All published articles of this journal are available on ScienceDirect.

Detection of Caries Coronal Condition Prevalence of Permanent Teeth in Children using the International Caries Detection and Assessment System for Measuring Dental Caries: A Cross-sectional Study
Authors Info & Affiliations
Abstract
Background
The International Caries Detection and Assessment System (ICDAS) is a clinical scoring system for use in dentistry education, clinical practice, research, and epidemiology, and provides a framework to support and facilitate comprehensive caries care to improve long-term health outcomes for children.
Objective
To detect coronal caries in children using ICDAS for measuring dental caries to support and facilitate comprehensive caries care to improve long-term health outcomes for children.
Methods
Cross-sectional observational study designs were used for population-based surveys with detection codes for coronal caries according to ICDAS. Sampling techniques were used for purposive sampling, with sample size being used as the adequate sample size in the prevalence study. The sample consisted of 210 students from Puteran village in Tasikmalaya district, West Java, Indonesia, who met the inclusion and exclusion criteria. The data were analyzed using distribution frequency and the prevalence rate formula.
Results
The ICDAS assessment showed a caries prevalence of 91.4% among permanent teeth in children aged 6 to 12 years. The prevalence of caries is higher in the mandible than in the maxilla. At these ages, the majority of ICDAS assessments are code 1, and the percentage value of caries is higher in ICDAS code 1 than in codes 2 to 6. The trend of decreasing numbers indicates that the percentage value of ICDAS decreases from code 1 to code 5, which represents the most severe condition of caries. The teeth with the most caries detected in the upper jaw are teeth 16, 26, and in the lower jaw are teeth 31, 36, 41, and 46.
Conclusion
The ICDAS evaluation revealed a caries prevalence of 91.4% for permanent teeth. The mandible has a higher prevalence of caries than the maxilla. Code 1 is the most frequent ICDAS assessment code. There is a decrease in the percentage value of ICDAS from code 1 to code 5, which is the code with the most severe caries condition.
1. INTRODUCTION
Teeth play an important role in chewing, speaking, facial growth and development and aesthetic appearance [1]. Dental caries is a complex disease in the dental public health area [2, 3], and it is essential to know that the condition can manifest in a variety of ways [2]. It is necessary to prevent tooth decay caused by dental caries. Dental caries in children can cause various complications such as pain and discomfort, tooth loss, acute and chronic infections, sleep and eating disorders, absence from school, decreased learning ability, decreased appetite, weight loss and decreased growth rate, as well as having an impact on reducing the quality of life of children and their families [1].
During the past decade, several measurement criteria for detecting dental caries have been created [2]. Key issues in management prevention of dental caries, specifically the control of tooth decay, is prevalent in nearly all regions [2, 4]. ICDAS was created to improve oral health assessment and plan implementation of its solutions using a new paradigm, particularly regarding managing dental caries, to understand the process, disease, and prevention, and to provide optimal oral health for society [2].
Managing dental caries in children is essential. The management of caries in primary teeth requires the least invasive caries management strategy [5], taking into account the timing of or absence of infection, the maintenance of tooth structure, the number of affected teeth, and efforts to prevent anxiety due to tooth decay [5]. Caries management for children with carious lesions on permanent teeth involves the least invasive caries management plan that takes into account the location and size of the lesion, the risk of infection, the preservation of tooth structure [5], the health of the dental pulp, the avoidance of anxiety caused by treatment, the lifetime prognosis of the tooth, and consideration of orthodontic as well as occlusal development [5].
A growing number of national surveys [6], which serve as the primary source of statistics on public oral health, must be simplified into comprehensive country health survey programs [7]. The FDI World Dental Federation [6] offers a global consultative approach to evaluate the challenges and potential consequences of establishing a preventative strategy employing ICDAS as a tool for the management of caries [7]. In addition to avoiding the onset of disease and stopping the progression of carious lesions, preventive measures aim to lessen the need for restorations [6].
The ICDAS criteria were created by an international caries research team to integrate various new criteria systems into one standard approach for caries detection and assessment. The ICDAS is a clinical scoring system for use in dentistry education, clinical practice, research, and epidemiology and provides a framework to support and facilitate comprehensive caries care to improve long-term health outcomes [7].
