orthodont*) OR (malocclusion*) OR (functional orthopedic*) OR (crossbite*) OR (openbite*) OR (open bite*) OR (deepbite*) OR (deep bite*) OR (overbite*) OR (prognath*) OR (orthognath*) OR (retrognath*) OR (mandibular deficienc*) OR (mandibular excess) OR (maxillary deficienc*) OR (maxillary excess) OR (growth modification) OR (dentofacial orthopedics) OR (maxillary growth) OR (mandibular growth) OR (molar relationship*) OR (occlusal problem*) OR (occlusal anomal*) OR (occlusal discrepanc*) OR (tooth problem*) OR (tooth anomal*) OR (tooth discrepanc*) OR (vertical excess) OR (vertical deficienc*) OR (tooth movement*) OR (tooth correction*) OR (teeth correction*) OR (tooth alignment*) OR (teeth alignment*) OR (distal movement*) OR (mesial movement*) OR (distalization) OR (mesialization) OR (functional applianc*) OR (removable applianc*) OR (fixed applianc*)) AND (meta-anal*) |
| (119) | |
|
|
|
| EMBASE | meta analys* AND orthodont* |
| www.embase.com | (5) |
|
|
|
| Cochrane Reviews | meta analys* AND orthodont* |
| searched via The Cochrane Library | (35) |
| www.thecochranelibrary.com | |
|
|
|
| Google Scholar Beta | meta analysis orthodontics |
| www.scholar.google.com | Limits: title search |
| (5) | |
|
|
|
| ISI Web of Knowledge | meta analys*) AND (orthodont*) |
| (all databases) | (57) |
| http://apps.isiknowledge.com | |
|
|
|
| Scopus | (meta analys*) AND (orthodont*) |
| www.scopus.com | (79) |
|
|
|
| LILACS & Bibliografia Brasileira de Odontologia | meta analys* AND orthodont* |
| searched via Virtual Health Library | (0) |
| http://www.bvs.br | |
| http://bases.bireme.br/cgi-bin/wxislind.exe/iah/online/ | |
|
|
|
| Bandolier | orthodont* |
| www.medicine.ox.ac.uk/bandolier/ | (0) |
| meta-analys* | |
| (0) | |
|
|
|
| Extenza | orthodontics |
| www.extenza-eps.com | (11) |
| www.atypon-link.com | |
|
|
|
| African Journals Online | orthodont* |
| www.ajol.info | (0) |
| meta-analys* | |
| (0) | |
|
|
|
| Databases of dissertations | |
|
|
|
| Dissertations & Theses | (meta analys*) AND (orthodont*) |
| searched via ProQuest | (2) |
| http://proquest.umi.com/login | |
|
|
|
| Theses (University of Glaskow) | meta analys* |
| http://eleanor.lib.gla.ac.uk/search~S7/ | (2) |
|
|
|
|
German National Library of Medicine (ZB MED) searched via http://opac.zbmed.de/ |
(((Freie Suche = "Metaanalyse" OR Freie Suche = "Metaanalysen" OR Freie Suche = "Metaanalyses" OR Freie Suche = "Metaanalysis" OR Freie Suche = "metaanalytic" OR Freie Suche = "metaanalytical" OR Freie Suche = "Metaanalytische" OR Freie Suche = "metaanalytischen" OR Freie Suche = "metaanalytischer" ) AND ( Freie Suche = "ORTHODONT" OR Freie Suche = "orthodontia" OR Freie Suche = "orthodontic" OR Freie Suche = "orthodontica" OR Freie Suche = "ORTHODONTICS" OR Freie Suche = "Orthodontie" OR Freie Suche = "Orthodontik" OR Freie Suche = "orthodontikē" OR Freie Suche = "orthodontique" OR Freie Suche = "orthodontiques" OR Freie Suche = "orthodontisch" OR Freie Suche = "orthodontischchirurgischen" OR Freie Suche = "Orthodontische" OR Freie Suche = "orthodontischem" OR Freie Suche = "orthodontischen" OR Freie Suche = "orthodontischer" OR Freie Suche = "orthodontisches" OR Freie Suche = "orthodontischstomatologische" OR Freie Suche = "orthodontist" OR Freie Suche = "Orthodontists"))) |
| (0) | |
Following the electronic searching as described above, the reference lists of the initially retrieved articles were handsearched to identify possible additional relevant publications that may have been missed in the database searches.
Databases were searched to include all languages and no language restriction was applied during the whole identification process of the published articles.
Inclusion Criteria
The criteria for considering studies to be included in this SR were the following: (a) the studies should have been indexed as MAs by the corresponding databases, (b) they should have analyzed primary data of the individual articles by means of meta-analytical statistical procedures, and (c) they should have investigated issues related to orthodontics.
Exclusion Criteria
Studies investigating subjects not relevant to orthodontics, as well as articles discussing various aspects of cleft lip and palate, were excluded from this SR.
In addition, SRs, all types of original studies, as well as other types of publications, such as narrative reviews, comments on other articles, short surveys, case reports, protocols, book reviews, letters to the editors, etc., were not included in this evaluation, even if they discussed orthodontic related issues.
Nevertheless, since some confusion still exists in the terminology of SR and MA, and several SRs are indexed in the corresponding databases (or even considered by the writing authors) as MAs and vice versa, the full text of each study initially identified as SRs was examined before its exclusion from current SR, in order to confirm that no MAPs have been used for primary data evaluation.
Selection of Articles
The eligibility of the selected articles was verified firstly by reading the titles and abstracts of the articles initially identified in order to exclude articles discussing subjects not related to orthodontics. Then, comprehensive reading of the full-text of the remaining articles was undertaken by the author of current SR in order to include or exclude articles according to the inclusion and exclusion criteria as described above.
Quality Assessment
Quality assessment is usually applied for the evaluation of primary studies, such as RCTs. However, the quality of studies with other study designs cannot be evaluated in the same way as for randomized controlled trials (RCTs) [28-30]. Various criteria have been suggested to critically appraise their validity, which can be applied to other types of studies; however, a great deal of judgment is necessary [31]. Thus, a quality assessment of the MAs included in this SR was undertaken using the following quality criteria: (a) number of the original studies included in the analysis, (b) electronic databases searched, (c) undertaking of hand-searching, (d) cross-checking of references, (e) inclusion of non-English studies, (f) quality analysis of the original studies, (g) heterogeneity analysis of the primary data, (h) publication bias assessment, and (i) statistical procedures used for primary data analysis.
RESULTS
The flow diagram of the retrieved studies during the selection process is shown in Fig. (2). In detail, following utilization of the above mentioned search strategy, 119 citations were initially retrieved from PubMed, 5 from EMBASE, 61 from Cochrane Database of Systematic Reviews (Cochrane Reviews), 5 from Google Scholar Beta, 57 from ISI Web of Knowledge (all databases), 79 from Scopus, 11 from Extenza, 2 from Dissertations and Theses, and 2 from Theses (University of Glaskow), resulting in a total of 315 citations (Table 2). However, several citations were cumulative entries, i.e., identified in more than one databases, and consequently 191 studies were initially identified through electronic searching. Six additional studies were identified through handsearching of the reference lists of the initially retrieved articles. Thus, a total of 197 studies were initially identified through electronic and handsearching.

Flow diagram of the retrieved studies through the selection process.
After applying the specific inclusion and exclusion criteria, 170 articles were excluded from current evaluation. The number of excluded articles according to the specific exclusion criteria is presented in Table 3, while the excluded articles along with the reason for their exclusion are presented in detail in Appendix I.
Exclusion Criteria and Number of Excluded Articles According to the Reason for their Exclusion
| Exclusion Criteria | Nr of Excluded Articles |
|---|---|
| Subject not relevant to orthodontics | 74 |
| Subject not relevant to orthodontics - Cleft lip and palate | 6 |
| Letter to the editor | 1 |
| Book Reviews | 1 |
| Protocol for a Cochrane review | 1 |
| Report of cases & Systematic review | 1 |
| Short survey | 1 |
| Comments on other articles | 11 |
| Original studies | 19 |
| Narrative reviews | 14 |
| Systematic reviews | 41 |
| Sum | 170 |
Consequently, 27 studies met the inclusion criteria and were considered as MAs appropriate to be included in this SR [32-58].
The quality characteristics of all MAs included in current SR, including their subjects, along with the number of the primary studies included in the analysis, the conducted search strategy, and the corresponding quality analysis, heterogeneity analysis, publication bias assessment and statistical procedures used for primary data analysis are presented in detail in Table 4.
Quality Characteristics of the MAs Included in Current SR, Including their Subjects, Along with the Number of the Primary Studies Included in the Analysis, the Conducted Search Strategy, and the Corresponding Quality Analysis, Heterogeneity Analysis, Publication Bias Assessment and Statistical Procedures Used for Primary Data Analysis
 |
The above 27 MAs have investigated the following subjects:
■ treatment of transverse problems [39-42]
■ incisor intrusion [43]
■ external apical root resorption [44]
■ frequency of occlusal problems [48]
■ nickel hypersensitivity [49]
■ orthodontics and temporomandibular disorders [50,51]
■ obstructive sleep apnea [52, 53]
■ oral hygiene [54]
■ cephalometric analysis [57] and
■ orthodontic education [58]
DISCUSSION
Class II Treatment
Nguyen et al. [32] investigated the risk of traumatic dental injuries of the anterior teeth due to overjet. The authors developed a methodological checklist for observational studies, in order to qualitatively assess the 11 articles that were finally included in the analysis. The relative risk of overjet compared with a reference was expressed as odds ratios (ORs). For each primary study, the ORs and their 95% confidence intervals (CIs) were computed and subsequently these ORs were pooled across the studies. Finally, the influence of the quality of the studies on the pooled OR was addressed. According to this evaluation, the authors concluded that: (a) children with an overjet larger than 3 mm are approximately twice as much at risk of traumatic dental injury on anterior teeth than children with an overjet less than 3 mm, (b) the effect of overjet on the risk of dental injury is less in boys than in girls of the same overjet group, and (c) the risk of anterior teeth injuries tends to increase with increasing overjet size. Regarding the MAPs used in this study, and despite the fact that a possibility of publication-bias cannot be excluded, some additional shortcomings include the following: (a) The studies selected for the metaanalysis showed heterogeneity of the outcomes, with exception of the subgroup between the ages 6 to 18. (b) There was no reference to the number of the control group size for any of the primary studies. (c) No information was given if studies in other language than English were included in the analysis. To conclude, although this MA was performed adequately well, the above mentioned conclusions should be considered with some caution due to the limitations of the source studies and the heterogeneity of the primary data implemented in the analysis.
The effect of functional appliances on the skeletal pattern following orthodontic treatment of patients with Class II, division I malocclusion was the subject of a MA performed by Mills [33]. The author reviewed the cephalometric findings of 26 papers investigating the Andresen-activator and Frankel appliances. In order to increase statistical significance, the findings of the primary studies were combined to produce larger samples, and they were also compared with a control group derived from reports of untreated Class II, division 1 individuals. For this purpose, the author combined the means and the given standard deviations of the primary studies using the student’s t-test for the full figures and the Mann-Whitney U-test for the annual measurements and concluded that: (a) there was no appreciable restraining effect on the forward growth of the maxilla in either of the groups (functional appliances group and control group); (b) a slight mean increase in mandibular growth could be observed, mainly in a vertical direction; (c) no change in the position of the glenoid fossa was evident; and (d) there was a wide individual response and average changes were rarely observed in a patient. Although there was no language bias, no multiple publication bias and no citation bias, the MAPs applied in this study presented the following problems: (a) No search strategy was developed and no searching of the electronic databases was performed. The literature search was incomplete including only papers from American, European and Scandinavian literature, and thus, additional studies may exist that were not included in the MA. (b) No special designed tests for MAs were used; instead, statistical tests designed for primary data analysis (student’s t-test and Mann-Whitney U-test) were used, even though some primary studies did not report standard deviations! (c) There was lack of quality and heterogeneity analysis as well as of assessment of publication bias. (d) The treatment duration of the patients included in the primary studies was different, while the control group was consisted of cases with rather milder symptoms, facts that are associated with selection bias. Consequently, this MA can not be considered as appropriately conducted. Thus, the corresponding conclusions are not supported with strong evidence and they should not be taken onto consideration.
