All published articles of this journal are available on ScienceDirect.

Clinical Performance of Two CAD/CAM Fabricated Ceramic Restorations with Different Designs for MIH Rehabilitation: A Randomized Controlled Trial
Authors Info & Affiliations
Abstract
Background:
Molars affected with severe molar incisor hypomineralisation (MIH) require extensive restorations, which do not last for a long time and often require treatment in the form of onlays or full coverage restorations.
Objective:
A randomized clinical trial evaluated the clinical performance of two CAD/CAM fabricated ceramic restorations, Vita Suprinity (VS) and Vita Enamic (VE), with different preparation designs, occlusal veneer and endocrown, for rehabilitation of the first permanent molar affected by MIH.
Materials and Methods:
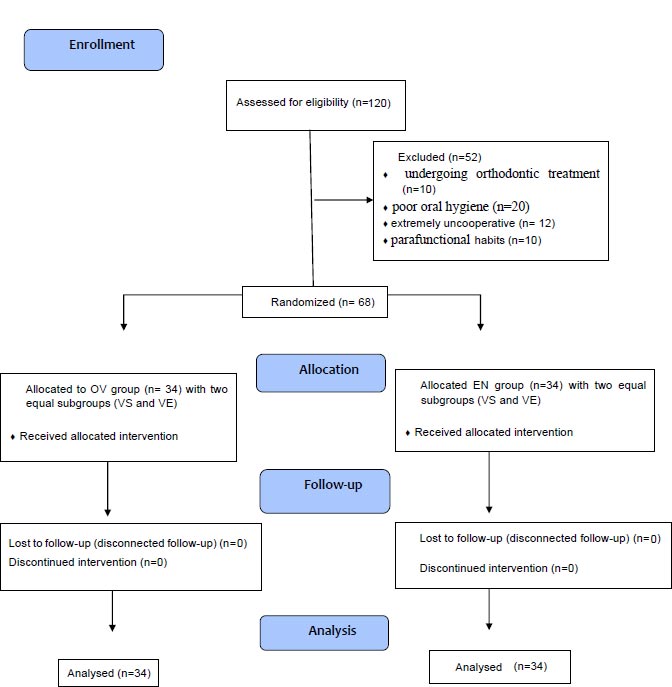
The study was registered with NCT05434884 clinical trial ID with 68 patients ranging from 8 to 13 years old, who attended the dental clinic of Al-Azhar University, Girls Branch, and suffering from a severe form of molar incisor hypomineralization. The patients were divided equally into two groups, group I, i.e., occlusal veneer (OV) group, and group II, i.e., endocrown (EN) group, according to different preparation designs related to different severity levels of first permanent molars’ hypomineralization (moderate and severe); each group was subdivided equally and randomly into two subgroups, subgroup A, i.e., Vita Suprinity (VS), and subgroup B, i.e., Vita Enamic (VE), according to the material used for fabrication of the restoration. The survival and success rates of restorations were assessed using the clinical United States Public Health Service (USPHS) criteria at 1 week, and 3, 6, 12, and 18 months' recall times after cementation, and statistical analysis was performed.
Results:
There was no statistically significant difference between groups and subgroups in terms of all evaluation parameters during the whole observational period.
Conclusion:
Based on observations, occlusal veneer and endocrown designs fabricated from CAD/CAM VS and VE showed similar clinical success in the rehabilitation of first permanent molars with severe MIH over 18 months of evaluation.
1. INTRODUCTION
Molar incisor hypomineralization (MIH) is a type of qualitative enamel defect that occurs due to disruption of the ameloblastic activity during the process of amelogenesis [1]. However, the enamel thickness appears normal, but it is fragile due to the presence of subsurface porosities and is liable to fracture under masticatory forces; this usually affects the first permanent molars and incisors [1] and may also affect other teeth, like canines and the second molar [2]. MIH has a strong negative effect on oral-health-related quality of life (OHRQoL); malformed teeth can be hypersensitive, and discoloration might affect children's appearances, reducing their well-being [3].
According to the European Academy of Pediatric Dentistry (EAPD) criteria [4], there are common features specific to hypomineralized first permanent molars, which are demarcated opacities, post-eruptive enamel loss, sensitivity, atypical restoration, and extraction of molars due to MIH. According to these features, molar hypomineralization (MH) has been rated into mild (demarcated enamel opacities without enamel breakdown and induced sensitivity to external stimuli, i.e., air, water, but not brushing), and severe (demarcated enamel opacities with breakdown and caries, spontaneous and persistent hypersensitivity, affecting function, including brushing and mastication) [4]. Dental management of MIH represents a challenge for pediatric dentists due to variations in clinical appearance and the broad spectrum of treatment modalities, which range from prevention or restorations to extraction and orthodontic management [1].
Successful preventive and treatment options have been studied and identified for MIH-affected molars, with the severity of the defect and the age of the patient often dictating the chosen approach [5]. Fissure sealants can be used in mild cases in fully erupted molars; glass ionomer cement (GIC) restorations using a non-invasive approach may be used in cases where the child cannot be subjected to conventional treatment. Composite resin restorations placed under rubber dam isolation, using an invasive approach, can be used as a restorative option in mild/severe cases besides laboratory-made restorations [4]. Usually, full coverage using prefabricated metal crowns (PMCs) can be placed in severe cases [5].