The ICDAS provides a flexible, internationally accepted system for defining all of the stages of the caries process and the lesion's activity, which may be included within the International Caries Classification and Management System (ICCMS) [2]. The ICCMS provides an option for dentists to integrate and synthesize patient oral health information, including caries risk result assessments, in order to plan, manage, and review caries in clinical practice and public health [2] addressing all required dental diagnostic, preventative, and therapeutic decisions [2].
Puteran Subdistrict is one of the rural areas in Tasikmalaya District that has been the subject of education from multiple parties over the past five years, but it has not been conducted regularly and has never been evaluated, so it is crucial to conduct research and develop a caries management plan for the children in that area. A caries management plan for the children in Puteran village can be started by measuring the condition of dental caries using ICDAS.
ICDAS has established a novel measurement paradigm for dental caries based on a previous systematic review analysis of caries detection systems and other sources. The ICDAS can serve as the basis and guideline for clinical and epidemiological research, as well as direct undergraduate and graduate dentistry education in Cariology. The ICDAS method was created to increase the understanding of dental caries initiation and progression in epidemiologic and clinical research [8].
The reason for the research focus on children aged 6-12 years is because the age of 6-12 years is an identified age indicator for policy formulation, target setting, and monitoring at the global, regional, and national levels and is a relevant indicator for use in oral health surveillance that must be linked to with standard age groups [4]. This study aims to detect coronal caries in children using ICDAS for measuring dental caries to support and facilitate comprehensive caries care to improve long-term health outcomes for children.
2. METHOD
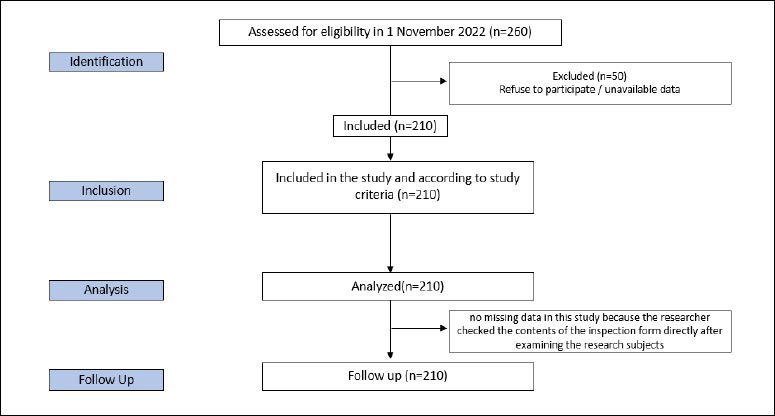
A cross-sectional observational study design, to measure the results and exposure of research subjects at the same time can be used to estimate prevalence for population-based surveys. This method is relatively fast and cheap and can be used to study a variety of outcomes [9-11]. ICDAS detection codes for coronal caries [7] are used in this study. The population of the study was 260 students in Puteran village in the Tasikmalaya district of West Java, Indonesia. The inclusion criteria were children between 6-12 years old who lived in Puteran village in Tasikmalaya district of West Java, Indonesia, willing to participate in the study, and permitted by their parents. Exclusion criteria included those who could not follow the entire research procedure, did not have teeth, or had no teeth. The sampling technique used was purposive sampling. The sample size was calculated using the adequate sample size in the prevalence study [12] with a precision of 0.04, assumed prevalence of 005, and confidence level of 95% and the result of the minimum sample is 114 samples. Sampling from 260 children who met the criteria were, 210 children met both inclusions and did not have exclusion criteria, and 50 students were excluded because they were not allowed by the parents, so we used 210 samples. The location of the research was Puteran village in Tasikmalaya district of West Java, Indonesia. The research was conducted in November 2022. Flow diagram assessed of eligibility in Fig. (1).
Interrater reliability was measured by the kappa statistic as efforts to address potential sources of bias, with a kappa value of 0.81. It was between 0.80-0,90, which was categorized as a strong level of agreement [13]. Data collection was carried out using an electronic form using the Cognito application.
