All published articles of this journal are available on ScienceDirect.

Stunting and its Effects on Salivary Biomarkers and Oral Health: A Cross-sectional Analysis of Flow Rate, pH, and Buffering Capacity
Authors Info & Affiliations
Abstract
Aim
This study investigates the effects of stunting on salivary characteristics in children aged 6-12 years, focusing on salivary flow rate, pH, viscosity, and buffering capacity to assess oral health vulnerabilities linked to stunting.
Methods
A cross-sectional study was conducted with 72 elementary students in Padang, Indonesia, equally divided into stunted and normal-growth groups. Saliva samples were collected and analyzed for flow rate, pH, viscosity, and buffering capacity. Data were processed using SPSS version 27.
Results
Stunted children showed significant alterations in salivary parameters, including a reduced salivary flow rate (0.02 mL/min vs. 0.63 mL/min; p = 0.001) and lower pH (5.87 vs. 7.48; p = 0.001), indicating an acidic oral environment. Additionally, salivary viscosity was higher (1.88 cP vs. 1.07 cP; p = 0.001), and buffering capacity was lower (3.63 vs. 5.92; p = 0.001) in the stunted group, suggesting impaired salivary function.
Conclusion
The findings highlight that stunted children are at a greater risk of oral diseases due to compromised salivary function. Interventions using CPP-ACP, probiotics, xylitol, and stimulants like pineapple juice could help improve salivary health, underscoring the need for targeted oral health strategies in this vulnerable population.
1. INTRODUCTION
Stunting, a form of chronic malnutrition, has been a persistent public health issue, particularly in developing countries. It affects millions of children worldwide, leading to significant physical and cognitive impairments. Stunting is defined by a height-for-age z-score below -2 standard deviations from the World Health Organization (WHO) Child Growth Standards. This condition is not only a marker of poor nutrition but also of repeated infections during critical periods of growth. The consequences of stunting extend beyond childhood, with potential lifelong impacts on health, productivity, and economic development [1, 2]. In recent years, researchers have begun to explore the relationship between stunting and various aspects of health, including oral health, which remains an underexplored area of study [3].
Oral health is a critical component of overall health and well-being, yet it is often neglected in public health initiatives, particularly in low-resource settings. Saliva plays a crucial role in maintaining oral health through its functions in lubrication, buffering, and antimicrobial activity [4]. Changes in the quantity and quality of saliva can significantly affect oral health outcomes, including the development of dental caries, periodontal diseases, and other oral infections [5]. In children, particularly those who are stunted, these changes in salivary characteristics may exacerbate the risk of poor oral health outcomes, which not only causes discomfort but also affects productivity [6, 7]. The existing literature suggests that malnutrition, including stunting, can lead to alterations in salivary flow rate, viscosity, pH, and buffering capacity, which are essential in preventing the demineralization of teeth and protecting against oral diseases [8].
Previous studies have demonstrated a significant reduction in salivary flow rate among stunted individuals compared to their non-stunted counterparts. This reduction in salivary flow is concerning as it diminishes the protective functions of saliva, including its ability to wash away food particles and neutralize acids in the oral cavity [9]. Reduced salivary flow can lead to a higher accumulation of dental plaque, thereby increasing the risk of dental caries and other oral infections [10]. Additionally, the buffering capacity of saliva, which is essential for maintaining the pH balance in the mouth, is often compromised in stunted children. A decrease in buffering capacity makes it more difficult to neutralize the acids produced by cariogenic bacteria, further elevating the risk of dental erosion and caries [11].
Another critical aspect of saliva that is affected by stunting is its viscosity. Increased salivary viscosity has been associated with a decreased ability to lubricate the oral tissues and cleanse the mouth, which may lead to a higher prevalence of oral discomfort and disease [12]. Studies have shown that stunted children often have significantly higher salivary viscosity, which can impair their ability to swallow food properly and may contribute to further nutritional deficiencies [13]. This creates a vicious cycle where poor nutrition exacerbates oral health problems, which in turn further impairs the ability to consume a nutritious diet, perpetuating the cycle of malnutrition [14].