As the conservation of tooth structure is considered vital in maintaining the subtle equilibrium between biological, mechanical, and esthetic factors, the protocol for placing restorations has altered [6]. Thus, newly cuspal coverage restorations, like occlusal veneers and endocrowns, can be provided without complete reduction of axial tooth surfaces or subgingival margins for severe MIH-related defects subsequently. Occlusal veneer restoration offers a viable promising conservative alternative to repair the defect in the occlusal third of the tooth; it consists of thin overlay coverage restoration with a non-retentive form [7]. While endocrown restoration or adhesive endodontic restoration is the monoblock technique indicated in teeth with extensive loss of coronal structure with pulp involvement, it is anchored to the internal portion of the pulp chamber and the cavity margins [8].
CAD/CAM equipment has been more and more used to fabricate dental prostheses in recent years [9]. Industrially made CAD/CAM ceramic blocks have been developed to enhance the mechanical properties of restoration [9]. Occlusal veneers and endocrown restorations can be fabricated from different ceramic materials. Recently, due to the continuing development of ceramic materials, the recently invented zirconia-reinforced lithium silicate glass ceramics blocks, Vita Suprinity, have been introduced [9]. It was claimed that this new addition of 8-10% zirconia to lithium silicate produced a new material category with high fracture resistance and superior mechanical properties with better esthetics [9].
The hybrid ceramic CAD/CAM materials have been suggested to create materials with a closely harmonized modulus of elasticity to dentin, which can be milled more easily than glass ceramics. In addition, it is easily repaired inside the patient's mouth and has grander esthetic properties. Recently, a hybrid ceramic CAD-CAM material has been introduced, called Vita Enamic, which consists of a polymer network (14% by weight) with an even distribution of ceramic network (86% by weight). This particularly planned hybrid ceramic makes it a perfect high-strength and stress-absorbing restoration for all indications of fixed restorations [9, 10].
The long-term success of any dental restoration is affected by its clinical performance. Despite the variances between the two materials, Vita Suprinity and Vita Enamic, revealed by in vitro studies, there is no adequate clinical evidence that supports the choice of a ceramic material over resin composite for indirect restorations inside the patient's mouth. These two materials have not been compared adequately in a clinical condition because the authors’ knowledge and information regarding their clinical performance are insufficient [11].
Thus, the current study aimed to compare the clinical performance of these two materials with different preparation designs after recall times of 18 months according to Modified Ryge Criteria (USPHS); the null hypothesis was that there would be no difference in clinical performance between the two materials.
2. MATERIALS AND METHODS
In the present randomized prospective study, ethical board approval was obtained before the commencement of the study from the Ethical Committee of Al-Azhar University (REC-PD-22-10), and all the procedures were conducted following the guidelines laid out in the Declaration of Helsinki. The study was further registered with the clinical trial registry (NCT05434884). All parents were asked to sign an informed consent after a detailed explanation of the procedures and possible outcomes of treatment. Children were excluded from the study when their parents declined to sign the form.
2.1. Selection of the Participants
Participants were selected from patients who attended the dental clinic of Al-Azhar University, Girls branch, with specific inclusion criteria as follows:
1- 8-13 years old healthy children without chronic diseases.
2- Having at least one fully erupted permanent first molar tooth affected with a severe form of MIH according to EAPD criteria [4] with the extent of caries and breakdown varying from the contribution of a minimum of two cusps to the pulp involvement, indexed 4 (b and c) in MIH TNI [12].
3- Patients having good oral hygiene as represented by an oral hygiene index of 0 and being able to maintain oral hygiene measures.
4- Participants being able to tolerate conventional restorative procedures and willing to return for a follow-up examination.
2.2. Exclusion Criteria
Patients with parafunction, active periodontal diseases, poor oral hygiene, undergoing orthodontic treatment, and patients having psychiatric problems or unrealistic expectations were excluded from this trial.
2.3. Sample Size Computation
Based on the study by Dhareula et al. [13] and by using the G power statistical power analysis program (version 3.1.9.7) (Franz Faul, Kiel University, Germany, Copyright ©1992-2020), the sample size was computed. After dropout, a total sample size of 68 (34 in each group, subdivided into 17 in each subgroup) was obtained, being sufficient to notice a great effect size (d) =1.03, with an actual power (1-β error) of 0.8 (80%) and a significance level (α-error) of 0.05 (5%), for a two-sided hypothesis test.
2.4. Study Design
This was a prospective randomized controlled study, in which patients, caregivers, and pediatric dentists were blinded for the type of ceramic restoration used in subgroups. All treatments were performed by two experienced, calibrated pediatric dentists, a fixed prosthodontist, and an endodontist. Randomization of subgroups was done with a contingency number table on www.random.org and preserved in sequentially numbered, sealed envelopes.
2.5. Baseline Assessment
Medical and dental history for all patients was recorded, oral hygiene status was assessed, and also, all teeth were clinically examined with a dental mirror and a dental explorer (High line series Bibodent® Egypt) under standard dental unit lightning. MIH was diagnosed and classified according to the criteria proposed by Lygidakis et al. [4]. The participant was graded as having a mild or a severe MIH according to the most affected MIH tooth. Only patients with the severe form criteria were included in the study, including demarcated enamel opacities with breakdown and caries, spontaneous and persistent hypersensitivity, affecting the function of brushing and mastication, with the extent of caries and breakdown varying from the contribution of a minimum of two cusps to pulp involvement, indexed as 4 b; more than 1/3 till 2/3 defect extension as 4 c, and more than 2/3 defect extension and/or defect close to the pulp or atypical restoration in MIH TNI [12].
Patients complained of hypersensitivity, which was further measured by cold air stimulus. The air was delivered with a standard dental unit air syringe at maximum pressure for 1s from a distance of 1cm perpendicular to the occlusal surface of the affected tooth. Schiff Cold Air Sensitivity Scale (SCASS) [13, 14] was used to assess the degree of hypersensitivity in the affected teeth, and only scores 2 and 3 were included in the study.