The variable of research is the ICDAS detection codes for coronal caries range from 0 to 6 depending on the severity of the lesion with code and description as follows: Code 0 indicates a healthy tooth with description: no surface caries after 5 seconds of air drying; Code 1 shows the first visual change in enamel: opacity or discoloration (white or brown) is visible at the entrance to the pit or fissure seen after prolonged air drying; Code 2 displays distinct visual change in enamel that is visible when wet, the lesion must be visible when dry; Code 3 with description: localized enamel breakdown (without clinical visual signs of dentinal involvement) is seen when wet and after prolonged drying; Code 4 with description: underlying dark shadow from dentine; Code 5 with description: distinct cavity with visible dentine; Code 6 with description: extensive (more than half the surface) distinct cavity with visible dentine [7].
The data were presented in the form of a frequency distribution table and analyzed using the prevalence rate formula. The data bias existed in the completion of the stated parent's occupation, which needed to be reconfirmed to the teacher at school. There was no missing data in this study because the researcher checked the contents of the inspection form directly after examining the research subjects. The research method and material have received an ethical approval recommendation from the Padjadjaran University Health Research Ethics Committee, Number 1174/UN6.KEP/ EC/2022, November, 21 2022.
3. RESULTS
The research sample that took part in the study was 260 children, but 210 children participated in all stages of the examination until completion. The results regarding caries prevalence in children aged 6-12 years using ICDAS detection codes for coronal caries are displayed in Tables 1-5. The total samples, as many as 210 children, were the subjects of the study who were eligible, met the inclusion and exclusion criteria, and were able to complete the research.
| Characteristics of Respondents | F | % |
|---|---|---|
| Gender | - | - |
| Boy | 115 | 54.8 |
| Girl | 95 | 45.2 |
| Address | - | - |
| Puteran | 210 | 100 |
| Age (Years) | - | - |
| 6 | 6 | 2.9 |
| 7 | 33 | 15.7 |
| 8 | 26 | 12.4 |
| 9 | 34 | 16.2 |
| 10 | 53 | 25.2 |
| 11 | 34 | 16.2 |
| 12 | 24 | 11.4 |
| The Head of Household’s Job | - | - |
| Housewife | 15 | 11.7 |
| Labour | 29 | 13.8 |
| Doctor | 1 | .5 |
| Lecturer | 1 | .5 |
| Teacher | 12 | 5.7 |
| Private sector employee | 24 | 11.4 |
| Self-employed | 103 | 49.0 |
| No Work | 18 | 8.6 |
| Child status | - | - |
| 1st child | 81 | 38.6 |
| 2nd child | 67 | 31.9 |
| 3rd child | 43 | 20.5 |
| 4th child | 10 | 4.8 |
| 5th child | 5 | 2.4 |
| 6th child | 2 | 1.0 |
| 7th child | 0 | 0 |
| 8th child | 0 | 0 |
| 9th child | 1 | 0.5 |
| 10th child | 1 | 0.5 |
| Tooth Condition | Right Maxillary | Left Maxillary | Left Mandibulary | Right Mandibulary | ||||
|---|---|---|---|---|---|---|---|---|
| F | % | F | % | F | % | F | % | |
| Free Caries | 65 | 31,0 | 58 | 27,6 | 33 | 15,7 | 33 | 15,7 |
| Caries | 137 | 65,2 | 142 | 67,6 | 171 | 81,4 | 171 | 81,4 |
| N/A | 8 | 3,8 | 10 | 4,8 | 6 | 2,9 | 6 | 2,9 |
| Total | 210 | 100,0 | 210 | 100,0 | 210 | 100,0 | 210,0 | 100,0 |
Table 1 presents the characteristics of the research subjects based on their gender (boys and girls in almost equal numbers), their age (the majority is 10 years old), their origin (the subjects of study are the residents of Puteran village), their parents’ occupations (mostly self-employed), and their status in the family (mostly first-born children).
Table 2 shows a lower prevalence of caries in the Maxillary Region compared to in the Mandibular Region and the prevalence in both the right and left Mandibular Region (person analysis unit) is equal (81.4%). This value is higher than that in the left Maxillary and Mandibular regions (67.6% and 65.2%, respectively).