Chen et al. [34] investigated the efficacy of functional appliances on mandibular growth in patients with Class II malocclusion, aiming to test the hypothesis that functional appliances enhance mandibular growth. The data of 6 articles meeting validity standards were evaluated for 12 cephalometric variables using ANOVA, students t-test for paired data, and 95% CIs. Only the variables Ar-Pg and Ar-Gn differed significantly between the treated and control groups. Weaknesses of the methodology used in this MA include the following: (a) The lack of searching databases additionally to MEDLINE. (b) Only English language papers were evaluated (language bias); (c) The use of statistical tests designed for primary data analysis (student’s t-test, ANOVA). (d) No control and treated group sizes were mentioned in the text (although the results of the analysis were given in box plots). (e) The age of patients at the start of the treatment as well as the treatment duration was different in the primary studies (selection bias). Consequently, no definite conclusions concerning the efficacy of functional appliances on mandibular growth could be reached. This could be attributed to the inconsistencies in the cephalometric variables of the primary studies measuring treatment outcome, as well as to the different treatment durations of the various patient samples.
More recently, Antonarakis and Kiliaridis [35] evaluated the anteroposterior short-term skeletal and dental effects in growing patients with Class II malocclusion following treatment with functional appliances, extraoral traction, or combination appliances. They assessed the primary data of 9 studies which investigated changes referring to maxilla (as expressed by the SNA angle), mandible (as expressed by the SNB angle), intermaxillary relationships (as expressed by the ANB angle), and to the amount of overjet after annualizing the corresponding results due to the different treatment duration observed in the various groups. For the statistical analysis they used the random-effects model to calculate the weighted mean differences (WMDs), while forest plots were drawn to graphically present their results. Heterogeneity analysis was performed by means of chi-square tests and I2 statistic. The authors concluded that: (a) Functional and extraoral traction appliances used for the treatment of Class II malocclusion in growing patients are associated with an improvement of the sagittal intermaxillary relationship. (b) Activators, twin block and combination appliances are acting mainly on the mandible, while twin block appliances also have a significant effect on maxillary growth. (c) Extraoral appliances are acting mainly on the maxilla. (c) All appliances under investigation except extraoral traction revealed a large decrease of the overjet. Although the literature search was performed adequately well (however, no information is given if non-English papers were also included) and a quality analysis of the included studies was undertaken, the methodology followed by the authors present some drawbacks. In detail, one of the studies involved patients with Juvenile Rheumatoid Arthritis (JRA), and in two studies there was no blind allocation for patients selected for the treated and the control groups. Further, the authors excluded papers investigating Herbst appliance treatment, although Herbst appliances are in general considered as functional (despite the fact that they are fixed) [59]. The data of these studies might have been used for sub-group analysis and comparison with the other treatment approaches under investigation. It is not rational to include in a MA a group of patients suffering from JRA, presenting specific craniofacial characteristics [60,61] and combine their data with data derived from conventional orthodontic patients and at the same time to exclude a treatment modality (Herbst appliance) that belongs to the subjects of the specific investigation. Finally, no assessment of publication bias was performed. To conclude, the results of this investigation should be treated with some caution.
At the same time period, Harrison and colleagues [36] assessed the effectiveness of orthodontic treatment of 7 to 9 years old children and adolescents presenting prominent upper front teeth. Following implementation of specific inclusion and exclusion criteria, 8 trials involving data from 592 individuals were included in the analysis. Initially, a quality analysis of the included studies was undertaken. Statistical analysis was performed as following: For dichotomous outcomes, the estimates of effect of an intervention were expressed as ORs together with their 95% CIs. For continuous outcomes, the mean differences and standard deviations were used to summarize the data for each group. Further, using the random-effects models, the ORs were combined for dichotomous data, and the mean differences for continuous data. Heterogeneity analysis was also performed by means of Cochran’s test for heterogeneity and the I2 statistic. The authors concluded that: (a) early orthodontic treatment, followed by a later phase of treatment when the patient is in early adolescence, does not appear to have any advantages over one-phase treatment in early adolescence, (b) when treatment with functional appliances is provided, there a minor skeletal changes, probably not clinically significant, and (c) the use of functional appliances does not seem more effective than twin blocks. The methodology followed by the authors present no shortcomings and therefore the corresponding conclusions are supported with strong evidence. Thus, they can be seriously taken into consideration when planning orthodontic treatment of children or adolescents presenting prominent upper front teeth.
Class III Treatment
Kim et al. [37] evaluated the effectiveness of maxillary protraction with orthopedic appliances in patients with Class III malocclusion, aiming additionally to determine a consensus for controversial issues such as treatment timing and use of adjunctive intraoral appliances. Fourteen studies met the selection criteria and included in the analysis. In order to combine the primary data, the means and standard deviations of the original articles were summarized and the corresponding results were graphically represented. The statistical analysis of the changes following treatment, as measured by selected cephalometric landmarks, showed no distinct differences between palatal expansion and non-expansion group, except for one variable. Further, examination of the effect of age revealed greater treatment changes in the younger group of patients. These results indicated that (a) protraction face mask therapy is effective in patients who are growing, but to a lesser degree in patients who are older than 10 years of age, and (b) protraction in combination with an initial period of expansion may provide more significant skeletal effects. Although no language bias was evident, this MA was associated with the following drawbacks that weaken the provided evidence: (a) The authors used statistical tests for primary data analysis and not specially designed tests for MAs. (b) The literature search was limited only to a MEDLINE search and no other databases were examined. (c) An ethnic maturation differential may exist in the primary studies. (d) There was lack of a matched control group. (e) There was lack of standardization of the design of the primary studies. (f) No heterogeneity analysis and no quality assessment of the included studies were undertaken. Consequently, the results of this MA cannot be considered that are supported with strong evidence.
Maxillary protraction treatment was also the subject of a MA performed by Jager et al. [38] aiming to quantitatively review the published results concerning the treatment effects of maxillary protraction on craniofacial growth of patients presenting Class III malocclusion. After applying specific inclusion criteria, 12 studies remained for further evaluation. In order to combine the data of the primary studies, the results of various cephalometric measurements were reviewed using the Dstat 1.10 software by calculating a standardized treatment effect variable. The homogeneity of the variances of the different effect variables was evaluated and a composite effect was calculated. According to the results of this investigation, a significant composite effect of the maxillary protraction treatment on some craniofacial skeletal and dental components was evident. However, several of the individual effect variables demonstrated a significant lack of homogeneity. Study characteristics which might possibly account for this variability were the age of the patients at treatment start and the combination of maxillary protraction with rapid maxillary expansion. With regard to the statistical procedures used, the fact that a specially designed test for MA was performed adds to the strengths of this study, while the limitation of literature searching in only one database (MEDLINE) without any information regarding the non-English studies, as well as the lack of assessment of publication bias weaken the power of the analysis.
Treatment of Transverse Problems
The subject of the MA performed by Burke and colleagues [39] was the evaluation of the changes of mandibular intercanine width during and after treatment and post-retention. Twenty six studies that assessed the longitudinal stability of post-retention mandibular intercanine width were evaluated. For the statistical analysis, weighted averages and standard deviations for the means were compared for linear changes in intercanine transverse dimensions during treatment (T1), immediately after treatment (T2), and after removal of all retention (T3). Paired two-tail t-tests were performed between T3 and T1 means on all groups and 95% CIs were computed. The authors concluded that: (a) Regardless of patient diagnostic and treatment modalities or whether treatment was extraction or non-extraction, mandibular intercanine width tends to increase during treatment about 1-2 mm, to decrease post-retention to approximately the original dimension, and to show a net change after post-retention between +0.5 to -0.6 mm. (b) While statistically significant differences could be demonstrated within various groups, the magnitudes of these differences were not considered clinically important. (c) The net change in mandibular intercanine width that was approximately zero, which supports the concept of maintenance of the initial intercanine width in orthodontic treatment. Regarding the methodology used, the following issues should be mentioned: (a) The authors used statistical tests for primary data analysis and not specially designed tests for MAs. (b) No control group size was mentioned. (c) The literature search was limited only to a MEDLINE search and no other databases were investigated. (d) The post-retention period varied from 4 months to 12 years. (e) Quality and heterogeneity analysis as well as assessment of publication bias of the included studies were not performed. Consequently, the results of this MA are not well supported by the methodology used and they should be considered with caution.
Schiffman and Tuncay [40] evaluated the existing literature on maxillary expansion in 2001 in order to understand the appropriateness and stability of this treatment approach. The assessment of the primary data was performed by coding and scoring each study with respect to pre-established characteristics. Following this evaluation, only 6 studies remained for the final analysis. An overall effect size was computed and aspects of study design were analyzed. The results of this investigation were the following: (a) The mean expansion after appropriate adjustment was 6 mm (±1.3 mm). Of the 6 mm average, 4.9 mm was retained while wearing retainers; (b) The 6 mm average expansion with retention yielded a 4.7 mm residual expansion, which subsequently was reduced to 3.9 mm during the short-term post-retention period. (c) In the long-term post-retention period, only 2.4 mm of the residual expansion remained, which was no greater than what is documented as normal growth. The authors concluded that there was inadequate evidence to support the opinion that the expansion achieved beyond of what is expected due to normal development of the maxilla could be retained in the long term. The methodology used in this study, includes the following shortcomings: (a) The literature search was performed in only one electronic database (MEDLINE), no other databases were investigated, and this search was conducted only for the period from 1979 to 1999. (b) There was a language restriction, since only English language publications were included in the MA. (c) The authors did not present any P-values for the measurements given in their analysis. (d) The lack of uniformity of the included primary studies and their improper study design, which did not permit an appropriate statistical analysis. (e) The lack of a detailed analysis of heterogeneity. To conclude, due to these weaknesses the revealed evidence should be regarded with some caution.
Harrison and Ashby [41] performed a MA aiming to evaluate orthodontic treatment procedures used to expand the maxillary dentition and correct posterior crossbites. For the statistical analysis of the 13 primary studies, the ORs, relative risk, relative risk reduction, absolute risk reduction, and the corresponding 95% CIs, were calculated for event data while the WMDs and 95% CIs were calculated for continuous data. The authors also conducted a quality analysis of the included studies. The conclusions of this MA were: (a) Occlusal grinding in the primary dentition, with or without the addition of an upper removable expansion plate, is effective in preventing a posterior crossbite from being perpetuated to the mixed and permanent dentition. This is however only based on data derived from two studies with small sample sizes. (b) No evidence of a difference in treatment effect, as documented by molar or canine expansion, between the test and control intervention was found in the trials which compared banded vs. bonded and two point vs. four point rapid maxillary expansion, banded vs. bonded slow maxillary expansion, transpalatal arch with or without buccal root torque, or upper removable expansion appliance vs. quad-helix. (c) Not adequate data were provided regarding two point vs. four point rapid maxillary expansion to permit an appropriate analysis. Although the procedures used in this study were according to the guidelines for performing MAs, [14] almost all primary trials included in the analysis presented small sample sizes, a fact that weakens in a way the evidence produced by this MA. Therefore, as the authors also concluded, further studies with appropriate sample sizes are needed to assess the effectiveness of the above interventions.
More recently, Lagravère and colleagues [42] performed a MA of the immediate transverse, anteroposterior, and vertical dental and skeletal changes following orthodontic treatment with rapid maxillary expansion. Fourteen articles satisfying the final inclusion criteria, though with methodological deficiencies, were included in the analysis by calculating of effect size estimates and their corresponding 95% CIs using the fixed-effects model for homogeneous data and the random-effects model for heterogeneous data. The authors concluded that (a) the greatest changes immediately after rapid maxillary expansion were observed in the maxillary transverse plane. (b) Maxillary width increase was due to dental expansion rather than true skeletal expansion. (c) Only few vertical and anteroposterior changes were statistically significant, and none of them was clinically significant. The drawbacks of this MA include the following: (a) The authors made a great effort by searching a large number of electronic databases and checking also the reference lists of the selected articles in order to identify all published studies dealing with rapid maxillary expansion, excluding however non-English published studies. (b) Although a quality analysis of the included papers was undertaken, no heterogeneity analysis and assessment of publication bias was performed. (c) All of the original studies presented methodological deficiencies. Consequently, the results of this investigation should be considered with some caution.