The relationship between stunting and oral health is further complicated by socio-economic factors. Poverty, food insecurity, and limited access to healthcare are significant determinants of both stunting and poor oral health. Addressing these underlying social determinants is essential for improving health outcomes in stunted populations. Interventions aimed at enhancing oral health in stunted children must, therefore, take a holistic approach, addressing not only the immediate dental needs but also the broader context of malnutrition and poverty [15].
There are limited explorations of the relationship between stunting and oral health, specifically in terms of salivary characteristics. While stunting is widely recognized as a public health issue with significant physical and cognitive consequences, its impact on oral health has received insufficient attention. Given the complexity of the relationship between stunting and oral health, there is a pressing need for further research to explore the underlying mechanisms and to develop effective interventions. This study aims to fill this gap by investigating the salivary characteristics of stunted children aged 6-12 years in West Sumatra, Indonesia. Specifically, the study will evaluate the salivary flow rate, viscosity, pH, and buffering capacity in stunted children and compare these parameters with those of non-stunted children. The findings of this study are expected to contribute to the understanding of how stunting affects oral health and to inform the development of targeted interventions to improve oral health outcomes in this vulnerable population [16].
The hypotheses being explored in this study are: (1) Stunted children have significantly lower salivary flow rates compared to non-stunted children; (2) stunted children exhibit higher salivary viscosity and lower buffering capacity, making them more susceptible to oral diseases; and (3) these changes in salivary characteristics are associated with an increased prevalence of dental caries and other oral health problems in stunted children [17]. The main goal of this study is to provide a comprehensive analysis of the salivary parameters in stunted children and to highlight the need for specific oral health interventions in this population [2].
This study is particularly important in the context of public health efforts to reduce the burden of stunting and its associated health outcomes. By identifying the specific oral health challenges faced by stunted children, this research will help to inform the development of comprehensive health programs that address both the nutritional and oral health needs of this vulnerable population [18]. Ultimately, this study aims to contribute to the global effort to improve the health and well-being of children affected by stunting, ensuring that they have the opportunity to lead healthy and productive lives.
2. MATERIAL AND METHODS
2.1. Research Design
This research is a descriptive, cross-sectional study conducted to investigate specific characteristics of saliva in elementary school children. The study aims to assess four primary salivary parameters—salivary flow rate, viscosity, pH, and buffering capacity—and to compare these parameters between stunted and normal-growth children. By focusing on these characteristics, the study provides insights into potential early indicators of salivary health in stunted children, serving as a preventive measure against the possible adverse impacts of stunting on salivary function.
2.2. Sampling Method and Study Population
The population of this study includes elementary school students aged 6-12 years from Padang, selected through purposive sampling. The samples were obtained with ethical approval from the Research Ethics Committee, Faculty of Medicine, Universitas Andalas, Indonesia, under the ethical code number 126/UN.16.2/KEP-FK/2024. This research was conducted on human subjects in accordance with the ethical principles outlined in the Helsinki Declaration of 1975, as revised in 2013. The sample size was calculated using a formula for comparing two independent groups with continuous variables, considering a significance level (α) of 0.05 and a power (1−β) of 0.90. As a result, a total of 72 students participated. Inclusion criteria were children aged 6–12 years, classified as either stunted or having normal growth based on the World Health Organization (WHO) growth standards. Stunted children were defined as having a height-for-age z-score of < -2 standard deviations, while children with normal growth had a height-for-age z-score of ≥ -2 standard deviations. Eligible participants were required to reside in the study area for a minimum of six months prior to the study, demonstrate overall good health apart from stunting, and provide written informed consent from parents or guardians along with assent from the child. Participants were also required to exhibit willingness and ability to cooperate during oral examinations and saliva collection.
Exclusion criteria included a history of systemic diseases or conditions known to affect salivary function, such as diabetes or Sjögren’s syndrome. Children who had used medications that could alter salivary flow or composition, including antihistamines or antidepressants, or who had undergone antibiotic or immunomodulatory treatment within the past three months, were excluded. These criteria were carefully designed to ensure the selection of a homogenous study population and to minimize confounding factors that could influence salivary biomarkers or oral health outcomes.