Moreover, data on confounding factors, such as the number of affected teeth, the involvement of the permanent incisors, and DMFT values, were recorded, The children were clinically examined and diagnosed by two experienced calibrated pediatric dentists and a restorative dentist, obtaining a Cohen’s kappa coefficient for inter-examiner calibration of 0.83. Teeth treatment and preparation were performed by a professional restorative dentist, endodontist, and a fixed prosthodontist. Also, patients were followed up by the 2 blinded pediatric dentists.
2.5.1. Grouping of the Participants
Patients were divided equally into two groups (34 patients each) according to different preparation designs related to different severity levels for rehabilitation of permanent first molars in molar incisor hypomineralization. The two groups are as follows. (Fig. 1)
2.5.1.1. Group I (OV)
Patients received occlusal veneer restorations representing occlusal veneer preparation with a circumferential chamfer finish line and proximal slot, proposed as modified occlusal veneer design, for rehabilitation of severe MIH TNI 4b index, without pulp involvement.
2.5.1.2. Group II (EN)
Patients received endocrown restorations after endodontic treatment for rehabilitation of MIH TNI 4c index and suffered from irreversible pulpitis.
Each group was further subdivided equally and randomly into two subgroups (17 patients each) according to different materials used for the fabrication of the restorations:
2.6. Clinical Procedures
2.6.1. I- Pre-operative Phase
In this phase, the case history was taken from each patient. A pre-operative clinical examination (as previously discussed), photographs, panoramic radiographs, and analytical casts for maxillary and mandibular arches were prepared from alginate (Tropicalgin, Zhermack SPA, Italy) impression material. The maxillary and mandibular casts were fixed on the articulator (A7 Fix; BioArt, Brazil).
2.6.2. II- Operative Phase
Shade selection was determined before tooth preparation in natural sunlight at 11 o’clock. Two putty indexes were used for the design of the modified proposed occlusal veneer and endocrown preparation to standardize the amount of tooth reduction in both groups.
2.6.2.1. Modified Proposed Occlusal Veneer Preparation [Group I (OV)]
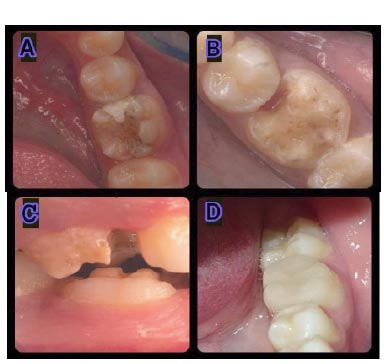
The occlusal surface was prepared following the occlusal anatomy with a 1.5 mm reduction at the cusp tip, 1 mm at the fossa, supragingival circumferential chamfer finish line 1mm in width, as well as one shallow mesial slot (2mm width and 1.5mm depth). Finishing and smoothening of the preparation were carried out [10] (Fig. 2A, B).
2.6.2.2. Endocrown Preparation [Group II (EN)
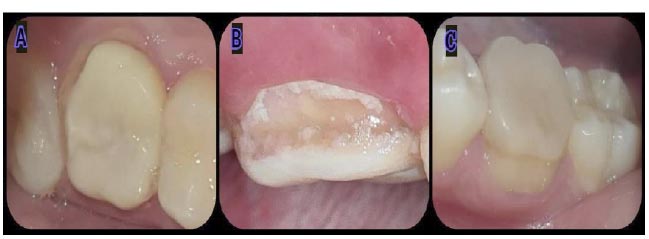
All decayed areas of the tooth were removed. The occlusal surface was reduced following the occlusal anatomy at 2 mm. The undercuts of the tooth cavity were blocked out with a flowable composite resin, and the internal walls of the cavity were diverged to 8 degrees. Enamel walls with a thickness of less than 1 mm were removed. Reshaping of all sharp edges and angles was performed [15] (Fig. 3A, B). Assessment of the accuracy of the preparation dimensions in both groups was performed with the putty index and the electronic digital caliper.
In both groups, full-arch impressions were taken using a two-stage putty-wash impression procedure with an additional silicon impression material (ExpressTM, 3M ESPE, Germany).
The prepared tooth of occlusal veneer was covered with bis-acryl provisional restorations (Protemp, 3M Oral Care), while the cavity wall of endocrown preparation was filled with provisional filling material (Orafill G, Indian). The final impressions and occlusal bite were delivered to the laboratory for the construction of occlusal veneers and endocrown restorations by standardized techniques.

2.6.2.3. Fabrication of all Ceramic Restorations
Each tooth with different preparation designs was restored with one of the two CAD/CAM materials: Vita Suprinity (VITA Zahnfabrik, Germany) or Vita Enamic (VITA Zahnfabrik, Germany).
The two types of restorations were designed and milled using the Cerec in Lab system (Sirona, Dentsply, Germany), consisting of a personal computer, inEosX5 Blue scanner, and inLab MC X5 milling unit, by the same dental technician following the manufacturer’s instructions. According to the manufacturer’s instructions, the crystallization of Vita Suprinity was performed using a Vita vacuum furnace. After that, the polishing of Vita Suprinity and Vita Enamic samples was done using the Vita Suprinity Polishing kit (Vita Zahnfabric, Bad Sackingen, Germany) as well as Vita Enamic Polishing kit (Vita Zahnfabric, Bad Sackingen, Germany) correspondingly with no additional glaze firing.
2.6.2.4. Cementation Procedure
All cementation procedures were carried out under rubber dam isolation. Cleaning of teeth was performed using a polishing brush, and all occlusal veneers and endocrowns were evaluated intraorally for seating, marginal fit, and proximal, occlusal contact.