Incisor Intrusion
The quantification of the amount of true incisor intrusion attained during orthodontic treatment was the subject of another MA performed by Ng et al. [43] Two studies were included in the analysis. The fixed-effects model was used to evaluate the amount of incisor intrusion attained by means of the segmented arch technique (SAT). The results indicated that true incisor intrusion was feasible in both arches using the SAT. Using the SAT a 1.5 mm of maxillary incisor intrusion and 1.9 mm of mandibular incisor intrusion could be achieved when applied in non-growing patients. However, the clinical significance of the amount of true intrusion as an exclusive treatment option was questionable for patients presenting severe deep bite. Regarding the methodology used, the very small number (n=2) of the source studies evaluated in this MA which additionally included only adult patients, the small sample sizes, as well as the lack of heterogeneity analysis and assessment of publication bias of the included studies weaken the power of this investigation. Therefore, the extrapolation of the observed values to younger populations appears to be questionable and the overall results of this MA should be viewed with caution.
External Apical Root Resorption
The treatment-related factors of external apical root resorption were also among the subjects recently investigated by Segal et al. [44] Clinical trials in English language with a sample size more than 10 individuals that received orthodontic treatment with fixed appliances, with available pre- and post-operative radiographs, and measurements of external apical root resorption mainly of the maxillary incisors were included in this study. Studies including samples with history of trauma, prior root resorption or endodontic treatment were excluded. In order to access the methodological soundness for each individual study, coding variables were determined along with a grading system and a cumulative "meta-analysis factor" was computed for each study. In addition, appropriateness of these selections and absence of publication bias was tested by a "funnel plot" analysis. Eight articles met the inclusion criteria and further evaluated in this MA. After calculating the weighted means of correlations between the variables, the authors found that apical tooth resorption was highly correlated with total apical displacement (r=0.822) and treatment duration (r=0.852) and concluded that treatment-related causes of external apical root resorption seem to be the total distance the apex had moved and the time it took. Consequently, factors that are associated with the duration of active treatment might result in increased levels of apical root resorption in a pre-disposed individual. Regarding the power of the statistical procedure, the limitation of searching in only one database, the restriction of articles published only in English language (suggesting database or language bias, respectively), as well as the lack of a heterogeneity analysis weaken the overall results of this MA.
Dental Anomalies
The prevalence of dental agenesis of the permanent teeth was the subject of a MA performed by Polder et al. [45]. Multiple regression-analysis (weighted least squares) was performed using date from 28 primary studies in order to evaluate the possible influence of chronological age, sample size, continent and year of publication. The prevalence of agenesis per tooth type, affected patients and number of missing teeth per patient was calculated, as far as it was reported in the corresponding papers. The relative risk was also calculated for the comparison of the prevalence between males and females. Following this evaluation the authors concluded the following: (a) The prevalence of dental agenesis differs in relation to continent and gender: for both sexes was higher in Europe (males 4.6%; females 6.3%) and Australia (males 5.5%; females 7.6%) than in North American Caucasians (males 3.2%; females 4.6%), while in females it was 1.37 times higher than in males for all three continents examined. (b) The mandibular second premolars were affected most frequently, followed by the maxillary lateral incisors and maxillary second premolars. (c) Bilateral agenesis of the maxillary lateral incisors was more frequent than the unilateral agenesis, while the opposite was found for the mandibular and maxillary second premolars, and the maxillary first premolars. Regarding the MAPs used in this study, although the consideration of possible bias (by evaluating the influence of chronological age, sample size, continent and year of publication) add to the value of this investigation, the lack of quality and heterogeneity analysis of the original studies included in the analysis weaken in a way the power of the analysis. Thus, the corresponding results should be regarded with some caution.
Most recently, the author of this paper along with colleagues [46] assessed the characteristic features and dental anomalies that may accompany tooth transposition. The literature search included several electronic databases, while cross-checking of the reference lists of the included articles was also performed. After applying specific exclusion criteria, 5 studies were found eligible to be included in the analysis. Meta-analysis was performed by determining the marginal mean proportions and the 95% CIs estimated by the random-effects model. Quality analysis of the included studies was undertaken, as well as evaluation of heterogeneity, which it was performed using the Q and the I2 statistic. After noting the lack of high-validity studies investigating the characteristic features and dental anomalies of tooth transposition the authors found that tooth transposition is significantly unrelated to dental anomalies, such as congenitally missing teeth, peg-shaped or hypoplastic teeth, and impacted teeth, while there might be an association with over-retained deciduous teeth. They therefore concluded that tooth transposition can be regarded as an isolated phenomenon rather than a syndrome, while occasionally it can be accompanied by some characteristic features and dental anomalies, but without distinct associations. The methodology followed by the authors present no shortcomings, since several electronic databases were searched, cross-checking of the reference lists was performed, no language restriction was applied during the selection process, quality analysis of the included studies and assessment of heterogeneity of data was performed, and appropriate statistical procedures were applied. Thus, it can be considered that the results of this investigation are supported with strong evidence.
A further MAs performed again by the author of this paper and colleagues aiming to synthesize currently existing data and to investigate the prevalence of tooth transposition as well as its relation to gender, dental arch, and quadrant occurrence [47]. Several electronic databases were searched, while cross-checking of the reference lists was also performed in order to identify the potentially relevant studies. After applying specific inclusion and exclusion criteria, 9 studies were included in this evaluation. Quality analysis of the included studies was undertaken, as well as heterogeneity analysis of the primary data by means of the Q and I2 statistic. In addition, Publication bias was also assessed by funnel plot analysis. Meta-analysis was performed by determining the event rate and the 95% CIs estimated by the random-effects model and the results were presented by means of forest plots. The analysis of the data of the primary studies revealed that (a) tooth transposition has a mean prevalence of 0.33%, (b) this prevalence seems to be similar between the two genders, and (c) tooth transposition appears more frequently in the maxilla than in the mandible and more unilaterally than bilaterally. As in the previous study mentioned above, the methodology followed by the authors including searching of several electronic databases along with cross-checking of the reference lists of the included articles and the absence of language restriction, quality analysis of the included studies, assessment of heterogeneity, and appropriate meta-analytic statistical procedures, strengthen significantly the power of the analysis and they strongly support the derived evidence.
Frequency of Severe Occlusal Problems
Frazao et al. [48] investigated the prevalence and severity of occlusal problems in populations with deciduous and permanent dentition. The authors evaluated the primary data of 7 articles by calculating the weighted ORs and their corresponding 95% CIs using the fixed-effects model, after checking data heterogeneity by means of the chi-square test with Yates correction. The statistical analysis revealed that (a) the prevalence of occlusal problems was found almost twice as large in patients with permanent than in deciduous dentition (71.3% and 49.0%, respectively), and (b) among the variables under evaluation (including sex, type of school and ethnic group), only the developmental stage of the dentition was significantly associated to the severity of malocclusion. Regarding the statistical methodology used for the analysis of the primary data, although the authors used appropriate meta-analytic approaches, the absence of a quality analysis and of the assessment of publication bias weaken in a degree the evidence produced by this MA.
Nickel Hypersensitivity
Kolokitha and colleagues [49] performed a MA in order to investigate the effect of orthodontic therapy on the prevalence of nickel hypersensitivity and compare it with the prevalence in the general population. Several electronic databases were searched and cross-checking of the reference lists of the articles was also performed. After applying specific inclusion criteria, 8 studies were eligible for the meta-analysis. For the studies reporting prevalence of Ni hypersensitivity before and after orthodontic treatment, the OR of a positive Ni patch test prior to orthodontic treatment to a positive Ni patch test after the placement of orthodontic appliances and the corresponding 95% CIs were calculated, while for the studies reporting the prevalence of Ni hypersensitivity only after placement or removal of orthodontic appliances, and in the general population, the relevant event rates were computed. Further, the random-effects model was used to combine the ORs before and after orthodontic treatment. In addition, evaluation of the validity of the included articles and funnel plot analysis for the evaluation of publication bias were performed, while the Cochran test for homogeneity and the I2 test were also calculated to check for heterogeneity and inconsistency, respectively. The results of this analysis indicated that: (a) There is lack of high-validity longitudinal studies of the prevalence of nickel hypersensitivity in patients before and after orthodontic treatment and in appropriate controls. (b) No statistically significant difference between the odds for a positive patch-test result before orthodontic treatment and after the placement of the appliances was observed. (c) Orthodontic patients with no cutaneous piercing or with skin pierced have no statistically significant differences of nickel hypersensitivity after treatment compared with the general population. Consequently the authors concluded that orthodontic treatment is not associated with an increase in the prevalence of nickel hypersensitivity unless subjects have a history of cutaneous piercing. The methodology followed in this MA resulted in strong evidence, since several electronic databases were searched, cross-checking of the reference lists was performed, no language restriction was applied during the selection process, quality analysis of the included studies and assessment of publication bias and of heterogeneity was performed, as well as appropriate statistical procedures were applied.
Orthodontics and Temporomandibular Disorders
The subject of the MA conducted by Kim et al. [50] was the investigation of the relationships between orthodontic treatment and temporomandibular disorders (TMDs) in orthodontic patients following completion of their treatment. Data was extracted from 31 articles and was divided according to the study designs, and TMD symptoms, signs, or indexes. To test whether all primary studies attempted to estimate or observed the same true effect, and whether variability between results of the studies was due to random error only, a statistical test for the hypothesis of parametric homogeneity was conducted. In addition, probabilities of homogeneity and odds on parametric homogeneity were calculated. Due to the extreme heterogeneity of the data of the primary studies, it was not possible to complete the statistical analysis. Thus, a definitive statement concerning the relationships between orthodontic treatment and TMDs could not be concluded. However, although it was not possible to perform a "true" (in other words, a complete) MA, the authors followed, at least during the initial stages an appropriate meta-analytic approach. Despite the extreme heterogeneity of the data of the primary studies, the following issues weaken even more the results of this investigation: (a) Only one electronic database was investigated. (b) Only English language papers were taken into consideration. (c) Not all the primary studies included were of the same quality. (d) Inclusion of studies regardless the age of the patients. (e) Large number of different types of appliances. (f) Different treatment durations of the patient samples. (f) Lack of assessment of the quality and publication bias of the original studies included in the analysis. To summarize, this MA do not provide any evidence concerning the relationships between TMDs and orthodontic treatment.
Macedo et al. [51] performed a MA to evaluate the effectiveness of occlusal splints for the treatment of sleep bruxism with alternative interventions, placebo or no treatment. Among the 32 potentially relevant clinical trials initially identified, only 5 RCTs satisfied the inclusion criteria and were selected for further analysis. In these trials occlusal splint treatment was compared to treatment with palatal splints, mandibular advancement devices, transcutaneous electric nerve stimulation, and no treatment at all. However, the methodological quality of the five trials included was low. In detail, none of the studies gave a clear description of the concealment of allocation and only one study described how the allocation sequence was generated, some inclusion criteria were not specified by the authors, and other outcomes could not be analyzed because they were inappropriately described. In addition, just one outcome (arousal index) was common and it was combined in a meta-analysis which was performed using the random-effects model. For dichotomous outcomes, the estimate of effect of an intervention was expressed as risk ratios together with the corresponding 95% CIs. For continuous outcomes, WMDs to compare groups and standard deviations were used to summarize the data for each group. In addition, quality analysis of the included studies was performed, and heterogeneity analysis was undertaken using the Cochran’s test for heterogeneity and the I2 statistic. The results of the MA indicated that no statistically significant differences between the occlusal splint treatment and the control groups were found. Therefore, there is not sufficient evidence to support the effectives of the use of occlusal splints for the treatment of sleep bruxism with regard to sleep outcomes, but their use might be beneficial with regard to tooth wear.
