All published articles of this journal are available on ScienceDirect.

Management of Unilateral Impacted Maxillary Permanent Canine: A Case Report
Abstract
Introduction
The management of maxillary canine is very complex because it must be carefully planned and carried out as a team. The handling of impacted canine cases must be seen from a clinical and radiological point of view. Maxillary canine impaction can be caused by a lack of space or inadequate seed placement. The time to treat canine impaction is usually between the ages of 11 and 14.
Objective
The aim of this case report was to describe the management of an impacted maxillary left canine of a teenage girl. Successful treatment requires complete diagnostics, such as radiographs, good teamwork, and precise treatment planning of the dental team.
Case Report
An 11-year-old female patient with class I molar relationship, bimaxillary protrusive, and impacted left upper canine visited the clinic for orthodontic treatment. Extraction of four first premolars (bicuspids) was carried out, and exposure by the periodontist was completed on the maxillary left canine for the installation of a traction device (gold chain traction).
Conclusion
The appropriate timing, treatment plan, and proper surgical exposure preparation in handling this case produced optimal and ideal results.
1. INTRODUCTION
Treatment of impacted teeth is very complex and requires careful multidisciplinary planning. Not every impacted tooth can be maintained to get an ideal occlusion. In some scenarios, the impacted tooth must be sacrificed for various reasons. Comprehensive data collection and careful analysis must be performed to correctly plan the treatment of impacted dentition cases. Impacted teeth or delayed tooth eruption is the eruption time of the teeth that radically differs from the normal time for every race, ethnicity, and gender. The prevalence of canine impaction rates is between 1%-3%, and it is the second most common impaction after third molars impaction [1-6]. Canine impaction is twice as common in females than in males [7]. Palatal impaction (about 2/3) is more common than labial impaction (about 1/3), and maxillary impaction is more common than mandibular impaction [8]. The main etiology for canine impaction is unknown and could be caused by multiple factors, such as arch length discrepancy, failure of primary canine resorption, prolonged retention of the primary canine, dilaceration of the roots, and many more [6-9].
1.1. Radiographic Verification of Crown Position
In order to evaluate the exact position of the impacted canine, the clinician must use a radiograph. Several radiographic methods evaluate the position of impacted canines, including periapical film, occlusal film, panoramic radiograph, lateral cephalogram, and the recent Cone Beam Computed Tomography (CBCT) or 3D X-ray [10]. Prior to the invention of CBCT, periapical films were widely used to determine the exact position of the impacted canine. In a work, two periapical films with the tube-shift method were used, and the SLOB (Same Lingual; Opposite Buccal) rule was applied to determine the exact position of the impacted canine [11, 12]. The SLOB rule has been widely used around the world. When an object moves in the same direction as the x-ray, the tooth is located on the lingual of the other object, while if the object moves to the opposite side, it is located on the buccal of the other object. With the availability of CBCT, clinicians could now accurately localize the exact position of the impacted canine by just taking a single radiograph. An additional advantage of the CBCT is that the clinician could further assess any possible root damage to the adjacent teeth and plan the mechanics needed to bring the impacted canine into occlusion.
1.2. Palatal Impaction