All internal surfaces of restorations were treated initially by etching with 5% hydrofluoric acid (BISCO, Inc, USA) applied for 40 seconds. Subsequently, each restoration was cleaned for 5 minutes using ultrasound with water and then dried with oil-free air. This was followed by the application of a silane coupling agent (Bisco, Inc, USA) for 30 seconds according to the manufacturer’s recommendations, and then it was thoroughly dispersed with air. After that, each restoration was adhesively cemented to its abutment by Total Cem (Itena, France) self-adhesive resin cement following the manufacturer’s instructions. Excess cement was removed after a brief light exposure, followed by light polymerization on each surface for 20 seconds (Figs. 2C, D, 3C). Periapical radiographs were taken after cementation.
2.7. III– Postoperative Phase
Patients were trained to follow oral hygiene measures in order to avoid recurrent caries or plaque accumulation around new restorations.
2.8. Clinical Evaluation
The restorations were assessed using the United States Public Health Service (USPHS) criteria [16] at baseline (1 week), and 3, 6, 12, and 18 months after cementation. Moreover, gingival health was recorded and compared with the antagonistic tooth using the Loe and Silness index [16].
Restoration fractures, recurrent caries at the crown margin, marginal adaptation, and discoloration were assessed [11]. The ratings were executed by the two pediatric dentists, both of whom were calibrated concerning the USPHS criteria. Clinical inspections were achieved using a mirror and sharp explorer, photographs, as well as radiographic inspections. A cumulative survival rate along with clinical success was assessed.
2.9. Statistical Analysis
Data management and statistical analysis were performed using the Statistical Package for Social Sciences (SPSS) version 18 software (IBM, Armonk, NY, USA). Categorical qualitative data were expressed as numbers and percentages, and were compared using the Chi-square test. According to the USPHS criteria, scores alpha and bravo represent “success,” while Charlie represents “failure”. To resolve the survival rates obtained for all restorations, Kaplan-Meier statistics were used. All p-values were two-sided. The significance level was set at P ≤ 0.05.
3. RESULTS
68 patients with different preparation designs (occlusal veneers and endocrowns) were examined clinically at the specific recall periods (Tables 1, 2). 34 patients received occlusal veneer preparation, and were included in group I (OV), with 17 patients in each subgroup of VS and VE. One patient (in subgroup VS) with one occlusal veneer did not show up at the 18-months follow-up, and the patient’s data were excluded from statistical evaluation. 34 patients received endocrown preparations, and were included in group II (EN), with 17 patients in each subgroup of VS and VE. One patient (in subgroup VE) with one endocrown did not show up at 6-months, 1-year, and 18-months follow-up, and the patient’s data were excluded from statistical evaluation. The intraexaminer reliability analyzed using the kappa statistical technique showed a degree of agreement k at the interval 0.95-1.
| - | Time | Score | Group OV | Group EN | - | P-value between Four Subgroups | |||
|---|---|---|---|---|---|---|---|---|---|
| VS | VE | P# | VS | VE | P# | ||||
| Fracture | Baseline | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns |
| M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| 12M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| 18M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| P within subgroup | ns | ns | - | ns | ns | ||||
| Sensitivity | Baseline | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns |
| M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| 12M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| 18M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| P within subgroup | ns | ns | ns | ns | |||||
| Secondary caries | Baseline | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns |
| M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| 12M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| 18M | Alpha | 100% | 100% | 0.31 ns | 100% | 100% | ns | 0.38 ns | |
| P within subgroup | ns | 0.38 ns | ns | ns | |||||
| Marginal adaptation | Baseline | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns |
| M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| 12M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| 18M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| P within subgroup | ns | ns | ns | ns | |||||
| Marginal discoloration | Baseline | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns |
| M | Alpha | 100% | 100% | ns | 100% | 100% | ns | ns | |
| M | Alpha | 88% | 100% | 0.144 ns | 100% | 100% | ns | 0.103 ns | |
| 12M | Alpha | 88% | 100% | 0.144 ns | 100% | 100% | ns | 0.103 ns | |
| 18M | Alpha | 88% | 100% | 0.144 ns | 100% | 100% | ns | 0.103 ns | |
| P within subgroup | 0.533 ns | ns | ns | ns | |||||
| Plaque score | Baseline | 0 | 100% | 100% | ns | 100% | 100% | ns | ns |
| M | 0 | 100% | 100% | ns | 100% | 100% | ns | ns | |
| M | 0 | 100% | 100% | ns | 100% | 100% | ns | ns | |
| 12M | 0 | 100% | 88% | 0.144 ns | 100% | 100% | ns | 0.103 ns | |
| 18M | 0 | 94% | 88% | 0.545 ns | 100% | 94% | 0.31 ns | 0.546 ns | |
| P within subgroup | 0.38 ns | 0.178 ns | ns | 0.38 ns | |||||
| - | Time | Score | Group OV | Group EN | - | P value between Four Subgroups | |||
|---|---|---|---|---|---|---|---|---|---|
| VS | VE | P# | VS | VE | P# | ||||
| Survival rate | Baseline | Survival | 100% | 100% | ns | 100% | 100% | ns | ns |
| M | Survival | 100% | 100% | ns | 100% | 100% | ns | ns | |
| M | Survival | 100% | 100% | ns | 100% | 100% | ns | ns | |
| 12M | Survival | 100% | 100% | ns | 100% | 100% | ns | ns | |
| 18M | Survival | 100% | 100% | ns | 100% | 100% | ns | ns | |
| P within subgroup | ns | ns | ns | ns | |||||
| Success rate | Baseline | Success | 100% | 100% | ns | 100% | 100% | ns | ns |
| M | Success | 100% | 100% | ns | 100% | 100% | ns | ns | |
| M | Success | 88% | 100% | 0.144 ns | 100% | 100% | ns | 0.103 ns | |
| 12M | Success | 88% | 88% | ns | 100% | 100% | ns | 0.235 ns | |
| 18M | Success | 82% | 82% | ns | 100% | 94% | 0.31 ns | 0.231 ns | |
| P within subgroup | 0.231 ns | 0.075 ns | ns | 0.38 ns | |||||
Significance level at P≤0.05, ns=non-significant.