The percentage rate of caries is shown in Table 3 (person analysis unit). The largest percentage is found in Code 1. The declining rate from code 1 to code 5 indicates the severity of the caries.
Table 4 displays the prevalence of coronal caries based on ICDAS scoring at 91.4%, whereas Table 5 displays ICDAS code analyses using teeth unit analyses within each Region.
As seen in Table 5, teeth as the unit analysis shows that the largest number of the maxillary and permanent teeth in all sections is in Code 0: healthy tooth surface, indicated by no evidence of caries after 5-sec airdrying, followed by code 2: distinct visual change in enamel visible when wet. The teeth with the most caries detected in the upper jaw are teeth 16, 26, and in the lower jaw are teeth 31, 36, 41, and 46.
| Tooth Condition | Code 1 | Code 2 | Code 3 | Code 4 | Code 5 | Code 6 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | % | F | % | F | % | F | % | F | % | F | % | |
| Free Caries | 19 | 9,0 | 50 | 23,8 | 83 | 39,5 | 140 | 66,7 | 170 | 81 | 151 | 71,9 |
| Caries | 191 | 91,0 | 160 | 76,2 | 127 | 60,5 | 70 | 33,3 | 40 | 19 | 59 | 28,1 |
| Total | 210 | 100 | 210 | 100 | 210 | 100 | 210 | 100 | 210 | 100 | 210 | 100 |
| Tooth Condition | Frequency | % | Caries Prevalence |
|---|---|---|---|
| Free Caries | 18 | 8,6 | 192/210*100%= 91,4 |
| Caries | 192 | 91,4 | |
| Total | 210 | 100 |
| Right Maxillary Permanent Tooth | 18 | 17 | 16 | 15 | 14 | 13 | 12 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|
| F | F | F | F | F | F | F | F | ||
| 0. Sound tooth surface: No evidence of caries after 5 sec air drying | 0 | 8 | 91 | 30 | 46 | 31 | 71 | 101 | 378 |
| 1. First visual change in enamel: Opacity or discoloration (white or brown) | 0 | 0 | 16 | 4 | 8 | 6 | 21 | 20 | 75 |
| 2. Distinct visual change in enamel visible when wet | 0 | 4 | 42 | 18 | 26 | 13 | 41 | 45 | 190 |
| 3. Localized enamel breakdown (without clinical visual signs of dentinal involvement) | 0 | 0 | 38 | 4 | 0 | 5 | 5 | 7 | 61 |
| 4. Underlying dark shadow from dentine | 0 | 0 | 9 | 3 | 0 | 1 | 0 | 5 | 20 |
| 5. Distinct cavity with visible dentine | 0 | 1 | 2 | 2 | 0 | 2 | 1 | 2 | 10 |
| 6. Extensive (more than half the surface) distinct cavity with visible dentine | 0 | 0 | 3 | 2 | 0 | 1 | 0 | 0 | 6 |
| Total | 0 | 13 | 201 | 63 | 80 | 59 | 139 | 180 | 740 |
| Left Maxillary Permanent Tooth | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | Total |
| F | F | F | F | F | F | F | F | ||
| 0. Sound tooth surface: No evidence of caries after 5 sec air drying | 98 | 65 | 28 | 39 | 25 | 82 | 8 | 0 | 345 |
| 1. First visual change in enamel: Opacity or discoloration (white or brown) | 20 | 21 | 5 | 12 | 8 | 11 | 1 | 0 | 78 |
| 2. Distinct visual change in enamel visible when wet | 48 | 50 | 19 | 31 | 22 | 39 | 3 | 0 | 212 |
| 3. Localized enamel breakdown (without clinical visual signs of dentinal involvement) | 9 | 4 | 1 | 9 | 8 | 40 | 5 | 0 | 76 |
| 4. Underlying dark shadow from dentine | 4 | 1 | 0 | 2 | 2 | 14 | 3 | 0 | 29 |
| 5. Distinct cavity with visible dentine | 3 | 0 | 0 | 3 | 1 | 5 | 1 | 0 | 15 |
| 6. Extensive (more than half the surface) distinct cavity with visible dentine | 1 | 1 | 0 | 1 | 0 | 6 | 0 | 0 | 9 |
| Total | 183 | 142 | 53 | 97 | 66 | 197 | 21 | 0 | 764 |
| Left Mandibulary Permanent Tooth | 38 | 37 | 36 | 35 | 34 | 33 | 32 | 31 | Total |
| F | F | F | F | F | F | F | F | ||
| 0. Sound tooth surface: No evidence of caries after 5 sec air drying | 0 | 4 | 33 | 24 | 43 | 67 | 117 | 150 | 438 |