Obstructive Sleep Apnea Syndrome
The subject of the MA conducted by Miles et al. [52] was the investigation of possible significant differences between the cephalometric variables describing the craniofacial skeletal or soft tissue morphology of individuals with and without obstructive sleep apnea syndrome (OSAS). A hierarchical analysis was conducted to examine the quality of evidence within the studies included in the analysis. The MAPs employed in this study included combined means and standard deviations for the OSAS and control groups for effect size plots in order to examine the distribution and consistency of outcomes across studies, Z-scores for statistical significance testing between groups, and receiver operating characteristic (ROC) curves. Following this evaluation the authors concluded that: (a) The literature is characterized by several methodological deficiencies and therefore is equivocal regarding a causal association between craniofacial structure and OSAS. (b) Evidence for a direct causal relationship between craniofacial structure and OSAS is unsupported by the literature, both qualitatively and quantitatively. (c) The rationale for OSAS treatments based on morphologic criteria remain unsubstantiated. (d) The two most consistent strong effect sizes with the highest potential diagnostic accuracies presented the variables related to mandibular structure (Sn/MPA, Go-Gn). (e) Although mandibular body length (Go-Gn) appears to be an associated factor, this does not support causality. (f) More standardization of research methods and data presentation is required. Regarding the methodology used, only one sample study and none of the efficacy treatment studies met all the quality criteria for inclusion in the analysis, as set by the authors. However, MA was performed in the examined variables by including data from studies with control samples and for each variable, data from different number of studies was included in the MA (i.e., for Go-Gn, measurements from 3 studies were combined). Further, although no publication biases were present, the studies included in the analysis were limited to those published in English language and no heterogeneity analysis of the primary data was undertaken. Consequently, it can be stated that the MAPs followed by the authors did not result in strong evidence.
Lim et al. [53] performed a MA in order to determine the clinical effectiveness of oral appliances in the treatment of obstructive sleep apnoea-hypopnoea (OSAH) syndrome in adults. After applying specific inclusion criteria, 17 studies (involving 831 participants) found to be eligible and they were included in the analysis. The quality assessment revealed that all the original studies included in the analysis presented some shortcomings, such as small sample size, underreporting of methods and data, and lack of blinding. For continuous variables, the authors calculated the results of the individual studies using a fixed-effect WMD or a standardized mean difference (SMD) with the corresponding 95% CIs. For dichotomous variables, a fixed-effect OR with the corresponding 95% CIs were calculated. Heterogeneity was assessed using the Breslow-Day's test, the Chi-square test and the I2 statistic. When heterogeneity was present, the random-effects model was used to calculate the results. According to the results of this MA the authors concluded that: (a) There is increasing evidence suggesting that oral appliances improve subjective sleepiness and sleep disordered breathing compared with a control. (b) Nasal continuous positive airway pressure (CPAP) therapy appears to be more effective in improving sleep disordered breathing than oral appliances. (c) Although more evidence is needed to further support the results of this investigation, it may be more appropriate to recommend oral appliances treatment to patients with mild symptomatic OSAH, as well as to those patients who are unwilling or unable to tolerate CPAP therapy. Although the evidence produced by this investigation with regard to the appropriate meta-analytic approaches followed by the authors revealed as strong enough to support the use of CPAP therapy in patients with OSAH syndrome, its relative effects compared with oral appliances treatment require further elucidation, since the currently existing trials present a number of shortcomings.
Oral Hygiene
Kaklamanos and Kalfas [54] performed a MA in order to meta-analysis was to compare the effectiveness of powered and manual toothbrushes in reducing gingival inflammation in patients treated with fixed orthodontic appliances. After applying specific inclusion criteria concerning study design, participants’ characteristics, intervention characteristics, and principal outcome measures, 5 trials were considered appropriate to be included in the meta-analysis. The WMD with the corresponding 95% CI was used to express the comparative treatment effect, while the random-effects model was used to combine treatment effects across the studies in each category. The quality of the included trials was evaluated by assessing randomization, allocation concealment, blinding, and handling losses using the Cochran test for homogeneity and the I2 statistic. Based on quality assessment and the short experimental period of the 5 trials included in the analysis, and following appropriate meta-analytic procedures the authors concluded that current evidence is insufficient to support the comparative efficacy of powered toothbrushes in reducing gingivitis in patients undergoing fixed orthodontic appliance treatment.
Dentition Analysis
The Moyer’s method of mixed dentition analysis was the subject of a MA performed by Buwembo and Luboga in order to assess its applicability in different ethnic groups [55]. The authors performed pooling of the correlation coefficients of the 7 primary studies included in the MA and calculated the weighted mean correlations, its variances, the variances in the population correlation, and the population correlation coefficients (by means of a chi-square test). Overall, correlation coefficients were found to be in the borderline of variation with a P-value of 0.05. Splitting the articles into Caucasian and Asian groups also gave borderline P-values of 0.05. Consequently, the authors concluded that Moyer’s method of mixed dentition analysis may present population variations and they therefore proposed prediction tables to be developed for specific populations. Regarding the methodology of this study, the search strategy including only one electronic database, the small amount of studies for the various ethnic groups and their different characteristics, the lack of a quality and heterogeneity analysis as well as of publication bias assessment of the original studies included in the analysis weaken the overall results of this investigation. In addition, no statistical outcomes were presented concerning the results of the MAPs conducted for the comparison of the Caucasian and Asian ethnic groups, although such results are discussed in the text. For all these reasons, the results of this MA should be regarded with caution.
The aim of the MA performed by Liversidge et al. [56] was to investigate the timing of individual tooth formation stages according to the Demirjian’s method in children from eight countries (i.e., Australia, Belgium, Canada, England, Finland, France, South Korea and Sweden). The authors included data from studies known to them, without trying to identify potential relevant articles by searching the major electronic databases or through hand searching of dental and orthodontic journals. Nevertheless, data of permanent mandibular developing teeth from panoramic radiographs were combined and the age-of-attainment was calculated using logistic regression for tooth stages for each group, boys and girls separately. The overall mean age-of-attainment was calculated using a weighting factor inversely proportional to the variance of the mean. The results of this MA indicated that: (a) The mean ages for each group and total sample were significantly different in 65 out of 509 comparisons. Some of these were of small sample size but there was no consistent pattern. (b) Apex closure of the first molar took place significantly later in children from Canada and this might explain differences found in the dental maturity score. Consequently the authors concluded that their results suggest no major differences in the timing of tooth formation stages using the Demirjian’s dental maturity method between the children of the above mentioned 8 countries. However, these results and conclusions should not be taken into consideration, since the MAPs followed by the authors presented significant drawbacks including: (a) lack of electronic and hand searching, (b) lack of inclusion criteria, (c) lack of quality analysis of the included papers, (d) lack of assessment of publication bias, and (e) lack of heterogeneity analysis.
Cephalometric Analysis
In this MA, Trpkova et al. [57] tried to assess the magnitude of lateral cephalometric landmarks identification error for 15 landmarks. The statistical analysis of the data of the 6 primary studies included in this investigation included weighted average of the estimates in order to combine studies reporting means and standard error, as well as one-way analysis of covariance in order to combine studies reporting standard deviations. The results of this study included a measure of systematic and random errors involved when locating landmarks on lateral cephalometric radiographs and they were presented as standard mean errors and 95% CIs for the repeatability and reproducibility of the 15 cephalometric landmarks investigated. The authors concluded that a 0.59 mm of total error for the x-coordinate and 0.56 mm for the y-coordinate are acceptable levels of accuracy and only the cephalometric landmarks B, A, Ptm, S, and Go on the x-coordinate, and Ptm, A and S on the y-coordinate presented with insignificant mean error and small value for total error. Therefore, these landmarks may be considered to be reliable for cephalometric analysis of lateral radiographs. Regarding the methodology used in this MA, the following limitations were present: (a) The literature search was included only one electronic database (MEDLINE) and no other databases were investigated. (b) No information was given if a language restriction was applied during the identification process of the papers to be included in the analysis. (c) No quality and heterogeneity analysis as well as assessment of publication bias of the primary data was undertaken. (d) No information was given regarding the age of the patients of the primary studies. Thus, it can be concluded than the methodology used by the authors rather weakens the evidence produced by this MA and consequently the above mentioned results should be treated with caution.
Orthodontic Education
The purpose of the study of Al-Jewair et al. [58] was to compare the efficacy of computer-assisted learning (CAL) with traditional methods of learning in orthodontic education. Participants considered were undergraduate or postgraduate orthodontic students or orthodontic educators. Comprehensive electronic and manual searches were conducted, and after applying specific criteria 9 studies (7 randomized controlled trials and 2 prospective studies) assessing CAL in teaching orthodontic diagnosis and treatment planning were included in the analysis. Initially, the sample size, mean percentage, and standard deviation percentage were obtained from the original studies. The statistical effect size was calculated using WMDs and the corresponding 95% CIs. Heterogeneity analysis was performed using the Cochran test for homogeneity and the I2 statistic. Due to the presence of heterogeneity, the random-effects model was used for the MA. The authors couldn't draw any definitive conclusions about the time efficiency of CAL. However, the evidence derived from current well conducted MA, indicates that when CAL is applied for teaching orthodontic topics related to diagnosis and treatment planning, it is at least as effective as conventional modes of orthodontic learning, and adds an additional small but significant gain in student knowledge acquisition. They therefore suggested that further studies are needed to examine other important outcomes, such as the efficacy of CAL on performance in clinical procedures or in different orthodontic subject areas, cost-effectiveness, knowledge retention, the burden it imposes on students, and its effect on educators in terms of attitudes and effort involved.
To summarize, the evaluation of the MAPs followed in the various studies discussed in this SR, revealed partially some deficiencies that weaken the evidence produced by these studies, and consequently a more critical appraisal of their results is recommended. The main deficiencies observed include: (a) Biases during the procedure of identifying and selecting the primary studies. (b) Language or publication biases are either present or the possible measures taken (or not) to avoid these bias are not reported by the authors. (c) Lack of evaluation of the homogeneity of the primary data, and if performed, the existence of heterogeneity. (d) Lack of information regarding sample and control group sizes, which eliminates the possibility for other researchers to repeat the MA using the same information and data provided or to re-evaluate the scientific progress by applying a cumulative MA. (e) Limitations in the treatment groups, such as the existing differences concerning the age of the patients, the analysis of treatment groups with developmental differences and the comparison of different types of interventions. (f) The small number of the original articles that was possible to be included in almost all the MAs, due to the lack of high quality research articles in orthodontic literature.
Taking into consideration only the well conducted MAs that used appropriate search strategies as well as meta-analytical statistical procedures to synthesize primary data without methodological deficiencies, and at the same time included in the corresponding analysis only original articles with a verified quality of an adequate level and presented no biases or significant heterogeneity of the primary data, it can be concluded that at the beginning of the 21st century the orthodontic related issues that are supported with adequate or strong evidence include the following:
Class II treatment- (a) The risk of anterior teeth injuries tends to increase with increasing overjet size and children with an overjet larger than 3 mm are approximately twice as much at risk of traumatic dental injuries on the anterior teeth than children with an overjet less than 3 mm. In addition, the effect of the amount of overjet on the risk of dental injuries is less in boys than in girls of the same overjet group. (b) Early orthodontic treatment, followed by a later phase of treatment when the patient is in early adolescence, does not appear to have any advantages over one-phase treatment in early adolescence. (c) When treatment with functional appliances is provided, although minor and probably not clinically significant skeletal changes are expected, there is however no definite evidence concerning their efficacy on mandibular growth and in addition their use does not seem more effective than twin blocks. Thus, even if some positive effects of the functional appliances on the skeletal pattern and especially on mandibular growth can be assumed, there is still no strong evidence to support these findings.
Class III treatment - A significant composite effect of the maxillary protraction treatment on some craniofacial skeletal and dental components was evident. However, no definite conclusions can be drawn regarding the effect of the different parameters, such as the age of the patients at treatment start and the combination of maxillary protraction with rapid maxillary expansion, on treatment outcome.
Treatment of transverse problems - (a) Occlusal grinding in the primary dentition, with or without the addition of an upper removable expansion plate, is effective in preventing a posterior crossbite from being perpetuated to the mixed and permanent dentition. (b) There is no evidence of a difference in maxillary expansion, between banded vs. bonded or two point vs. four point rapid maxillary expansion, banded vs. bonded slow maxillary expansion, transpalatal arch with or without buccal root torque or upper removable expansion appliance vs. quad-helix.