3.1. Clinical Evaluation (Tables 1, 2 and Figs. 4, 5, 6)
3.1.1. Fracture
3.1.1.1. Comparison between the Groups
At baseline, 3 months, 6 months, 12 months, and 18 months, the alpha score was recorded for all cases (100%) in all subgroups, indicating no significant difference between the groups (p=1).
3.1.1.2. Comparison of different Observation Times within the same Subgroup
Within group OV and group EN and subgroups VS and VE, for all cases (100%) consistently, score alpha was recorded throughout the study. The difference by time was not statistically significant (p=1).
3.1.1.3. Comparison between Subgroups of the same Group
Group OV: At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference between the subgroups (p=1).
Group EN: At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference between the subgroups (p=1).
3.1.2. Sensitivity
3.1.2.1. Comparison between the Groups
At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in all subgroups, score alpha was recorded, with no significant difference between the groups (p=1).
3.1.2.2. Comparison of different Observation Times within the same Subgroup
Within group OV and group EN and subgroups VS and VE, for all cases (100%), score alpha was consistently recorded throughout the study. The difference by time was not statistically significant (p=1).
3.1.2.3. Comparison between the Subgroups of the same Group
Group OV: At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference between the subgroups (p=1).
Group EN: At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference between the subgroups (p=1).
3.1.2.4. Comparison between the Four Subgroups
At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in all subgroups, score alpha was recorded, with no significant difference between the groups (p=1).
3.1.3. Secondary Caries
3.1.3.1. Comparison between the Groups
Subgroup VS: At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in both the subgroups, score alpha was recorded, with no significant difference between the groups (p=1).
Subgroup VE: At baseline, 3 months, 6 months, and 12 months, for all cases (100%) in both subgroups, score alpha was recorded, with no significant difference between the groups (p=1). At 18 months, for 94% of cases in group OV, score alpha was recorded, and for 6%, score bravo was recorded, in comparison to 100% of cases recording score alpha in group EN; however, this difference was not statistically significant (p=0.31).
3.1.3.2. Comparison of different Observation Times within the same Subgroup
Within group OV (subgroup VS) and group EN (subgroups VS and VE), for all cases (100%), score alpha was consistently recorded throughout the study. The difference by time was not statistically significant (p=1). In group OV (subgroup VE), score alpha was noted in 100% of the cases at baseline, 3 months, 6 months, and 12 months, and in 94% of cases at 18 months, with no significant difference by time (p=0.38).
3.1.3.3. Comparison between Subgroups of the same Group
Group OV: At baseline, 3 months, 6 months, and 12 months, all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference between the subgroups (p=1). At 18 months, for all cases in subgroup VS, score alpha was recorded, in comparison to 94% in subgroup VE, with no significant difference observed between the subgroups (p=0.31).
Group EN: At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference observed between the subgroups (p=1).
3.1.3.4. Comparison between the Four Subgroups
At baseline, 3 months, 6 months, and 12 months, for all cases (100%) in all subgroups, score alpha was recorded, with no significant difference between the groups (p=1). At 18 months, for one case (6%) in group OV and subgroup VE, score bravo was recorded, whereas for all cases in other subgroups, score alpha was recorded. However, this difference was not statistically significant (p=0.38).
3.1.4. Marginal Adaptation
3.1.4.1. Comparison between the Groups
At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in all subgroups, score alpha was recorded, with no significant difference between the groups (p=1).
3.1.4.2. Comparison of different Observation Times within the same Subgroup
Within group OV and group EN and subgroups VS and VE, for all cases (100%), score alpha was consistently recorded throughout the study. The difference by time was not statistically significant (p=1).
3.1.4.3. Comparison between Subgroups of the same Group
Group OV: At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference between the subgroups (p=1).
Group EN: At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference between the subgroups (p=1).
3.1.5. Marginal Discoloration
3.1.5.1. Comparison between the Groups
Subgroup VS: At baseline and 3 months, for all cases (100%) in both subgroups, score alpha was recorded, with no significant difference between the groups (p=1). At 6, 12, and 18 months, for 88% of cases in group OV, score alpha was recorded, and for 12%, score bravo was recorded, in comparison to 100% of cases recording score alpha in group EN; however, this difference was not statistically significant (p=0.144).
Subgroup VE: At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in both subgroups, score alpha was recorded, with no significant difference between the groups (p=1).
3.1.5.2. Comparison of different Observation Times within the same Subgroup
Within group OV (subgroup VE) and group EN (subgroups VS and VE), for all cases (100%), score alpha was consistently recorded throughout the study. The difference by time was not statistically significant (p=1). In group OV (subgroup VS), score alpha was noted in 100% of the cases at baseline and 3 months, and in 88% of cases at 6 months, 12 months, and 18 months, with no significant difference by time observed (p=0.533).