| 1. First visual change in enamel: Opacity or discoloration (white or brown) | 0 | 2 | 8 | 8 | 7 | 9 | 16 | 17 | 67 |
| 2. Distinct visual change in enamel visible when wet | 0 | 9 | 31 | 10 | 20 | 11 | 34 | 28 | 143 |
| 3. Localized enamel breakdown (without clinical visual signs of dentinal involvement) | 0 | 6 | 48 | 8 | 4 | 0 | 1 | 1 | 68 |
| 4. Underlying dark shadow from dentine | 0 | 3 | 33 | 1 | 0 | 3 | 0 | 1 | 41 |
| 5. Distinct cavity with visible dentine | 0 | 0 | 15 | 0 | 2 | 0 | 1 | 1 | 19 |
| 6. Extensive (more than half the surface) distinct cavity with visible dentine | 0 | 4 | 29 | 4 | 1 | 1 | 1 | 0 | 44 |
| Total | 0 | 28 | 197 | 55 | 77 | 91 | 170 | 198 | 820 |
| Right Mandibulary Permanent Tooth | 41 | 42 | 43 | 44 | 45 | 46 | 47 | 48 | Total |
| F | F | F | F | F | F | F | F | ||
| 0. Sound tooth surface: No evidence of caries after 5 sec air drying | 149 | 116 | 62 | 46 | 25 | 33 | 8 | 0 | 439 |
| 1. First visual change in enamel: Opacity or discoloration (white or brown) | 16 | 15 | 9 | 9 | 7 | 10 | 2 | 0 | 68 |
| 2. Distinct visual change in enamel visible when wet | 30 | 36 | 18 | 20 | 16 | 40 | 8 | 0 | 168 |
| 3. Localized enamel breakdown (without clinical visual signs of dentinal involvement) | 3 | 2 | 2 | 5 | 9 | 42 | 4 | 0 | 67 |
| 4. Underlying dark shadow from dentine | 0 | 0 | 1 | 4 | 3 | 29 | 4 | 0 | 41 |
| 5. Distinct cavity with visible dentine | 0 | 0 | 1 | 1 | 0 | 11 | 1 | 0 | 14 |
| 6. Extensive (more than half the surface) distinct cavity with visible dentine | 0 | 0 | 2 | 1 | 1 | 25 | 0 | 0 | 33 |
| Total | 198 | 169 | 95 | 86 | 61 | 190 | 27 | 0 | 830 |
4. DISCUSSION
The characteristics of the respondents in Table 1 show that there is a slight difference in the number of percentages between male and female subjects, as well as differences in gender and age. This research, in line with previous research by Dermici et al. [14], indicates that gender and age do not affect the prevalence of caries on tooth sites but is different from Bhardwaj's study whichstates that gender affects the prevalence of caries [15]. This difference may occur because caries is a disease that is also influenced by many factors, such as social, economic, demographic and nutritional factors [16]. The incidence of caries is higher in younger age groups and declines with age [15]. Caries rates were slightly lower in the oldest and newest generations. Although there has been a decline in caries in children, caries rates increase with age and remain a problem in adults [17]. Variable parents’ jobs as a factor of social-economic in this research were replaced with the head of household's job. During the research, it was found that many children were raised by a single parent because their father died, left without news or the child did not know where his father was.
According to Table 2, the prevalence of caries in the maxilla is lower than that in the mandible. This finding is consistent with the findings of Bhardwaj et al. and Suwargiani et al. study [15, 18], which found that the prevalence of dental caries in the dentition was lower in the mandibular arch than in the maxillary arch. The difference in the incidence of caries in upper jaw teeth and lower jaw teeth is due to some evidence that the sequence of caries attacks is stated to follow a certain pattern. The first order of attack is the mandibular teeth, followed by the maxillary teeth [15, 19].