External apical root resorption - The total distance and the time period of orthodontic tooth movement could be considered as treatment-related causes of external apical root resorption, and consequently, all factors that contribute to a prolonged duration of active orthodontic treatment might enhance the phenomenon of apical root resorption, especially in pre-disposed individuals.
Dental anomalies - (a) The prevalence of congenitally missing teeth differs in relation to continent and gender: for both sexes was higher in Europe and Australia than in North American Caucasians, while in females it was 1.37 times higher than in males for all three continents examined; the mandibular second premolars are affected most frequently, followed by the maxillary lateral incisors and maxillary second premolars; and bilateral occurrence of congenitally missing maxillary lateral incisors is more frequent than unilateral, while the opposite was found for the first maxillary premolars and the second mandibular and maxillary premolars. (b) Tooth transposition can be regarded as an isolated phenomenon rather than a syndrome, while occasionally it can be accompanied by some characteristic features and dental anomalies, but without distinct associations; tooth transposition has a mean prevalence of 0.33%; this prevalence seems to be similar between the two genders; tooth transposition appears more frequently in the maxilla than in the mandible and more unilaterally than bilaterally.
Frequency of severe occlusal problems - The developmental stage of the dentition is significantly associated to the severity of malocclusion, while the prevalence of occlusal problems is almost twice as large in patients with permanent than in patients with deciduous dentition.
Nickel hypersensitivity - (a) No statistically significant difference exists between the odds for a positive patch-test result before orthodontic treatment and after the placement of the appliances. (b) Nickel hypersensitivity of orthodontic patients with no history of cutaneous piercing or with skin pierced prior to orthodontic treatment does not differ statistically significant after treatment with the corresponding hypersensitivity of the general population. (c) Orthodontic treatment is not associated with an increase in the prevalence of nickel hypersensitivity unless subjects have a history of cutaneous piercing.
Obstructive sleep apnea syndrome - (a) There is increasing evidence suggesting that oral appliances improve subjective sleepiness and sleep disordered breathing. (b) Nasal continuous positive airway pressure (CPAP) therapy appears to be more effective in improving sleep disordered breathing than oral appliances. (c) Although more evidence is needed, it may be more appropriate to recommend oral appliances treatment to patients with mild symptomatic OSAH, as well as to those patients who are unwilling or unable to tolerate CPAP therapy.
Orthodontic education - When CAL is applied for teaching orthodontic topics related to diagnosis and treatment planning, it is at least as effective as conventional modes of orthodontic learning, and adds an additional small but significant gain in student knowledge acquisition.
Oral hygiene - Current evidence is insufficient to support the comparative efficacy of powered toothbrushes in reducing gingivitis in patients undergoing fixed orthodontic appliance treatment.
Orthodontics and temporomandibular disorders - There is not sufficient evidence to support the effectives of the use of occlusal splints for the treatment of sleep bruxism with regard to sleep outcomes, but their use might be beneficial with regard to tooth wear.
Incisor intrusion, Dentition analysis, Cephalometric analysis - No evidence based conclusions could be drawn.
CONCLUSIONS
Only a few orthodontic related issues have been yet investigated by means of MAs, which are considered as study designs providing the highest level of evidence in medical literature. In addition, for some of these issues investigated in the corresponding MAs no definite conclusions could be drawn, due to significant methodological deficiencies of these studies, such as the use of not appropriate meta-analytical statistical procedures, as well as the lack of high quality original studies or the heterogeneity of the primary data. According to this investigation, which evaluated the existing MAs in orthodontic literature, it can be therefore concluded that at the begin of the 21st century there is evidence for only a few orthodontic related issues and more well-conducted high quality research studies are needed to produce strong evidence in order to support evidence-based clinical practice in orthodontics.
Appendix
Appendix I. Papers Excluded from this SR and Reason for their Exclusion (authors in alphabetical order)
| Nr | Study | Reason for Exclusion |
|---|---|---|
| 1. | [No authors listed] Malocclusion Therapy; Researchers from University of Geneva, Department of Orthodontics detail new studies and findings in the area of malocclusion therapy. Genomics Genets Weekly Atlanta Oct 19, 2007; p. 227. | Comment on: Angle Orthod. 2007 Sep; 77(5): 907-14. |
| 2. | Agabiti-Rosei E, Muiesan ML, Rizzoni D. [Antihypertensive treatment and left ventricular hypertrophy]. Ann Ital Med Int 1993 Oct; 8 (Suppl): 97S-103S. | Subject not relevant to orthodontics |
| 3. | Agabiti-Rosei E. Evaluation of the cardiac effects of antihypertensive agents. J Cardiovasc Pharmacol. 1994; 23 (Suppl 5): S42-8. | Subject not relevant to orthodontics |
| 4. | Andreasen JO, Andreasen FM, Skeie A, Hjorting-Hansen E, Schwartz O. Effect of treatment delay upon pulp and periodontal healing of traumatic dental injuries - a review article. Dent Traumatol 2002; 18: 116-28. | Subject not relevant to orthodontics |
| 5. | Arhun, N; Arman, A; Sesen, C, et al. Shear bond strength of orthodontic brackets with 3 self-etch adhesives. Am J Orthodont Dentofac Orthoped 2006; 129 (4), pp. 547-550. | Original study, not meta-analysis |
| 6. | Ash MM. Occlusion: reflections on science and clinical reality. J Prosthet Dent 2003; 90: 373-84. | Subject not relevant to orthodontics |
| 7. | Ashley PF, Williams CECS, Moles DR, Parry J. Sedation versus general anaesthesia for provision of dental treatment in under 18 year olds. Cochrane Database Systemat. Rev 2009; (1), Art. No.: CD006334. DOI: 10.1002/14651858.CD006334.pub2 | Subject not relevant to orthodontics |
| 8. | Athanasiou AE, Gjorup H, Toutountzakis N. Soft tissue and dentoskeletal profile changes associated with mandibular advancement osteotomy. Hell Period Stomat Gnathopathoprosopike Cheir 1990; 5 (4), pp. 157-163. | Original study, not meta-analysis |
| 9. | Avenell A, Brown TJ, McGee MA, Campbell MK, Grant AM, Broom J, Jung RT, Smith WC. What interventions should we add to weight reducing diets in adults with obesity? A systematic review of randomized controlled trials of adding drug therapy, exercise, behaviour therapy or combinations of these interventions. J Hum Nutr Diet 2004 Aug; 17(4): 293-316. | Subject not relevant to orthodontics |
| 10. | Bauer R, Gedrange T, Bauer K, Walter B. Intrauterine growth restriction induces increased capillary density and accelerated type I fiber maturation in newborn pig skeletal muscles. J Perinatal Med 34(3): 235-242. | Subject not relevant to orthodontics |
| 11. | BeGole EA, Sadowsky C. Methodologies for evaluating long-term stability of dental relationships after orthodontic treatment. Semin Orthod 1999; 5: 142-50. | Subject not relevant to orthodontics |
| 12. | Beirne PV, Clarkson JE, Worthington HV. Recall intervals for oral health in primary care patients. Cochrane Database Systemat Rev 2007, (4), Art. No.: CD004346. DOI: 10.1002/14651858.CD004346.pub3. | Subject not relevant to orthodontics |
| 13. | Benson PE, Parkin N, Millett DT, Dyer F, Vine S, Shah A. Fluorides for the prevention of white spots on teeth during fixed brace treatment. Cochrane Database Systemat Rev 2004, (3), Art. No.: CD003809. DOI: 10.1002/14651858.CD003809.pub2. | Systematic review |
| 14. | Benson PE, Shah AA, Millett DT, Dyer F, Parkin N, Vine RS. Fluorides, orthodontics and demineralization: a systematic review. J Orthod 2005; 32: 102-14. | Systematic review |
| 15. | Berg A, Kloock B, König D. [Dietary modification in hypertensives]. MMW Fortschr Med 2006 Nov 23; 148(47): 36-7, 39. | Subject not relevant to orthodontics |
| 16. | Bergstrand F, Twetman S. Evidence for the efficacy of various methods of treating white-spot lesions after debonding of fixed orthodontic appliances. J Clin Orthod 2003; 37: 19-21. | Narrative review |
| 17. | Bhatt SP, Luqman-Arafath TK, Guleria R. Non-pharmacological management of hypertension. Indian J Med Sci. 2007 Nov; 61(11): 616-24. | Subject not relevant to orthodontics |
| 18. | Bloch, K.E. Alternatives to CPAP in the treatment of the obstructive sleep apnoea syndrome. Swiss Medical Weekly 2006; 136 (17-18), pp. 261-267. | Narrative review |
| 19. | Bonner BC, Clarkson JE, Dobbyn L, Khanna S. Slow-release fluoride devices for the control of dental decay. Cochrane Database Systemat Rev 2006, (4). Art. No.: CD005101. DOI: 10.1002/14651858.CD005101.pub2. | Subject not relevant to orthodontics |
| 20. | Buijs GJ, Stegenga B, Bos RR. Efficacy and safety of biodegradable osteofixation devices in oral and maxillofacial surgery: a systematic review. J Dent Res 2006 Nov; 85(11): 980-9. | Subject not relevant to orthodontics |
| 21. | Burke SP. A meta-analysis of mandibular intercanine width in treatment and postretention: A study regrading the stability of alteration of mandibular intercanine width in orthodontic treatment. Dissertation. University of Louisville, 1994. | Comment on: Angle Orthod 1998; 68: 53-60. |
| 22. | Büyükyilmaz T, Zachrisson BU. Improved orthodontic bonding to silver amalgam. Part 2. Lathe-cut, admixed, and spherical amalgams with different intermediate resins. Angle Orthodontist 1998; 68 (4), pp. 337-344. | Original study, not meta-analysis |
| 23. | Büyükyilmaz T, Zachrisson YØ, Zachrisson BU. Improving orthodontic bonding to gold alloy. Am J Orthodont Dentofac Orthoped 1995; 108 (5), pp. 510-518. | Original study, not meta-analysis |
| 24. | Carless PA, Henry DA, Anthony DM. Fibrin sealant use for minimising peri-operative allogeneic blood transfusion. Cochrane Database of Systematic Reviews 2003, (1), Art. No.: CD004171. DOI: 10.1002/14651858.CD004171. | Subject not relevant to orthodontics |
| 25. | Carr A, Ebbert J. Interventions for tobacco cessation in the dental setting. Cochrane Database Systemat Rev 2006, (1), Art. No.: CD005084. DOI: 10.1002/14651858.CD005084.pub2. | Subject not relevant to orthodontics |
| 26. | Carvalho FR, Lentini-Oliveira DA, Machado MAC, Saconato H, Prado LBF, Prado GF. Oral appliances and functional orthopaedic appliances for obstructive sleep apnoea in children. Cochrane Database of Systemat Rev 2007, (2), Art. No.: CD005520. DOI: 10.1002/14651858.CD005520.pub2. | Systematic review |