Palatal impaction of the maxillary canine is the most common problem encountered by an orthodontist compared to labial impaction of the maxillary canine [3]. Many studies have determined the treatment of palatally impacted maxillary canines, most commonly those of Ericson and Kurol [8]. Once a radiograph is taken, the clinician should see the position of the impacted maxillary canine in relation to the adjacent teeth (lateral and central incisors) [8, 10]. Certain positions of ectopically displaced permanent maxillary canines could be resolved only by extracting deciduous maxillary canines and monitoring the progress for several months. Ericson and Kurol suggested that 91% of the time, the canine will normalize over time if the root of the canine is hovering around the root of the maxillary lateral incisors [8-10]. However, in situations where the maxillary permanent canine is positioned past the roots of the lateral incisor, the percentage may decrease significantly from 91% to about 64%, and additional treatment, such as exposure and uncovering by other dental specialists (oral surgeon or periodontists), may be needed. Orthodontists can then need to strategically guide the canine into position. Improper uncovering of the impacted canine can increase orthodontists' difficulty with treatment. Ideally, the impacted canine should be uncovered within the first six to nine months of treatment once sequential archwires have been placed. During exposure appointment, a large rectangular archwire (e.g., .019 x .025 stainless steel) should be used to prevent any side effects of treatment. Continuous discussion and planning with the oral surgeon or periodontist should be done to maximize treatment time. Not long after the surgery, the orthodontist should then move the permanent canine into the arch or the prepared edentulous site. In a situation where the maxillary canine is ankylosed, then extraction of the canine should be completed, and an alternative treatment plan should be discussed with the patient. This number is very low for young patients aged between 12-16 years, but the number increases with adult patients [11-13].
1.3. Labial Impaction
In labial impaction, the most common cause is insufficient space for eruption [1]. This leads to shifting the maxillary midline or ectopic migration of the canine over the root of the lateral incisor or first premolar. Opening the space for the maxillary canine using routine orthodontic mechanics might allow spontaneous eruption [4]. In the case of labial impaction, the amount of attached gingiva present in the eruption area should be considered as this will affect the posttreatment aesthetic outcome. Ideally, there should be about 2-3 mm of attached gingiva for best treatment outcome. The treatment mechanic may also impact the treatment result. The following three techniques are recommended: excisional uncovering, apically positioned flap, and closed eruption techniques, which may help with treatment results [6].
2. TREATMENT OBJECTIVE
This case report aimed to discuss the management and treatment of unilateral impaction of the left maxillary canine of a female patient treated in our clinic. Successful treatment results require good teamwork and precise and careful treatment planning.
3. CASE REPORT
An 11-year-old female patient visited our clinic with a chief complaint: “My upper teeth are sticking out, and my left maxillary canine is missing, as was told by my dentist.” Anamnesis showed that her deciduous maxillary left canine was still intact and had no sign of mobility. The patient did not report early loss of primary dentition and had no significant medical condition.
An extraoral examination revealed the patient to have a bimaxillary protrusion with a convex profile and lip fullness. Intraoral examination revealed that the patient had all her permanent dentition in occlusion except her second molar, third molar, and left maxillary canine. Mild to moderate rotation and crowding were seen in her maxillary dentition. The left maxillary canine was not palpable. The patient had a class I molar and canine relationship. The midline was not incidental. The patient had normal overbite (1mm) and overjet (1mm) (Fig. 1).
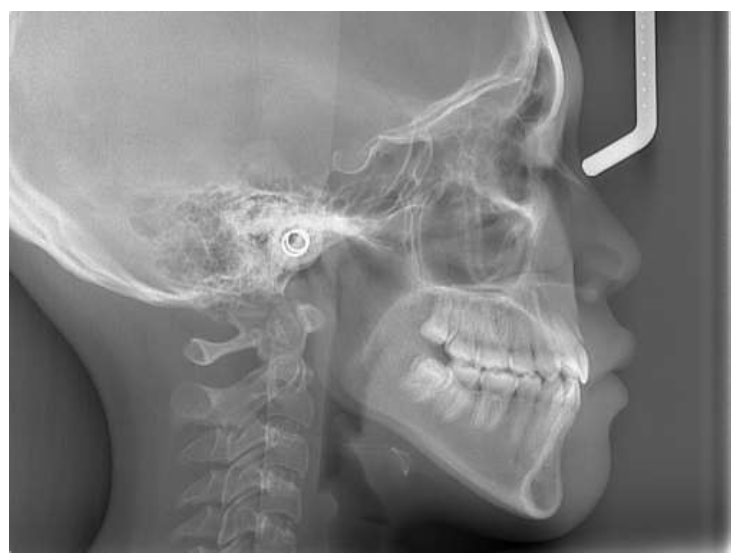
The cephalometric radiograph suggested the patient to have class I malocclusion with bimaxillary protrusion (Fig. 2). The panoramic radiograph showed the maxillary left deciduous canine to still be present. The permanent maxillary left canine was impacted very high up, buccally or palatally, and between the maxillary lateral incisor and first premolar (Fig. 3). The root of the deciduous canine was still fully intact. After waiting and monitoring for several months, no changes were seen to determine if the permanent canine position would improve.
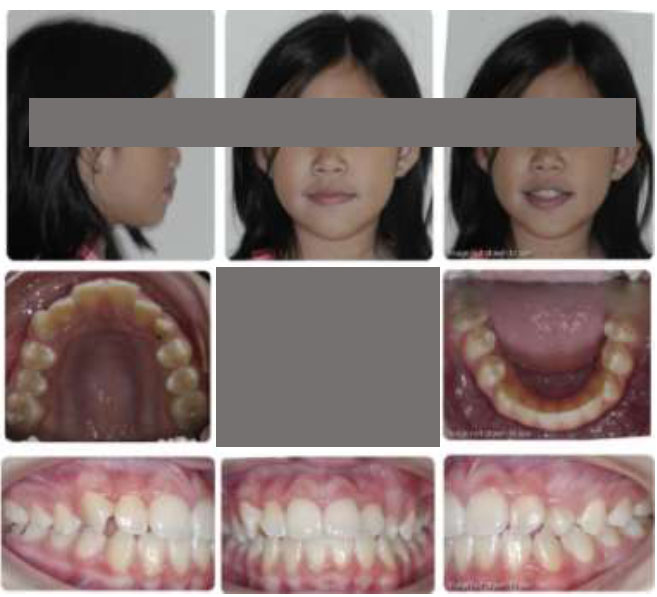
Pretreatment intra and extraoral photography.