3.1.5.3. Comparison between Subgroups of the same Group
Group OV: At baseline and 3 months, for all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference between the subgroups (p=1). At 6, 12, and 18 months, for all cases in subgroup VE, score alpha was recorded, in comparison to 88% in subgroup VS, with no significant difference observed between the subgroups (p=0.144).
Group EN: At baseline, 3 months, 6 months, 12 months, and 18 months, for all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference between the subgroups (p=1).
3.1.5.4. Comparison between the Four Subgroups
At baseline and 3 months, for all cases (100%) in all subgroups, score alpha was recorded, with no significant difference between the groups (p=1). At 6, 12, and 18 months, for 2 cases (12%) in group OV and subgroup VS, score bravo was recorded, whereas for all cases in other subgroups, score alpha was recorded. However, this difference was not statistically significant (p=0.103).
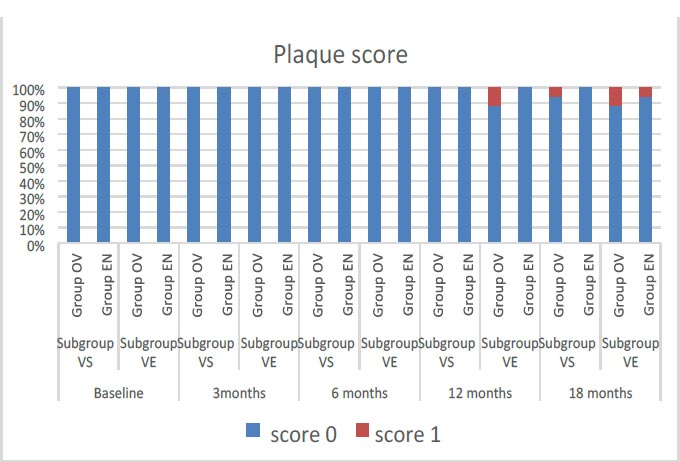
3.1.6. Plaque Score
3.1.6.1. Comparison between the Groups
Subgroup VS: At baseline, 3, 6, and 12 months, for all cases (100%) in both subgroups, score alpha was recorded, with no significant difference between the groups (p=1). At 18 months, for 94% of cases in group OV, score alpha was recorded, and for 6% of cases, score bravo was recorded, in comparison to 100% of cases recording score alpha in group EN; however, this difference was not statistically significant (p=0.31).
Subgroup VE: At baseline, 3 months, and 6 months, for all cases (100%) in both subgroups, score alpha was recorded, with no significant difference between the groups (p=1). At 12 months, the score alpha was recorded for 88% of cases in group OV, in comparison to 100% of cases in group EN; however, no significant difference (p=0.144) was observed. At 18 months, score alpha was recorded for 88% of cases in group OV, in comparison to 94% of cases in group EN; however, no significant difference (p=0.545) has been observed.
3.1.6.2. Comparison of different Observation Times within the same Subgroup
Within group EN (subgroup VS), for all cases (100%), score alpha was consistently recorded throughout the study. The difference by time was not statistically significant (p=1). In group OV (subgroup VS) and group EN (subgroup VE), score alpha was noted in 100% of the cases at baseline, 3, 6, and 12 months, and in 94% of cases at 18 months, with no significant difference observed by time (p=0.38).
In group OV (subgroup VE), score alpha was noted in 100% of the cases at baseline, 3, and 6 months, and in 88% of cases at 12 and 18 months, with no significant difference observed by time (p=0.178).
3.1.6.3. Comparison between Subgroups of the same Group
Group OV: At baseline, 3 and 6 months, for all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference between the subgroups (p=1). At 12 months, for all cases in subgroup VS, score alpha was recorded, in comparison to 88% in subgroup VE, with no significant difference observed between the subgroups (p=0.144). At 18 months, for 94% of cases in subgroup VS, score alpha was recorded, in comparison to 88% in subgroup VE, with no significant difference observed between the subgroups (p=0.545).
Group EN: At baseline, 3 months, 6 months, and 12 months, for all cases (100%) in subgroups VS and VE, score alpha was recorded, with no significant difference between the subgroups (p=1). At 18 months, for all cases in subgroup VS, score alpha was recorded, in comparison to 94% in subgroup VE, with no significant difference observed between the subgroups (p=0.31).
3.1.6.4. Comparison between the Four Subgroups
At baseline, 3 and 6 months, for all cases (100%) in all subgroups, score alpha was recorded, with no significant difference between the groups (p=1). At 12 months, for 2 cases (12%) in group OV and subgroup VE, score bravo was recorded, whereas for all cases in other subgroups, score alpha was recorded. However, this difference was not statistically significant (p=0.103).
At 18 months, for 2 cases (12%) in group OV and subgroup VE and one case (^%) in each of the subgroups OV-VS and EN-VE, score bravo was recorded, whereas for all cases in the EN-VS subgroup, score alpha was recorded. However, this difference was not statistically significant (p=0.546).
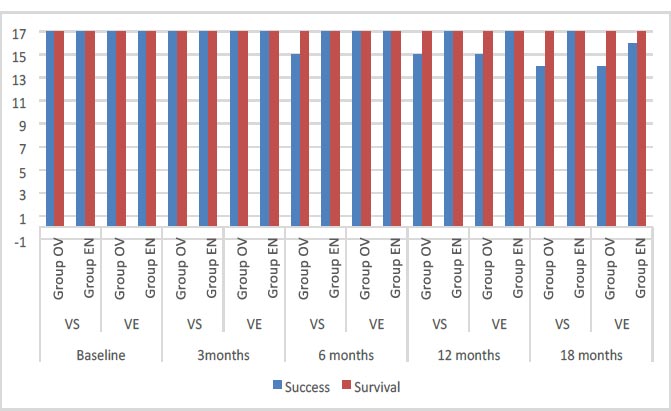
3.1.7. Survival Rate
3.1.7.1. Comparison between the Groups
At baseline, 3 months, 6 months, 12 months, and 18 months, all cases (100%) in all subgroups showed survival, with no significant difference between the groups (p=1).