| 27. | Chaushu S, Shapira J, Heling I, Becker A. Emergency orthodontic treatment after the traumatic intrusive luxation of maxillary incisors. Am J Orthod Dentofacial Orthop 2004; 126: 162-72. | Report of cases & Systematic review |
| 28. | Cheung LK, Chua HD. A meta-analysis of cleft maxillary osteotomy and distraction osteogenesis. Int J Oral Maxillofac Surg 2006 Jan; 35(1): 14-24. Epub 2005 Sep 8. | Subject not relevant to orthodontics - Cleft lip and palate |
| 29. | Chia M. Evidence not strong enough to advocate powered toothbrushes over manual for orthodontic patients. Evid Based Dent 2008; 9(3): 78. | Comment on: Am J Orthod Dentofacial Orthop. 2008 Feb; 133(2): 187.e1-14. |
| 30. | Clark T. Book Reviews Featuring a Special Essay by Russell W. Belk. Journal of Marketing. 2002; 66(1): 120-130. | Book Reviews |
| 31. | Clark, S.A., Gordon, P.H., McCabe, J.F. An ex vivo investigation to compare orthodontic bonding using a 4-META-based adhesive or a composite adhesive to acid-etched and sandblasted enamel. J Orthodont 2003; 30(1), pp. 51-58; discussion 23. | Original study, not meta-analysis |
| 32. | Costa F, Robiony M, Politi M. Stability of sagittal split ramus osteotomy used to correct Class III malocclusion: review of the literature. Int J Adult Orthodon Orthognath Surg 2001; 16: 121-9. | Narrative review |
| 33. | Creager MA. Medical management of peripheral arterial disease. Cardiol Rev 2001 Jul-Aug; 9(4): 238-45. | Subject not relevant to orthodontics |
| 34. | Cronin A. Periodontal disease is a risk marker for coronary heart disease? Evid Based Dent 2009; 10(1): 22. | Subject not relevant to orthodontics |
| 35. | Dansinger ML, Tatsioni A, Wong JB, Chung M, Balk EM. Meta-analysis: the effect of dietary counseling for weight loss. Ann Intern Med 2007 Jul 3; 147(1): 41-50. | Subject not relevant to orthodontics |
| 36. | Davies AA, Davey Smith G, Harbord R, Bekkering GE, Sterne JA, Beynon R, Thomas S. Nutritional interventions and outcome in patients with cancer or preinvasive lesions: systematic review. J Natl Cancer Inst. 2006 Jul 19; 98(14): 961-73. | Subject not relevant to orthodontics |
| 37. | Davies NM, Longstreth J, Jamali F. Misoprostol Therapeutics Revisited. Pharmacotherapy. Vol. 21(1): 60-73. | Subject not relevant to orthodontics |
| 38. | Dawson KH, Chigurupati R. Fixation of mandibular fractures: a tincture of science. Ann R Australas Coll Dent Surg 2002 Oct; 16: 118-22. | Subject not relevant to orthodontics |
| 39. | De Vries N, Den Herder C, Hessel NS, Hoekema A. Treatment of obstructive sleep apnea syndrome in adults [7] (multiple letters) | [Behandeling van het obstructieve slaapapneusyndroom bij volwassenen]. Nederlands Tijdschrift voor Geneeskunde 2004; 148 (5): pp. 250-251. | Letter to the editor |
| 40. | Derks A, Katsaros C, Frencken JE, van't Hof MA, Kuijpers-Jagtman AM. Caries-inhibiting effect of preventive measures during orthodontic treatment with fixed appliances. A systematic review. Caries Res 2004; 38: 413-20. | Systematic review |
| 41. | Dodson T. Efficacy of biodegradable osteofixation devices in oral and maxillofacial surgery remains inconclusive. Evid Based Dent 2007; 8(2): 44. | Subject not relevant to orthodontics |
| 42. | Dorri M, Nasser M, Oliver R. Resorbable versus titanium plates for facial fractures. Cochrane Database of Systematic Reviews 2009, (1), Art. No.: CD007158. DOI: 10.1002/14651858.CD007158.pub2. | Subject not relevant to orthodontics |
| 43. | Esposito M, Grusovin MG, Kwan S, Worthington HV, Coulthard P. Interventions for replacing missing teeth: bone augmentation techniques for dental implant treatment. Cochrane Database of Systematic Reviews 2008, (3), Art. No.: CD003607. DOI: 10.1002/14651858.CD003607.pub3. | Subject not relevant to orthodontics |
| 44. | Esposito M, Grusovin MG, Maghaireh H, Coulthard P, Worthington HV. Interventions for replacing missing teeth: management of soft tissues for dental implants. Cochrane Database Syst Rev 2007 Jul 18; (3): CD006697. | Subject not relevant to orthodontics |
| 45. | Fedorowicz Z, Nasser M, Newton T, Oliver R. Resorbable versus titanium plates for orthognathic surgery. Cochrane Database of Systematic Reviews 2007, (2), Art. No.: CD006204. DOI: 10.1002/14651858.CD006204.pub2. | Subject not relevant to orthodontics |
| 46. | Feldmann I, Bondemark L. Orthodontic anchorage: a systematic review. Angle Orthod 2006 May; 76(3): 493-501. | Systematic review |
| 47. | Fernandes M, Atallah AN, Soares BG, Humberto S, Guimarães S, Matos D, Monteiro L, Richter B. Intragastric balloon for obesity. Cochrane Database Syst Rev 2007 Jan 24; (1): CD004931. | Subject not relevant to orthodontics |
| 48. | Fleming PS, DiBiase AT. Systematic reviews in orthodontics: what have we learned? Int Dent J 2008 Feb; 58(1): 10-4. | Systematic review |
| 49. | Flores-Mir C, Major MP, Major PW. Search and selection methodology of systematic reviews in orthodontics (2000-2004). Am J Orthod Dentofacial Orthop 2006 Aug; 130(2): 214-7. | Systematic review |
| 50. | Flores-Mir C, Major PW. Cephalometric facial soft tissue changes with the twin block appliance in Class II division 1 malocclusion patients. A systematic review. Angle Orthod 2006 Sep; 76(5): 876-81. | Systematic review |
| 51. | Flores-Mir C, Nebbe B, Major PW. Use of skeletal maturation based on hand-wrist radiographic analysis as a predictor of facial growth: a systematic review. Angle Orthod 2004; 74: 118-24. | Systematic review |
| 52. | Fox N. Longer orthodontic treatment may result in greater external apical root resorption. Evid Based Dent 2005; 6: 21. | Comment on: Orthod Craniofac Res 2004;7:71-8. |
| 53. | Fox NA, McCabe JF, Buckley JG. A critique of bond strength testing in orthodontics. Br J Orthod 1994; 21: 33-43. | Narrative review |
| 54. | Fricton J. Current evidence providing clarity in management of temporomandibular disorders: summary of a systematic review of randomized clinical trials for intra-oral appliances and occlusal therapies. J Evid Based Dent Pract 2006; 6: 48-52. | Systematic review (summary of results) |
| 55. | Fritz ME. Two-stage implant systems. Adv Dent Res 1999 Jun; 13: 162-9. | Subject not relevant to orthodontics |
| 56. | Gesch D, Bernhardt O, Alte D, Schwahn C, Kocher T, John U, Hensel E. Prevalence of signs and symptoms of temporomandibular disorders in an urban and rural German population: results of a population-based Study of Health in Pomerania. Quintessence Int 2004; 35: 143-50. | Original study, not meta-analysis |
| 57. | Gessa S. Simple strategies for variance uncertainty in meta-analysis. MSc(R) thesis, University of Glasgow, 2008. | Subject not relevant to orthodontics |
| 58. | Gioka C, Eliades T. Materials-induced variation in the torque expression of preadjusted appliances. Am J Orthod Dentofacial Orthop 2004; 125: 323-8. | Narrative review |
| 59. | Glenny AM, Hooper L, Shaw BC, Reilly S, Kasem S, Reid J. Feeding interventions for growth and development in infants with cleft lip, cleft palate or cleft lip and palate. Cochrane Database of Systematic Reviews 2004, (3). Art. No.: CD003315. DOI: 10.1002/14651858.CD003315.pub2. | Subject not relevant to orthodontics - Cleft lip and palate |
| 60. | Goh HH, Fernandez Mauleffinch LM. Interspace/interdental brushes for oral hygiene in orthodontic patients with fixed appliances. Cochrane Database of Systematic Reviews 2007, (3), Art. No.: CD005410. DOI: 10.1002/14651858.CD005410.pub2. | Systematic review |
| 61. | Golan I, Baumert U, Hrala BP, Mussig D. Dentomaxillofacial variability of cleidocranial dysplasia: clinicoradiological presentation and systematic review. Dentomaxillofac Radiol 2003; 32: 347-54. Erratum in: Dentomaxillofac Radiol 2004; 33: 422. | Systematic review |
| 62. | Gruen RL, Weeramanthri TS, Knight SS, Bailie RS. Specialist outreach clinics in primary care and rural hospital settings. Cochrane Database of Systematic Reviews 2003, (4), Art. No.: CD003798. DOI: 10.1002/14651858.CD003798.pub2. | Subject not relevant to orthodontics |
| 63. | Grusovin MG, Coulthard P, Jourabchian E, Worthington HV, Esposito M. Interventions for replacing missing teeth: maintaining and recovering soft tissue health around dental implants. Cochrane Database of Systematic Reviews 2008, (1), Art. No.: CD003069. DOI: 10.1002/14651858.CD003069.pub3. | Subject not relevant to orthodontics |
| 64. | Hanke BA, Motschall E, Türp JC. Association between orthopedic and dental findings: what level of evidence is available? J Orofac Orthop 2007 Mar; 68(2): 91-107. | Subject not relevant to orthodontics |
| 65. | Harvald B, Hauge G, Ohm K, Kaare K, Christensen A, Niels S, Holm V. The Danish Twin Registry: Past and Present. Twin Res Human Genet Vol. 7(4): 318-335. | Subject not relevant to orthodontics |
| 66. | Hashish DI, Mostafa YA. Effect of lip bumpers on mandibular arch dimensions. Am J Orthod Dentofacial Orthop 2009 Jan; 135(1): 106-9. | Systematic review |
| 67. | Hausen H. Oral health promotion reduces plaque and gingival bleeding in the short term. Evid Based Dent 2005; 6(2): 31. | Subject not relevant to orthodontics |
| 68. | Hawes J, McEwan P, McGuire W. Nasal versus oral route for placing feeding tubes in preterm or low birth weight infants. Cochrane Database Syst Rev 2004, (3), Art. No.: CD003952. DOI: 10.1002/14651858.CD003952.pub2. | Subject not relevant to orthodontics |
| 69. | Hayakawa K, Nd: YAG laser for debonding ceramic orthodontic brackets. Am J Orthodon Dentofac Orthoped 2005; 128 (5), pp. 638-647. | Original study, not meta-analysis |
| 70. | Henry PJ. Oral implant restoration for enhanced oral function. Clin Exp Pharmacol Physiol 2005 32: 1-2 (123-127). | Subject not relevant to orthodontics |
| 71. | How Kau C. Orthodontic retention regimes: will we ever have the answer? Evid Based Dent. 2006; 7(4): 100. | Comment on: Cochrane Database Syst Rev 2006; (1): CD002283. |
| 72. | Howe GR, Hirohata T, Hislop TG, Iscovich JM, Yuan JM, Katsouyanni K, Lubin F, Marubini E, Modan B, Rohan T, et al. Dietary factors and risk of breast cancer: combined analysis of 12 case-control studies. J Natl Cancer Inst 1990 Apr 4; 82(7): 561-9. | Subject not relevant to orthodontics |
| 73. | Hunt O, Burden D, Hepper P, Johnston C. The psychosocial effects of cleft lip and palate: a systematic review. Eur J Orthod 2005; 27: 274-85. | Subject not relevant to orthodontics - Cleft lip and palate |
| 74. | Ikemura K, Tay FR, Nishiyama, N, et al. Multi-purpose bonding performance of newly synthesized phosphonic acid monomers. Dental Mater. J 2007; 26 (1), pp. 105-115. | Original study, not meta-analysis |
| 75. | Ismail AI, Bader JD. Evidence-based dentistry in clinical practice. J Am Dental Assoc 2004; 135 (1), pp. 78-83. | Subject not relevant to orthodontics |