2.3. Group Allocation
Participants were divided equally into two distinct groups to facilitate a comparative analysis. Of the 72 students, 36 were classified in the stunted group, and 36 were classified in the normal group. Stunting was determined based on the WHO Z-Score Table, with children having a height below -2 SD (standard deviation) categorized as stunted. This allocation allows for a direct comparison of salivary characteristics between stunted and normally growing children, enabling a more detailed examination of any differences that may be associated with growth delays.
2.4. Data Collection Procedure
Data collection involved the careful measurement and evaluation of unstimulated saliva to determine the targeted salivary parameters. Saliva was collected using the passive drooling method, which is widely regarded as the gold standard for collecting unstimulated saliva due to its ability to preserve the natural composition of the sample without introducing external stimulants. During the process, subjects were seated comfortably with their heads slightly tilted forward. They were instructed to relax their oral muscles and refrain from swallowing while allowing saliva to accumulate passively on the floor of the mouth. Once sufficient saliva had pooled, subjects gently drooled into a sterilized funnel connected to a microtube without applying any external pressure, such as spitting or suction.
This method reduces variability caused by mechanical or gustatory stimulation and ensures a more consistent representation of basal salivary function. All samples were collected between 9:30 AM and 11:30 AM to minimize circadian variability, which can influence salivary parameters, such as pH and flow rate. Subjects were instructed to abstain from eating, drinking, smoking, or brushing their teeth for at least one hour before collection to ensure sample integrity. They were also advised to avoid intense physical activity and acidic or spicy foods the evening prior to saliva collection.
Salivary pH was measured immediately using a calibrated digital pH meter, buffering capacity was assessed using standardized Check Buffer Kits, and viscosity was measured with a viscometer to determine the fluid’s flow characteristics accurately. Each step was performed under controlled conditions, with strict adherence to standardized protocols to ensure reliability and comparability across all participants.
2.5. Data Analysis
The collected data were processed using SPSS version 27, following a structured sequence that included data checking, coding, entry, and cleaning. Data were subjected to univariate analysis to identify trends and characteristics within the sample groups. This approach allowed for a systematic comparison of salivary flow rate, viscosity, pH, and buffering capacity, providing a clear analysis of how these parameters differ between stunted and normally growing children. Through this analytical process, the study contributes valuable findings on the relationship between stunting and salivary function, with potential implications for early detection and intervention strategies.
3. RESULTS
The results of this study provide a detailed examination of the salivary parameters in both stunted and non-stunted children, focusing on key factors, such as salivary flow rate, pH, viscosity, and buffering capacity. Statistical analysis revealed significant differences between the two groups, highlighting the potential impact of stunting on oral health. The following sections present the findings of these parameters, demonstrating the variations observed and their potential implications for oral health management in children with stunting. Each parameter is discussed in relation to its physiological role and the observed deviations in the stunted population.
The comparison of salivary flow rate between the normal and stunting groups (Table 1) reveals a significant reduction in the flow rate among the stunted individuals (Mean = 0.02, SD = 0.004) compared to the normal group (Mean = 0.63, SD = 0.12), with a p-value of 0.001. This significant decrease in salivary flow rate in the stunting group suggests that stunting may be associated with impaired salivary gland function, potentially contributing to an increased risk of oral health issues due to inadequate saliva production.
As shown in Fig. (1), the salivary pH is significantly lower in the stunting group (Mean = 5.87, SD = 0.22) compared to the normal group (Mean = 7.48, SD = 0.35), with a p-value of 0.001. The decrease in salivary pH among stunted individuals indicates a shift towards more acidic conditions in the oral environment, which may increase susceptibility to dental caries and other acid-related oral pathologies.
| Groups | N | Mean | SD | p-value |
|---|---|---|---|---|
| Normal | 36 | 0.63 | 0.12 | 0.001 |
| Stunting | 36 | 0.02 | 0.004 |
The analysis of salivary viscosity (Fig. 2) demonstrates a marked increase in viscosity in the stunting group (Mean = 1.88, SD = 0.02) compared to the normal group (Mean = 1.07, SD = 0.03), with a statistically significant p-value of 0.001. Elevated salivary viscosity in stunted individuals could further exacerbate oral health challenges by reducing the effectiveness of saliva in lubricating and cleansing the oral cavity, thus impairing its protective functions.