3.1.7.2. Comparison of different Observation Times within the same Subgroup
Within group OV and group EN and subgroups VS and VE, all cases (100%) consistently showed survival throughout the study. The difference by time was not statistically significant (p=1).
3.1.7.3. Comparison between Subgroups of the same Group
Group OV: At baseline, 3 months, 6 months, 12 months, and 18 months, all cases (100%) in subgroups VS and VE showed survival, with no significant difference between the subgroups (p=1).
Group EN: At baseline, 3 months, 6 months, 12 months, and 18 months, all cases (100%) in subgroups VS and VE showed survival, with no significant difference between the subgroups (p=1).
3.1.8. Success Rate
3.1.8.1. Comparison between the Groups
Subgroup VS: At baseline and 3 months, all cases (100%) in both subgroups showed success, with no significant difference between the groups (p=1). At 6 and 12 months, 88% of cases in group OV showed success and 12% failure, in comparison to 100% showing success in group EN; however, this difference was not statistically significant (p=0.144). At 18 months, 82% of cases in group OV showed success and 18% failure, in comparison to 100% showing success in group EN; however, this difference was not statistically significant (p=0.069).
Subgroup VE: At baseline, 3 and 6 months, all cases (100%) in both subgroups showed success, with no significant difference between the groups (p=1). At 12 months, 88% of cases in group OV showed success and 12% failure, in comparison to 100% showing success in group EN; however, this difference was not statistically significant (p=0.144). At 18 months, 82% of cases in group OV showed success and 18% failure, in comparison to 94% showing success in group EN; however, this difference was not statistically significant (p=0.287).
3.1.8.2. Comparison of different Observation Times within the same Subgroup
Within group EN (subgroup VS), all cases (100%) consistently showed success throughout the study, with no difference by time (p=1).
In group OV (subgroup VS), success was noted in 100% of the cases at baseline and 3 months, in comparison to 88% success at 12 months and 82% success at 18 months, with no significant difference by time (p=0.231).
In group OV (subgroup VE), success was noted in 100% of the cases at baseline, 3, and 6 months, and in 88% of cases at 12 and 82% at 18 months, with no significant difference by time (p=0.075). In group EN (subgroup VE), success was noted in 100% of the cases at baseline, 3, 6, 9, and 12 months, and in 94% at 18 months, with no significant difference by time (p=0.38).
3.1.8.3. Comparison between Subgroups of the same Group
Group OV: At baseline and 3 months, all cases (100%) in subgroups VS and VE showed success, with no significant difference between the subgroups (p=1). At 6 months, for 88% of cases in subgroup VS, score alpha was recorded, in comparison to 100% in subgroup VE; however, no significant difference has been observed between the subgroups (p=0.144). At 12 months, 88% of cases in both subgroups VS and VE recorded success, with no significant difference between subgroups (p=1). At 18 months, 82% of cases in both subgroups VS and VE recorded success, with no significant difference observed between the subgroups (p=1).
Group EN: At baseline, 3 months, 6, and 12 months, all cases (100%) in subgroups VS and VE recorded success, with no significant difference observed between the subgroups (p=1). At 18 months, all cases in subgroup VS recorded success, in comparison to 94% in subgroup VE, with no significant difference observed between the subgroups (p=0.31).
3.1.8.4. Comparison between the Four Subgroups
At baseline and 3 months, all cases (100%) in all subgroups showed success, with no significant difference between the groups (p=1). At 6 months, 2 cases (12%) in group OV and subgroup VS demonstrated failure, whereas all cases in other subgroups succeeded. However, this difference was not statistically significant (p=0.103).
At 12 months, 2 cases (12%) in group OV and subgroups VS and VE demonstrated failure, whereas all cases in subgroups of group EN succeeded. However, this difference was not statistically significant (p=0.235).
At 18 months, 3 cases (18%) in group OV and subgroups VS and VE showed failure, in comparison to no failure observed in group EN and subgroup VS; however, only one failed case (6%) has been observed in group EN and subgroup VE. However, this difference was not statistically significant (p=0.231).
4. DISCUSSION
One of the important considerations in hypo-mineralized enamel is that the enamel defect is localized and can be differentiated from the surrounding healthy enamel so there is no need for extensive preparation. Regarding the minimal intervention concept, the occlusal veneer is suitable for young permanent teeth affected with MIH [17, 18]. Another thought in the restoration of endodontically newly erupted hypomineralized teeth is the minimum inter occlusal space, which affects the retention and strength of the restoration, and that there is no sufficient coronal structure, which thus decreases the retention of the full coverage restoration. Endocrown appears to be a suitable restoration in such cases as it obtains retention from the pulp chamber [6].
Full coverage crowns in the form of preformed metal crowns for rehabilitation of localized hypomineralized defects have been documented with acceptable results [19], and have a significantly higher survival rate than composite resin restorations [20]. The use of a glass hybrid restoration system, after 12 months of evaluation, has proven to be an effective approach to preserving the first permanent molars affected by MIH; however, the type of failure occurring in a restoration involves three or more surfaces presenting the breakdown of all cusps [21].
The literature is still trying to find another solution for the rehabilitation of severely MIH-affected molars using modalities other than full coverage crowns with special care for both biological and mechanical aspects. Partial coverage metallic restoration has also been recorded in the literature [22] and offers a good substitute for full coverage; however, the metal has a less acceptable esthetic appearance [17].