| 76. | Itoh T, Fukushima T, Inoue Y, Arita S, Miyazaki K. Effect of water, saliva and blood contamination on bonding of metal brackets with a 4-META/MMA/TBB resin to etched enamel. Am J Dentistry 1999; 12, pp. 299-304. | Original study, not meta-analysis |
| 77. | Jagger R. The effectiveness of occlusal splints for sleep bruxism. Evid Based Dent. 2008; 9(1): 23. | Comment on: Cochrane Database Syst Rev 2007; (4): CD005514. |
| 78. | Jang JC, Fields HW, Vig KWL, Beck FM. Controversies in the timing of orthodontic treatment. Seminars in Orthodontics 2005; 11 (3), pp. 112-118. | Narrative review |
| 79. | Javidkar M, Darvish J, Riahi Bakhtiari A. Morphological and morphometric analyses of dental and cranial characters in Apodemus hyrcanicus and A. witherbyi (Rodentia: Muridae) from Iran. Mammalia, Vol. 71(1-2): 56-62. | Subject not relevant to orthodontics |
| 80. | Kalha A. Can I intrude? Evid Based Dent 2007; 8(1): 17. | Comment on: Am J Orthod Dentofacial Orthop 2005 Aug; 128(2): 212-9. |
| 81. | Kalha AS. Is anchorage reinforcement with implants effective in orthodontics? Evid Based Dent 2008; 9(1): 13-4. | Comment on: Cochrane Database Syst Rev 2007; (3): CD005098. |
| 82. | Kawabata R, Hayakawa T, Kasai K. Modification of 4-META/MMA-TBB resin for safe debonding of orthodontic brackets - Influence of the addition of degradable additives or fluoride compound. Dental Mater J 2006; 25 (3), pp. 524-532. | Original study, not meta-analysis |
| 83. | Kazuno T, Fukushima, T, Hayakawa T, Inoue Y, Ogura R, Kaminishi H, Miyazaki K. Antibacterial activities and bonding of MMA/TBB resin containing amphiphilic lipids. Dental Mater J 2005; 24 (2), pp. 244-250. | Original study, not meta-analysis |
| 84. | Keilig L, Bourauel C, Grüner M, Hültenschmidt R, Bayer S, Utz K-H, Stark H. Aufbau und Erprobung eines neuartigen Meßsystems für die dentale Biomechanik – Meßprinzip und Beispielmessungen des Hexapod-Meß-Systems [Design and Testing of a Novel Measuring Set-up for Use in Dental Biomechanics – Measuring Principle and Exemplary Measurements with the Hexapod Measuring System]. Biomedizinische Technik/Biomedical Engineering, Vol. 49(7-8): 208-215. | Subject not relevant to orthodontics |
| 85. | Kersey ML, Nebbe B, Major PW. Temporomandibular joint morphology changes with mandibular advancement surgery and rigid internal fixation: a systematic literature review. Angle Orthod 2003; 73: 79-85. | Systematic review |
| 86. | Koh H, Robinson PG. Occlusal adjustment for treating and preventing temporomandibular joint disorders. The Cochrane Database of Systematic Reviews 2003, Issue 1. Art. No: CD003812. DOI: 10.1002/14651858.CD003812. | Systematic review |
| 87. | Koletzko B, von Kries R, Monasterolo RC, SubÃas JE, Scaglioni S, Giovannini M, Beyer J, Demmelmair H, Anton B, Gruszfeld D, Dobrzanska A, Sengier A, Langhendries JP, Cachera MF, Grote V; European Childhood Obesity Trial Study Group. Infant feeding and later obesity risk. Adv Exp Med Biol 2009; 646: 15-29. | Subject not relevant to orthodontics |
| 88. | Kraus DM, Stohlmeyer LA, Hannon PR, Freels SA. Effectiveness and Infant Acceptance of the Rx Medibottle versus the Oral Syringe. Pharmacotherapy. Vol. 21(4): 416-423. | Subject not relevant to orthodontics |
| 89. | Kuijpers MA, Kuijpers-Jagtman AM. [Orthodontics in general practice 3. Angle Class II/1 malocclusion: one-phase treatment treatment preferred to two-phase treatment]. Ned Tijdschr Tandheelkd. 2008 Jan; 115(1): 22-8. | Narrative review |
| 90. | Labanauskaite B, Jankauskas G, Vasiliauskas A, Haffar N. Implants for orthodontic anchorage. Meta-analysis. Stomatologija. 2005; 7(4): 128-32. | Systematic review |
| 91. | Lagravere MO, Major PW, Flores-Mir C. Long-term skeletal changes with rapid maxillary expansion: a systematic review. Angle Orthod 2005 Nov; 75(6): 1046-52. | Systematic review |
| 92. | Lagravere MO, Major PW, Flores-Mir C. Skeletal and dental changes with fixed slow maxillary expansion treatment: a systematic review. J Am Dent Assoc 2005; 136: 194-9. | Systematic review |
| 93. | Lentini-Oliveira D, Carvalho FR, Qingsong Y, Junjie L, Saconato H, Machado MA, Prado LB, Prado GF. Orthodontic and orthopaedic treatment for anterior open bite in children. Cochrane Database Syst Rev 2007 Apr 18; (2): CD005515. | Systematic review |
| 94. | Leonard LG. Breastfeeding Rights of Multiple Birth Families and Guidelines for Health Professionals. Twin Research and Human Genetics Vol. 6(1): 34-45. | Subject not relevant to orthodontics |
| 95. | Lidral AC, Moreno LM. Progress toward discerning the genetics of cleft lip. Curr Opin Pediatr 2005 Dec; 17(6): 731-9. | Subject not relevant to orthodontics - Cleft lip and palate |
| 96. | Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database of Systematic Reviews 2006, (1). Art. No.: CD002283. DOI: 10.1002/14651858.CD002283.pub3. | Systematic review |
| 97. | Liu Z, McGrath C, Hägg U. The impact of malocclusion/orthodontic treatment need on the quality of life. Angle Orthod 2009 May; 79(3): 585-91. | Systematic review |
| 98. | MacDonald-Jankowski DS, Yeung R, Lee KM, Li TK. Odontogenic myxomas in the Hong Kong Chinese: clinico-radiological presentation and systematic review. Dentomaxillofac Radiol 2002; 31: 71-83. | Subject not relevant to orthodontics |
| 99. | Mandall NA, Hickman J, Macfarlane TV, Mattick RCR, Millett DT, Worthington HV. Adhesives for fixed orthodontic brackets. Cochrane Database of Systematic Reviews 2003, (2), Art. No.: CD002282. DOI: 10.1002/14651858.CD002282. | Systematic review |
| 100. | Marinho VCC, Higgins JPT, Logan S, Sheiham A. Fluoride gels for preventing dental caries in children and adolescents. Cochrane Database of Systematic Reviews 2002, (1), Art. No.: CD002280. DOI: 10.1002/14651858.CD002280. | Subject not relevant to orthodontics |
| 101. | Marinho VCC, Higgins JPT, Logan S, Sheiham A. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database of Systematic Reviews 2003, (1), Art. No.: CD002278. DOI: 10.1002/14651858.CD002278. | Subject not relevant to orthodontics |
| 102. | Marinho VCC, Higgins JPT, Logan S, Sheiham A. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database of Systematic Reviews 2002, (1), Art. No.: CD002279. DOI: 10.1002/14651858.CD002279. | Subject not relevant to orthodontics |
| 103. | Mariotti A. Efficacy of chemical root surface modifiers in the treatment of periodontal disease. A systematic review. Ann Periodontol 2003 Dec; 8(1): 205-26.. | Subject not relevant to orthodontics |
| 104. | Marzooq AA, Yatabe M, Ai M. What types of occlusal factors play a role in temporomandibular disorders...? A literature review. J Med Dent Sci 1999; 46: 111-6. | Narrative review |
| 105. | Matharu L, Ashley PF. Sedation of anxious children undergoing dental treatment. Cochrane Database of Systematic Reviews 2006, (1), Art. No.: CD003877. DOI: 10.1002/14651858.CD003877.pub3. | Subject not relevant to orthodontics |
| 106. | Mattheeuws N, Dermaut L, Martens G. Has hypodontia increased in Caucasians during the 20th century? A meta-analysis. Eur J Orthod 2004; 26: 99-103. | Systematic review |
| 107. | McBain AJ, Madhwani T, Eatough J, Ledder R. An introduction to probiotics for dental health. Food Science & Technology Bulletin: Functional Foods Vol. 6(2): 5-29. | Subject not relevant to orthodontics |
| 108. | Mettes DTG, Nienhuijs MMEL, van der Sanden WJM, Verdonschot EH, Plasschaert A. Interventions for treating asymptomatic impacted wisdom teeth in adolescents and adults. Cochrane Database of Systematic Reviews 2005, (2), Art. No.: CD003879. DOI: 10.1002/14651858.CD003879.pub2 | Subject not relevant to orthodontics |
| 109. | Millett D, Mandall N, Hickman J, Mattick R, Glenny AM. Adhesives for fixed orthodontic bands. A systematic review. Angle Orthod 2009 Jan; 79(1): 193-9. | Systematic review |
| 110. | Millett DT, Cunningham S, O'Brien KD, Benson PE, Williams A, de Oliveira CM. Orthodontic treatment for deep bite and retroclined upper front teeth in children. Cochrane Database of Systematic Reviews 2006, (4), Art. No.: CD005972. DOI: 10.1002/14651858.CD005972.pub2. | Systematic review |
| 111. | Millett DT, Glenny AM, Mattick CR, Hickman J, Mandall NA. Adhesives for fixed orthodontic bands. Cochrane Database Syst Rev 2006 Jul 19; 3: CD004485. Update in: Cochrane Database Syst Rev 2007; (2): CD004485. | Systematic review |
| 112. | Millett DT, Glenny AM, Mattick RCR, Hickman J, Mandall NA. Adhesives for fixed orthodontic bands. Cochrane Database of Systematic Reviews 2007, (2), Art. No.: CD004485. DOI: 10.1002/14651858.CD004485.pub3. | Systematic review |
| 113. | Miwa H, Miyazawa K, Goto S, Kondo T, Hasegawa A. A resin veneer for enamel protection during orthodontic treatment. European Journal of Orthodontics 2001; 23 (6), pp. 759-767. | Original study, not meta-analysis |
| 114. | Moore NL. Suffer the little children: fixed intraoral habit appliances for treating childhood thumbsucking habits: a critical review of the literature. Int J Orofacial Myology 2002; 28: 6-38. | Narrative review |
| 115. | Mucedero M, Coviello A, Baccetti T, Franchi L, Cozza P. Stability factors after double-jaw surgery in Class III malocclusion. A systematic review. Angle Orthod. 2008 Nov; 78(6): 1141-52. | Systematic review |
| 116. | Nasser M, Fedorowicz Z, Newton T, Nouri M. Interventions for the management of submucous cleft palate. Cochrane Database of Systematic Reviews 2008, (1), Art. No.: CD006703. DOI: 10.1002/14651858.CD006703.pub2. | Subject not relevant to orthodontics - Cleft lip and palate |
| 117. | Nollet PJ, Katsaros C, Van't Hof MA, Kuijpers-Jagtman AM. Treatment outcome in unilateral cleft lip and palate evaluated with the GOSLON yardstick: a meta-analysis of 1236 patients. Plast Reconstr Surg 2005 Oct; 116(5): 1255-62. | Subject not relevant to orthodontics - Cleft lip and palate |
| 118. | O'Neill J. Do lip bumpers work? Evid Based Dent 2009; 10(2): 48-9. | Comment on: Am J Orthod Dentofacial Orthop. 2009 Jan;135(1):106-9. |
| 119. | O'Neill JR. Functional appliances and mandibular growth--is there an effect? Evid Based Dent 2004; 5: 74. HANDSEARCHING!!!!! | Comment on: Am J Orthod Dentofacial Orthop. 2009 Jan;135(1):106-9. |
| 120. | Orthlieb JD, Giraudeau A, Laplanche O. Occlusion and dysfunction: the paradox of dentofacial orthopedics. Orthod Fr 1998; 69: 69-78. | Systematic review |
| 121. | Padwal R, Li SK, Lau DC. Long-term pharmacotherapy for obesity and overweight. Cochrane Database Syst Rev 2004; (3): CD004094. | Subject not relevant to orthodontics |
| 122. | Ow AT, Cheung LK. Meta-analysis of mandibular distraction osteogenesis: clinical applications and functional outcomes. Plast Reconstr Surg 2008; 121: 54e-69e. | Systematic review |
| 123. | Papadopoulos MA, Gkiaouris I. A critical evaluation of meta-analyses in orthodontics. Am J Orthod Dentofacial Orthop 2007 May; 131(5): 589-99. | Systematic review |
| 124. | Papadopoulos MA. Meta-analysis in evidence-based orthodontics. Orthod Craniofac Res 2003; 6: 112-26. | Narrative review |