Table 2 illustrates a significant reduction in salivary buffer capacity in the stunting group (Mean = 3.63, SD = 0.12) when compared to the normal group (Mean = 5.92, SD = 1.37), with a p-value of 0.001. The diminished buffering capacity observed in stunted individuals suggests a compromised ability to neutralize acids in the oral environment, which may contribute to an increased risk of dental erosion and caries development.
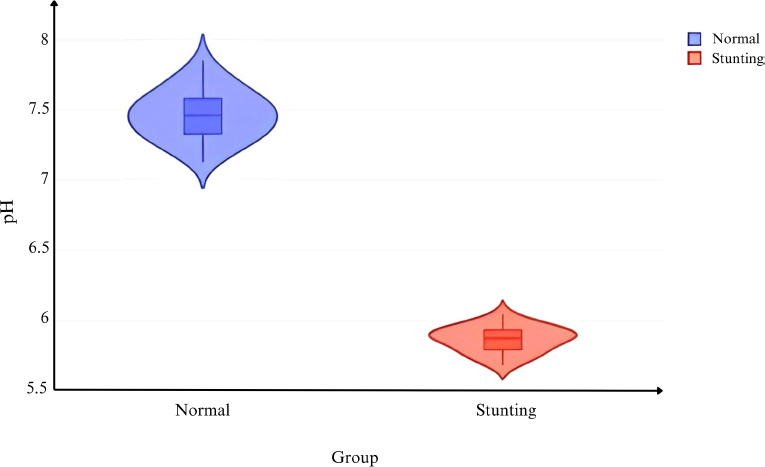
Comparison of salivary pH levels between normal and stunted children.
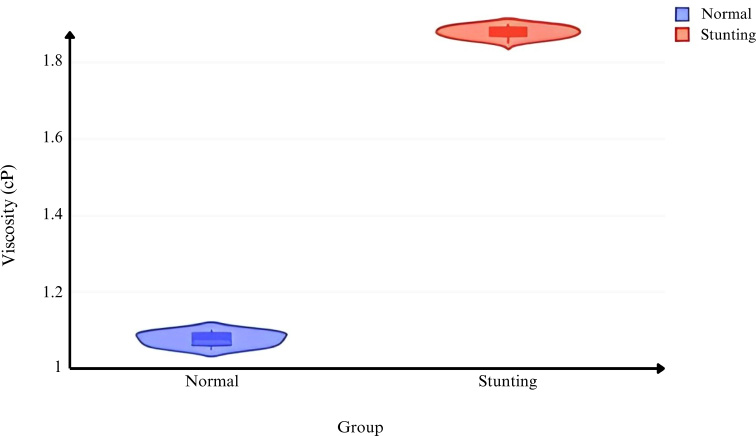
Comparison of salivary viscosity values between the groups.
4. DISCUSSION
The present study offers an in-depth assessment of the effect of stunting on the salivary parameters, which are crucial to the maintenance of oral health [19]. The parameters being considered are saliva flow rate, pH, viscosity, and buffering capacity. This controlled laboratory study was aimed at comparing two groups of children: those who were well-grown and children with evident stunting. Such information provides a great understanding of the effects of stunting on the oral environment as well as their risk susceptibility to a number of oral health conditions. This discussion, therefore, seeks to situate these findings within the current body of evidence and assess what could be some of the mechanisms available and the possible ramifications for oral care in stunted populations.