The above finding is inconsistent with the findings of Al-Darwish et al. who discovered that caries distribution was more prevalent in the maxillary than in the mandibular, and the finding of Demirci study, et al., showed that caries distribution was higher in the maxillary jaw (62.4%) than in the mandibular jaw (37.6%) [14, 20]. This difference may occur because caries can be attributed variety of factors, including regional factors, occupation, income, social class, ethnic group, education, and lifestyle factors, which might affect the prevalence of tooth surface caries [21-23]. and toothbrush use, consumption of fizzy drinks, and father's education level are factors associated with dental caries [24].
The finding indicated by Table 5 shows that the teeth with the most caries detected in the upper jaw are teeth 16 and 26, while in the lower jaw are teeth 31, 36, 41, and 46. This finding is in line with a study from Bhardwaj and Chawla that found the first order of attack of caries is the mandibular molars, followed by the maxillary molars [15, 19]. Demirci study, et al. showed that the first and second molars of the upper jaw were most susceptible to caries, and caries susceptibility in permanent teeth found that molars are more susceptible than incisors, canines or premolars [14] The results can occur because the maxillary first molar tooth is one of the most complicated teeth in the maxillary arch [25] and mandibular molars are most susceptible to caries [14]. This can happen because the permanent first molars are the teeth most susceptible to caries because they erupt at the earliest.
Molar teeth have a morphology that can influence the development of carious lesions, including the presence of deep holes and fissures on the occlusal surface and large crowns, which cause a build-up of more acid produced by bacteria [26]. Furthermore, extensive caries are more common in mandibular molars, with a different level of significance than other teeth. These findings can be attributed to the unique morphology and eruption time of the dental cavities and fissures in the mandibular molars compared to other teeth, as well as the subsequent increase in food retention in conjunction with the early eruption of the mandibular permanent first molars [27].
Table 2 also shows that the prevalence of dental caries in the right and left mandibles has the same prevalence value of 81.4%. This result is the same as research by Elfseyie, et al., which stated that the incidence of caries in the maxillary shows the same value on both sides [28]. The prevalence of dental caries value is higher than the prevalence of caries in the upper left and lower jaw, with values of 67.6% and 65.2% (Table 2), respectively. These findings cannot be compared with prior studies because it is rare to do research on this topic, however, the premolars and molars in the lower jaw are often damaged due to caries [29-31].
Based on the ICDAS code, code 1 accounts for the biggest percentage of caries, as seen in Table 3. Table 3 illustrates a pattern of decreasing ICDAS codes from code 1 to code 5, which represents the most severe form of caries. These results are different from studies that state that the highest average number of occlusal caries in children is the ICDAS code above 0, namely codes 2 and 6, and the lowest code is 4 [32]. These findings indicate that in Puteran Village, the caries pattern is still in the early stages of development. Therefore, it is important to introduce early diagnosis of dental caries to prevent new lesions. This method is expected to strengthen dental and oral health programs in the community by incorporating early prevention activities to prevent the development of new lesions [33].
Table 4 illustrates the prevalence of caries based on the ICDAS assessment, with an occlusal caries prevalence of 91.4 percent. These results are very similar to those of the study by Leon et al., which demonstrated that the prevalence of caries in permanent teeth using the ICDAS measurement tool exceeded 87% [33]. These findings highlight the importance of inviting all stakeholders to reflect on changes to traditionally implemented health strategies, emphasizing preventive strategies aimed at mothers or caregivers as elements of knowledge transmission, prioritizing the practice of brushing teeth with fluoride-containing products and encouraging dentists to take preventive action [33, 34].