| 125. | Parkin N, Benson PE, Shah A, Thind B, Marshman Z, Glenroy G, Dyer F. Extraction of primary (baby) teeth for unerupted palatally displaced permanent canine teeth in children. Cochrane Database of Systematic Reviews 2009, (2). Art. No.: CD004621. DOI: 10.1002/14651858.CD004621.pub2. | Systematic review |
| 126. | Parkin N, Benson PE, Thind B, Shah A. Open versus closed surgical exposure of canine teeth that are displaced in the roof of the mouth. Cochrane Database of Systematic Reviews 2008, (4), Art. No.: CD006966. DOI: 10.1002/14651858.CD006966.pub2. | Systematic review |
| 127. | Patton LL, Shugars DA, Bonito AJ. A systematic review of complication risks for HIV-positive patients undergoing invasive dental procedures. J Am Dent Assoc 2002 Feb; 133(2): 195-203. | Subject not relevant to orthodontics |
| 128. | Paul JE, Ling E, Lalonde C, Thabane L. Deliberate hypotension in orthopedic surgery reduces blood loss and transfusion requirements: a meta-analysis of randomized controlled trials. Can J Anaesth 2007 Oct; 54(10): 799-810. | Subject not relevant to orthodontics |
| 129. | Petren S, Bondemark L, Soderfeldt B. A systematic review concerning early orthodontic treatment of unilateral posterior crossbite. Angle Orthod 2003; 73: 588-96. | Systematic review |
| 130. | Popowich K, Nebbe B, Major PW. Effect of Herbst treatment on temporomandibular joint morphology: a systematic literature review. Am J Orthod Dentofacial Orthop 2003; 123: 388-94. | Systematic review |
| 131. | Poyak J. Effects of pacifiers on early oral development. Int J Orthod Milwaukee 2006 Winter; 17(4): 13-6. | Systematic review |
| 132. | Que K-H, Guo B. Evidence-based practice of pit and fissure sealants. Chin J Evid-Based Med 2006 6: 2 (146-149). | Subject not relevant to orthodontics |
| 133. | Ren Y, Maltha JC, Kuijpers-Jagtman AM. Optimum force magnitude for orthodontic tooth movement: a systematic literature review. Angle Orthod 2003; 73: 86-92. | Systematic review |
| 134. | Riley M, Bearn DR. A systematic review of clinical trials of aligning archwires. J Orthod 2009 Mar; 36(1): 42-51; discussion 15. | Systematic review |
| 135. | Rinchuse DJ, Rinchuse DJ, Kandasamy S, Ackerman MB. Deconstructing evidence in orthodontics: making sense of systematic reviews, randomized clinical trials, and meta analyses. World J Orthod 2008 Summer; 9(2): 167-76. | Narrative review |
| 136. | Rinchuse, DJ; Kandasamy, S. Articulators in orthodontics: An evidence-based perspective. Am J Orthodont Dentofac Orthoped 2006; 129 (2), pp. 299-308. | Narrative review |
| 137. | Robinson PG, Deacon SA, Deery C, Heanue M, Walmsley AD, Worthington HV, Glenny AM, Shaw WC. Manual versus powered toothbrushing for oral health. The Cochrane Database of Systematic Reviews 2005, (2), Art. No.: CD002281. DOI: 10.1002/14651858.CD002281.pub2. | Subject not relevant to orthodontics |
| 138. | Romanyukha A, Schauer DA, Malikov YK. Analysis of current assessments and perspectives of ESR tooth dosimetry for radiation dose reconstruction of the population residing near the Semipalatinsk nuclear test site. J Radiat Res (Tokyo). 2006 Feb; 47 Suppl A: A55-60. | Subject not relevant to orthodontics |
| 139. | Saito K, Hayakawa T, Kawabata R, Meguro D, Kasai K. Antibacterial activity and shear bond strength of 4-methacryloxyethyl trimellitate anhydride/methyl methacrylate-tri-n-butyl borane resin containing an antibacterial agent. Angle Orthodontist 2007; 77 (3), pp. 532-536. | Original study, not meta-analysis |
| 140. | Saito K, Sirirungrojying S, Meguro D, Hayakawa T, Kasai K. Bonding durability of using self-etching primer with 4-META/MMA-TBB resin cement to bond orthodontic brackets. Angle Orthodontist 2005; 75 (2), pp. 260-265. | Original study, not meta-analysis |
| 141. | Sánchez AR, Sheridan PJ, Kupp LI. Is platelet-rich plasma the perfect enhancement factor? A current review. Int J Oral Maxillofac Implants 2003 Jan-Feb; 18(1): 93-103. | Subject not relevant to orthodontics |
| 142. | Shaw WC, Mandall NA, Mattick CR. Ethical and scientific decision making in distraction osteogenesis. Cleft Palate Craniofac J 2002; 39: 641-5. | Systematic review |
| 143. | Shi Z, Guo C, Awad M. Hyaluronate for temporomandibular joint disorders. Cochrane Database of Systematic Reviews 2003, (1), Art. No.: CD002970. DOI: 10.1002/14651858.CD002970. | Subject not relevant to orthodontics |
| 144. | Sirirungrojying S, Hayakawa T, Saito, K, Meguro, D, Nemoto, K, Kasai K. Bonding durability between orthodontic brackets and human enamel treated with megabond self-etching primer using 4-META/MMA-TBB resin cement. Dental Mater J 2004; 23 (3), pp. 251-257. | Original study, not meta-analysis |
| 145. | Sirirungrojying S, Saito K, Hayakawa T, Kasai K. Efficacy of using self-etching primer with a 4-META/MMA-TBB resin cement in bonding orthodontic brackets to human enamel and effect of saliva contamination on shear bond strength. Angle Orthodontist 2004; 74 (2), pp. 251-258. | Original study, not meta-analysis |
| 146. | Skeggs R, Benson P. Surgical reinforcement of anchorage during orthodontic brace treatment. (Protocol) The Cochrane Database of Systematic Reviews 2005, Issue 1. Art. No: CD005098. DOI: 10.1002/14651858.CD005098 HANDSEARCHING!!!!! | Protocol for a Cochrane review |
| 147. | Skeggs RM, Benson PE, Dyer F. Reinforcement of anchorage during orthodontic brace treatment with implants or other surgical methods. Cochrane Database Syst Rev 2007 Jul 18; (3): CD005098. | Systematic review |
| 148. | Sonnesen L, Pallisgaard C, Kjær I. Cervical Column Morphology and Craniofacial Profiles in Monozygotic Twins. Twin Research and Human Genetics Vol. 11(1): 84-92. | Subject not relevant to orthodontics |
| 149. | Sood N, Baker WL, Coleman CI. Effect of glucomannan on plasma lipid and glucose concentrations, body weight, and blood pressure: systematic review and meta-analysis. Am J Clin Nutr 2008 Oct; 88(4): 1167-75. | Subject not relevant to orthodontics |
| 150. | Sprangers MAG, Sloan JA, Veenhoven R, Cleeland CS, Halyard MY, Abertnethy AP et al. The Establishment of the GENEQOL Consortium to Investigate the Genetic Disposition of Patient-Reported Quality-of-Life Outcomes. Twin Research and Human Genetics Vol. 12(3): 301-311. | Subject not relevant to orthodontics |
| 151. | Symington A, Pinelli J. Developmental care for promoting development and preventing morbidity in preterm infants. Cochrane Database Syst Rev 2000; (4): CD001814. Review. Update in: Cochrane Database Syst Rev 2001; (4): CD001814. | Subject not relevant to orthodontics |
| 152. | Symington A, Pinelli J. Developmental care for promoting development and preventing morbidity in preterm infants. Cochrane Database Syst Rev 2001; (4): CD001814. Review. Update in: Cochrane Database Syst Rev 2003; (4): CD001814. | Subject not relevant to orthodontics |
| 153. | Symington A, Pinelli J. Developmental care for promoting development and preventing morbidity in preterm infants. Cochrane Database Syst Rev 2003; (4): CD001814. Review. Update in: Cochrane Database Syst Rev 2006; (2): CD001814. | Subject not relevant to orthodontics |
| 154. | Symington A, Pinelli J. Developmental care for promoting development and preventing morbidity in preterm infants. Cochrane Database Syst Rev 2006 Apr 19; (2): CD001814. | Subject not relevant to orthodontics |
| 155. | Thomas DE, Elliott EJ, Naughton GA. Exercise for type 2 diabetes mellitus. Cochrane Database Syst Rev 2006; Jul 19; 3: CD002968. | Subject not relevant to orthodontics |
| 156. | Torlaschi, R. Orthodontics and periodontics: A meta-analysis | [Ortodonzia e parodonto: Una metanalisi]. Giornale dell'Odontoiatra 2008; 25 (13): pp. 23. | Short survey, not meta-analysis |
| 157. | Tsukiyama, Y., Baba, K., Clark, G.T. An evidence-based assessment of occlusal adjustment as a treatment for temporomandibular disorders. Journal of Prosthetic Dentistry 2001; 86 (1), pp. 57-66. | Narrative review |
| 158. | Tsuruoka, T., Namura, Y., Shimizu, N. Development of an easy-debonding orthodontic adhesive using thermal heating. Dental Mater J 2007; 26 (1), pp. 78-83. | Original study, not meta-analysis |
| 159. | Tuncay OC, Tulloch JF. Apparatus criticus: methods used to evaluate growth modification in Class II malocclusion. Am J Orthod Dentofacial Orthop 1992; 102: 531-6. | Comment on: Am J Orthod Dentofacial Orthop 1990; 98: 340-70. |
| 160. | van der Sanden WJ, Mettes TG, Grol R, Plasschaert AJ, Verdonschot EH. Topics in clinical dentistry. Trends in the Dutch dental literature. Ned Tijdschr Tandheelkd 1999; 106: 366-88. | Subject not relevant to orthodontics |
| 161. | Vidaeff AC, Yeomans ER. Corticosteroids for the syndrome of hemolysis, elevated liver enzymes, and low platelets (HELLP): what evidence? Minerva Ginecol 2007; Apr; 59(2): 183 90. | Subject not relevant to orthodontics |
| 162. | von Böhl M, Kuijpers-Jagtman AM. Hyalinization during orthodontic tooth movement: a systematic review on tissue reactions. Eur J Orthod 2009; Feb; 31(1): 30-6. Epub 2008 Dec 10. | Systematic review |
| 163. | Weston P, Yaziz YA, Moles DR, Needleman I. Occlusal interventions for periodontitis in adults. Cochrane Database Syst Re 2008; Jul 16; (3): CD004968. | Subject not relevant to orthodontics |
| 164. | Whelton SP, Chin A, Xin X, He J. Effect of aerobic exercise on blood pressure: a meta-analysis of randomized, controlled trials. Ann Intern Med 2002; Apr 2; 136(7): 493-503. | Subject not relevant to orthodontics |
| 165. | Wimmer G, Pihlstrom BL. A critical assessment of adverse pregnancy outcome and periodontal disease. J Clin Periodontol 2008; Sep; 35(8 Suppl): 380-97. | Subject not relevant to orthodontics |
| 166. | Yaegashi N, Niinuma T, Chisaka H, Watanabe T, Uehara S, Okamura K, Moffatt S, Sugamura K, Yajima A. The incidence of, and factors leading to, parvovirus B19-related hydrops fetalis following maternal infection; report of 10 cases and meta-analysis. J Infect 1998; Jul; 37(1): 28-35. | Subject not relevant to orthodontics |
| 167. | Yamada, T., Smith, D.C., Maijer, R. Tensile and shear bond strengths of orthodontic direct-bonding adhesives. Dental Materials 1988; 4 (5), pp. 243-250. | Original study, not meta-analysis |
| 168. | Yengopal V, Harnekar SY, Patel N, Siegfried N. Dental fillings for the treatment of caries in the primary dentition. Cochrane Database of Systematic Reviews 2009; (2), Art. No.: CD004483. DOI: 10.1002/14651858.CD004483.pub2. | Subject not relevant to orthodontics |
| 169. | Zachrisson, Y.O., Zachrisson, B.U., Büyükyilmaz, T. Surface preparation for orthodontic bonding to porcelain. American Journal of Orthodontics and Dentofacial Orthopedics 1996; 109 (4), pp. 420-430. | Original study, not meta-analysis |
| 170. | Zhang M, McGrath C, Hägg U. The impact of malocclusion and its treatment on quality of life: a literature review. Int J Paediatr Dent 2006; Nov; 16(6): 381-7. | Narrative review |