| Groups | N | Mean | SD | p-value |
|---|---|---|---|---|
| Normal | 36 | 5.92 | 1.37 | 0.001 |
| Stunting | 36 | 3.63 | 0.12 |
4.1. Salivary Flow Rate and its Implications
Management of saliva secretion phenomena is crucial as saliva plays an important role in units of oral hygiene, as its decrease has been related to the development of dental caries, periodontitis, and other diseases [5]. The study shows a remarkable drop in the amount of saliva produced by stunted individuals, averaging 0.02 mL/min, which is a record low as opposed to normal group figures of 0.63 mL/min (p = 0.001) for patients with normal nutritional status. This shows that there is a loss of function in the salivary glands and that could result from malnutrition or other systemic factors relating to stunting [3]. It ensures that there is enough saliva to cleanse the oral cavity and thereby reduces the chances of bacterial proliferation and plaque buildup, which predispose one to more severe oral diseases [6].
4.2. The Shift in Salivary pH and Oral Health Risks
The study also highlights a significant decrease in salivary pH among stunted individuals, with a mean pH of 5.87 compared to 7.48 in the normal group (p = 0.001). Oral salivary pH helps sustain the acid-neutralizing ability of saliva, thus preventing de-remineralization and related dental caries. Increased exposure of the enamel of stunted subjects to acidic pH could propose a higher chance of wearing down the enamel and developing caries. This acidic condition enhances the growth of the aforementioned acidogenic bacteria, which might facilitate dental caries [9].
4.3. Increased Salivary Viscosity and its Consequences
Salivary viscosity is another critical parameter that influences the protective functions of saliva. The study shows that in the stunted group, salivary viscosity has a higher value (Mean = 1.88 cP) than in the normal group (Mean = 1.07 cP) with a p-value of 0.001. Salivary viscosity in excess may compromise the lubricating and self-cleaning function of saliva in the oral cavity, making it less effective in protecting the mucosa and teeth against wear and bacterial infestations. Also, high viscosity may limit the ability to properly swallow food, leading to food intake limitations, which will cause more nutritional deficiency. Such results are in accordance with studies that expect a positive association between salivary viscosity and oral discomfort and diseases [12-14].
4.4. Decreased Salivary Buffering Capacity and Acid Neutralization
A lack of buffering capability in saliva increases the risk of acid erosion and caries because there is no recovery from the state of conditioning [7]. In the research, it was found that stunted individuals have a considerable decrease of 3.631 salivary buffering capacity, while normal individuals have a mean value of 5.921 (p = 0.001). This reduced capability implies that based on the high acidic content of the oral environment of the stunted individuals, they will be more prone to diseases that are caused by high acidity in the mouth [11]. Nutritional deficits due to stunting are hypothesized to be the cause of the decrease in buffering capability, where even the bicarbonate ions necessary for the buffering action would be reduced [15].
4.5. Potential Mechanisms Underlying Altered Salivary Parameters in Stunted Individuals
The changes in some salivary parameters in the stunted individuals might also be due to some other reasons. Since stunting is often linked to malnutrition, the latter can result in underdevelopment of the salivary gland, resulting in a lack of hormones that are necessary for optimum salivary production [3]. In addition, the repeated but low-grade swelling that often comes with stunting may lead to the loss of these salivary glands’ functionalities, hence causing a decrease in the amount of salivary secretion as well as its buffering action. Hormones-related factors that are induced by stunting may equally be responsible for the changes noted in secretion, both in composition and quantity [16, 17].
4.6. Implications for Oral Health Management in Stunted Populations
Stunted children experience significant oral health challenges, partly due to compromised salivary composition, an essential factor in maintaining oral health. Saliva plays a crucial role in buffering acids, controlling bacterial growth, and facilitating tooth remineralization [19]. Research by Nerawati et al. reveals that stunted children show higher Streptococcus mutans levels and an elevated DMF-T (Decayed, Missing, Filled Teeth) index, indicating greater caries susceptibility likely due to altered salivary function and immune response [20].