Pretreatment cephalometric radiograph.
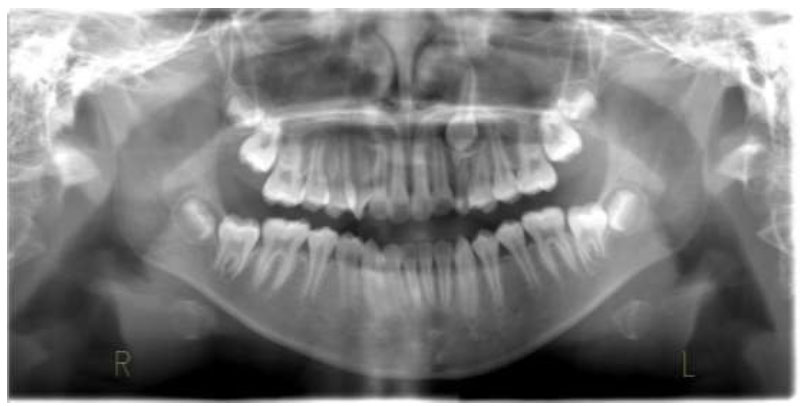
Pretreatment panoramic radiograph.
Several treatment options, with pros and cons, were given to the patient and her family. The informed signed consent for treatment was obtained. The treatment plan involved the extraction of the four first premolars to relieve the bimaxillary protrusion and surgical exposure and traction using a gold chain to bring down the maxillary permanent left canine to normal class I occlusion (Fig. 4).

Progress treatment intra and extra-photography.
Treatment was completed, and the maxillary permanent left canine was guided down to normal occlusion (Figs. 5-7).

Posttreatment intra and extra-oral photography.
Posttreatment cephalometry radiograph.

Posttreatment panoramic radiograph.
4. DISCUSSION
The patient visited the clinic with the chief complaint that her front teeth are sticking out and her maxillary permanent left canine has not erupted. Clinical and radiographic examination showed that the patient had a bimaxillary protrusion, and her maxillary permanent left canine was still impacted. After consultation with the patient and parents, along with educating them regarding the finding, it was decided that there would be extraction of the four first premolars to relieve the bimaxillary protrusion and extraction of deciduous maxillary left canine, followed by surgical traction using a gold chain attached to the maxillary left permanent canine to help the eruption of the permanent canine.
The biggest concerns during the traction of the impacted canine to normal occlusion are eruption failure (ankylosis) and possible root resorption [14]. The second biggest concern is the periodontal and gingival status around the canine area once it is in occlusion [15]. The advantage of performing traction is that the treatment will be finished post-orthodontic management without the need for any additional treatment, such as permanent restoration, which will also save cost and time. For this case alone, another concern was the gold chain's disengagement due to the impacted canine's high position. In this case, a second exposure was needed as the clinician decided to perform a closed exposure.
For this case, the movement of the maxillary impacted canine through the cortical bone demanded heavy anchorage control. A slower rate of tooth movement was needed to prevent root resorption. Extraction of the four first premolars and retraction of the anterior teeth were done first to eliminate the bimaxillary protrusion. Surgical exposure of the maxillary left impacted canine was completed afterward. The patient was very satisfied with the result even though the treatment took slightly longer than usual due to slow movement. The patient’s treatment led to class I occlusion and a nice smile. However, additional finishing remained to be completed.
Treatment of impacted teeth needs to be handled carefully taking into account full diagnostic records to prevent prolonging the treatment and damaging the roots of the teeth [16].
CONCLUSION
Any treatment dealing with tooth impaction needs to be handled very carefully. In the majority of situations, appropriate surgical procedures and the timing for exposure of the impacted canine need to be determined by considering several criteria. Successful results require teamwork and an interdisciplinary approach that includes a team of orthodontists, periodontists, and oral surgeons. The patient and parents need to be informed regarding the procedure's difficulty and time frame.
AUTHORS’ CONTRIBUTION
HH contributed to the treatment of the patient by providing complete initial, progress, and final treatment photos and radiographs. HH initiated the case report and provided the final approval for the manuscript. IAH contributed to data collection towards the end of the treatment, literature review, and completion/revision of the manuscript.
ABBREVIATION
| CBCT | = Cone Beam Computed Tomography |