The best methods for caries prevention include dietary modification, adequate oral hygiene practices, antimicrobial agents, pit and fissure sealants, and the use of fluoride varnish and fissure sealants [34, 35]. All of these measures target the microorganisms responsible for dental caries to inhibit and limit their growth [34]. The new material, CPP-ACP, is a milk-derived substance that strengthens and re-mineralizes tooth structure and also possesses anti-cariogenic properties. CPP aids in the stabilization of Amorphous Calcium Phosphate (ACP) in the form of a multiphosphoseryl chain. CPP binds to ACP and thereby prevents the dissolution of calcium and phosphate ions. CPP-ACP helps facilitate remineralization and maintains it in a saturated form by acting as a reservoir of naturally available calcium and phosphate [34]. Chlorhexidine varnish provides a moderate caries-prevention impact when applied at intervals of three to four months but has no effect when administered at longer intervals [36].
The ICDAS code analysis by dental analysis unit for each mandibular region is presented in Table 5. The majority of the right maxillary permanent teeth have code 0: Sound-tooth surface: No evidence of caries after 5 seconds of air drying, followed by code 1: first visual change in enamel: opacity or discoloration (white or brown), and code 2 (distinct visual change in enamel visible when wet), followed by code 6 with a percentage. The findings differ slightly from those of Torres' study, which reported that the highest caries coding average value was found in code 3 (3.79; SD ± 3.27) and the lowest average value was found in code 5 (0.49; SD ±0.91) [37] while the findings of this study were lowest at code 6. This is due to the influence of social determinants of health, which have long been defined as the circumstances under which individuals are born, grow, play, live, work, pray, and age, all of which affect health status [38]. Experts acknowledge that health status is shaped by forces such as gene-environment interactions, limited social capital, community resources, social policies, and family economic conditions. This issue conveys a contemporary perspective on common health conditions, highlighting the social burdens faced by children and under-resourced families [38].
Differences in ICDAS scores for children aged 6 to 12 years were associated with family background, oral hygiene, the frequency of visits to the dental practice, and eating habits. These data will serve as the foundation for conducting community-based oral health promotion interventions to lower the prevalence of dental caries in the population. This strategy will incorporate primary prevention methods that address resistance to disease progression as well as secondary prevention methods aimed at halting the development of dental disease. Primary prevention methods may comprise the use of fluorides, sugar substitutes, mechanical hole blocking and sealing, and health education in schools and kindergartens. Secondary prevention will aim to get an early diagnosis and prompt treatment to reduce the complications of the lesion.
The limitation of this study is the research results cannot be generalized, and the results cannot be applied in various regions because there are slightly varying characteristics of the respondents' parents in this research sample. This study did not examine caries risk factors as an oral health determinant, and the research results did not analyze the relationship between health determinants and ICDAS results; as a result, these causal factors cannot be investigated more clearly. A previous study by Suwargiani et al. Suggestions for further research are to study the relationship with the determinant factors and provide health promotion interventions and caries prevention to suppress caries development.
CONCLUSION
The ICDAS assessment showed a caries prevalence of 91.4% among permanent teeth in children aged 6 to 12 years. The prevalence of caries is higher in the mandible than in the maxilla. At these ages, the majority of ICDAS assessments are code 1, and the percentage value of caries is higher in ICDAS code 1 than in codes 2 to 6. The trend of decreasing numbers indicates that the percentage value of ICDAS decreases from code 1 to code 5, which represents the most severe condition of caries, and the teeth with the most caries detected in the upper jaw are teeth 16, 26, and in the lower jaw are teeth 31, 36, 41, and 46. The implication of the research is detecting coronal caries in children in Puteran Village using ICDAS so it can measure dental caries and support and facilitate comprehensive caries care to improve long-term health outcomes for children by the local health department. The local health department can collaborate with the dental public health department at universities to create a comprehensive dental caries problem-solving program.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Institutional Review Board (or Ethics Committee) of the Health Research Ethics Committee of the Faculty of Medicine of Universitas Padjadjaran, Indonesia. The research has received an ethical approval recommendation from the Padjadjaran University Health Research Ethics Committee, Number 1174/UN6.KEP/EC/2022, November, 21 2022.
HUMAN AND ANIMAL RIGHTS
No animals were used that are the bassis of this study. The study was conducted by the Declaration of Helsinki.
CONSENT FOR PUBLICATION
All subjects/patients completed written informed consent and it was obtained prior to data collection.