Fitri et al. found that stunted children had poorer oral hygiene, as reflected in elevated OHI-S scores, exacerbating risks of periodontal issues. Delays in tooth eruption, as observed by Wulandari et al., also relate to nutritional deficiencies that impact salivary and bone health [21, 22]. Syafitri et al. demonstrated that altered salivary RANKL levels contribute to persistent primary teeth [23]. These findings emphasize the importance of saliva in supporting oral health, underscoring the need for integrative care focusing on both nutrition and oral hygiene in stunted children.
The results from this study highlight the necessity of designing specific oral health interventions in stunted populations. The intervention of food products containing Casein Phosphopeptide Amorphous Calcium Phosphate (CPP-ACP), probiotics, and xylitol in the form of chewing gum can be administered to address saliva-related issues [24, 25].
Casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) is an effective sugar-free anti-cariogenic agent derived from the milk protein casein, in combination with calcium phosphate. The unique sequence of Ser(P)-Ser(P)-Ser(P)-Glu-Glu in CPP-ACP plays a crucial role in maintaining the stability of calcium phosphate ions, thereby facilitating the remineralization process. In addition to enhancing salivary pH and buffering capacity, CPP-ACP disrupts plaque formation by competing for calcium ions, which are essential for bacterial adhesion within the dental plaque matrix [24, 26].
Probiotics exert an inhibitory effect on pathogenic bacterial environments by competing for host tissue binding sites and essential nutrients, such as carbohydrates, commonly utilized by pathogens, thereby reducing acid production. In vitro studies have identified Lactobacillus acidophilus as the most suitable species for formulating a novel probiotic chewing gum. This advanced technology ensures the probiotic's survival during processing, its stability without refrigeration, its extended shelf life, and its adherence to consumer preferences regarding taste, texture, color, and odor. Upon release in the oral cavity, the probiotic produces compounds that combat Streptococcus mutans, a major pathogen responsible for dental caries. Notably, the action of probiotic gum is localized within the mouth, without systemic effects, which typically require probiotic adhesion in the intestines [25].
Xylitol, a non-fermentable sugar alcohol, has been shown to reduce Streptococcus mutans levels by disrupting the organism's energy cycle through a suicidal mechanism involving the dephosphorylation of xylitol-5-phosphate. Moreover, xylitol in chewing gum enhances salivary flow due to its sweet taste and strengthens the salivary defense mechanisms by raising pH and improving buffering capacity. By accelerating the clearance of acids and promoting the uptake of calcium phosphate, xylitol-containing gum indirectly facilitates enamel remineralization. Additionally, xylitol offers the benefit of substituting cariogenic sugars in the diet, further reducing the risk of dental caries. Children aged 3-5 years are vulnerable to early childhood caries [24, 27].
In addition to chewing gum that mechanically stimulates saliva, the general population can also stimulate saliva chemically. One chemical stimulant that can be used is pineapple juice. The acidic chemical stimulus in pineapple is a potent inducer of increased saliva secretion [28]. Pineapple contains the enzyme bromelain, dextrose, levulose, mannitol, sucrose, ergosterol peroxide, ananasic acid, sugars, and organic acids [29]. One of the main organic acids in pineapple is citric acid, which constitutes 87% of the total acids present in the fruit [30]. The pure citric acid content in 100 ml and 200 ml of fresh pineapple juice is 0.0350 g and 0.0466 g, respectively [31].
4.7. Key Findings
The key findings of the study are as follows:
4.7.1. Significant Reduction in Salivary Flow Rate
Stunted children exhibited a substantially lower salivary flow rate (Mean = 0.02 mL/min) compared to their normally growing counterparts (Mean = 0.63 mL/min, p = 0.001). This reduction may indicate impaired salivary gland function, increasing vulnerability to oral health issues, such as dental caries and periodontal disease.
4.7.2. Acidic Oral Environment in Stunted Children
The salivary pH of stunted children was significantly lower (Mean = 5.87) compared to the normal group (Mean = 7.48, p = 0.001), reflecting an acidic oral environment. This condition predisposes stunted individuals to enamel demineralization and caries.
4.7.3. Elevated Salivary Viscosity
Stunted children showed higher salivary viscosity (Mean = 1.88 cP) compared to the normal group (Mean = 1.07 cP, p = 0.001). This elevated viscosity likely impairs the protective and self-cleansing functions of saliva, compounding the risk of oral discomfort and disease.