Nevertheless, the greatest restorative material is yet to be recognized. As the glass and hybrid ceramics include the biomimetic principles of conservation and esthetics together [10], a few investigations have been done to investigate the performance of these recent materials when utilized as minimal thickness posterior occlusal veneers and endocrowns. Therefore, the chief importance of the current in vivo investigation was focusing specifically on evaluating the clinical performance of different preparation designs (occlusal veneer and endocrown) fabricated from two types of CAD/CAM ceramic restorations (zirconia-reinforced lithium silicate glass ceramic “Vita Suprinity” and hybrid ceramic “Vita Enamic” restorations).
In the present study, the modified USPHS criteria have been used to evaluate the clinical performance of the materials as these criteria have proven to be reliable for the tooth-colored restorations in preceding studies [11, 21, 22]. For standardization, two independent examiners performed assessments using a grading system based on several observations (e.g., fracture, sensitivity, recurrent caries at the crown margin, marginal adaptation, and discoloration). The parameters (alpha as “perfect”, bravo as “less perfect”, and Charlie as “complete failure”) were chosen because they are considered the most important features to evaluate the clinical performance, and hence establish the treatment plan. In addition, plaque status was assessed using the plaque index. This index has proven to be an accurate and reproducible tool in clinical research [23].
The modified proposed occlusal veneer was prepared with standard dimensions to allow accurate control of the variables of the preparation dimensions, 1.5 mm reduction at the cusp tip with 1 mm at the fossa, supragingival circumferential chamfer finish line 1mm in width, as well as one shallow mesial slot (2mm width and 1.5mm depth) [10]. While the endocrown was prepared with 2mm occlusal reduction and divergence of the internal wall of the cavity at 8 degrees [15].
The outcomes of the current study can be briefed clinically with some clarifications. One of these clarifications is the fracture of the restorative material, which has been reported as the main cause of failure in partial indirect restorations in posterior teeth [24, 25]. No fractures in this study were observed, and this may be attributed to many factors, including the prober preparation technique for ceramic material and the adherence to manufacturer’s instructions, which lead to the absence of stress concentration areas. Clinical reports have determined a relevant role of occlusal forces in ceramic fractures and, consequently, a higher risk of failure in molars than in premolars [26, 27]. This result is compatible with preceding investigations in which no complete fractures have been reported [28, 29].
Secondary caries might be due to the MIH defect characterized by rapid and recurrent disintegration of the porous enamel that causes secondary caries [17]. This outcome is similar to the former investigation in which secondary caries was reported during the 1st year of recall time evaluation [30].
For marginal discoloration, the results have been found to be in agreement with the short-term preceding investigation that evaluated partial coverage of Vita Suprinity restoration at 12 months [31]. This discoloration might be attributed to the restoration procedure, the finishing and polishing procedure, and other exterior influences, such as the food types and beverages consumed. However, this material has still presented clinically acceptable margins [32].
Plaque accumulation may be due to several factors, for example, the patient’s hygiene behaviors, the patient’s bacterial flora, and periodontal maintenance [33]. This outcome is similar to a prior search that has evaluated the clinical performance of resin matrix partial coverage restoration [34].
Regarding the effect of preparation design regardless of ceramic material, the results have been found to be in accordance with former investigations that have shown no significant differences between endocrown restorations and zirconia crown restorations [15]. Concerning the effect of ceramic materials regardless of preparation design, results of former investigations have demonstrated no significant differences between zirconia-reinforced lithium silicate and polymer-infiltrated ceramic network restorations [31, 35].
In the current scientific search, the Kaplan-Meier analysis was used for survival and success assessment during the observational period of 18 months; occlusal veneer and endocrown designs fabricated from Vita Suprinity and Vita Enamic restorations exhibited a survival rate of 100%. All restorations remained in situ and in good function, which is consistent with preceding data of scientific literature [23, 29, 30]. The overall success rate for occlusal veneer restorations was 88% and 94% for endocrowns restorations, which is consistent with previous data published in scientific literature [31, 34]. Finally, the hypothesis of the study was accepted.
The current scientific search was not free of constraints and involved a small follow-up period; thus, variances among both CAD/CAM materials may become significant after a lengthier period of clinical service. No split-mouth design and no blinding or standardization were performed between the main groups due to different preparation designs related to different extents of the breakdown of hypomineralized molar. In addition, data on confounding factors, such as the number of affected teeth, hypersensitivity, and the involvement of permanent incisors, have not been included in the study’s results. In addition, a small number of patients participated in this research. Numerous clinical dissimilarities (restoration dimensions and intra-oral spreading) could act as cofounders.
CONCLUSION
Within the constraints of the current study, it can be concluded that in the rehabilitation of severe MIH-affected first permanent molar, both CAD/CAM zirconia-reinforced lithium silicate and hybrid ceramic restorations can be considered reliable materials for partial coverage restorations with reliable clinical performance within 18 months. Also, both occlusal veneer restorations and endocrown restorations are clinically accepted in the management of severely affected first permanent molar.
LIST OF ABBREVIATIONS
| MIH | = Molar incisor hypomineralisation |
| VS | = Vita Suprinity |
| EN | = endocrown |
| PMCs | = prefabricated metal crowns |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
In the present randomized prospective study, ethical board approval was obtained before the commencement of the study from the Ethical Committee of Al-Azhar University (REC-PD-22-10).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee, and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
All parents were asked to sign an informed consent after a detailed explanation of the procedures and possible outcomes of treatment.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
Declared none.