4.7.4. Decreased Buffering Capacity
The buffering capacity of saliva was markedly lower in the stunted group (Mean = 3.63) compared to the normal group (Mean = 5.92, p = 0.001). This reduction compromises the ability to neutralize oral acids, increasing the risk of dental erosion and caries development.
4.8. Strengths
The strengths of the study are as follows:
4.8.1. Comprehensive Salivary Analysis
The study provides a detailed examination of four critical salivary parameters—flow rate, pH, viscosity, and buffering capacity—offering a holistic view of how stunting impacts salivary function.
4.8.2. Robust Study Design
The use of a cross-sectional design with equal representation of stunted and normal-growth groups enhances the reliability of the comparative analysis.
4.8.3. Standardized Data Collection Methods
The passive drooling method, coupled with precise laboratory analyses (digital pH meter, viscometer, and buffering kits), ensures high accuracy and reliability of the data.
4.9. Weaknesses
The weaknesses of the study are as follows:
4.9.1. Cross-sectional Design
While valuable for identifying associations, the cross-sectional nature of the study limits causal inference. Longitudinal studies are needed to establish cause-and-effect relationships between stunting and salivary dysfunction.
4.9.2. Limited Generalizability
The study population was restricted to elementary school students in Padang, Indonesia. Results may not be directly applicable to other regions or demographic groups with differing socioeconomic or environmental conditions.
4.9.3. Lack of Dietary and Lifestyle Data
The study did not account for individual dietary habits, oral hygiene practices, or environmental factors that may influence salivary parameters, potentially confounding the results.
CONCLUSION
This study provides a comprehensive analysis of the effects of stunting on salivary parameters, highlighting significant alterations in saliva flow rate, pH, viscosity, and buffering capacity. Stunted children exhibit markedly reduced salivary flow and pH, accompanied by increased viscosity and diminished buffering capacity, all of which heighten their susceptibility to oral diseases, such as dental caries and enamel erosion. The findings suggest that nutritional deficits associated with stunting may impair salivary gland function, resulting in diminished protective properties of saliva.
Interventions, such as the use of CPP-ACP, probiotics, and xylitol in chewing gum formulations, are promising approaches for mitigating these oral health challenges by enhancing saliva composition and functionality. Furthermore, chemical stimulants like pineapple juice may serve as an additional method to improve saliva secretion and oral health in stunted populations. These insights underscore the necessity of tailored oral health strategies for stunted individuals to address their unique vulnerabilities and enhance their overall oral care outcomes.
AUTHORS’ CONTRIBUTION
D.G.A.N. and N.K.: Study conception and design were contributed; R.W.W. and H.A.: Data collection was performed; D.R., I.S., D.R.J., and G.E.: Analysis and interpretation of results were performed; and B., M.D.S.E., T.R.W., and F.A.A.: Manuscript was drafted. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| WHO | = World Health Organization |
| CPP-ACP | = Casein Phosphopeptide Amorphous Calcium Phosphate |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The samples were obtained with ethical approval from the Research Ethics Committee, Faculty of Medicine, Universitas Andalas, Indonesia, under the ethical code number 126/UN.16.2/KEP-FK/2024.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent from parents or guardians, along with assent from the child, was taken.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article are available within the article.
FUNDING
This research was financially supported by BIMA Kemendikbud, 041/E5/PG.02.00.PL/2024 and 69/UN16.19/PT.01.03/PL/2024. The funding was allocated for data collection, laboratory analysis, or manuscript preparation, enabling comprehensive investigation of the salivary characteristics of stunted children. The sponsor had no involvement in study design, data interpretation, or manuscript writing.
ACKNOWLEDGEMENTS
The authors would like to express their gratitude to the Faculty of Medicine and Faculty of Dentistry of Andalas University, Indonesia for providing facilities essential for data collection and analysis. We are also grateful to the participating children and their families for their invaluable cooperation in this research.

