All published articles of this journal are available on ScienceDirect.

Effect of Aging and Different Surface Treatments on Repair Bond Strength of Hybrid Resin Composites
Abstract
Background:
With the trend for minimally invasive dentistry and the rapid evolution of composite resin materials, repair of defective composite resin restorations is a popular choice rather than replacement of the restoration. The durability of the bond between the old and repaired composite restoration is important for a successful outcome.
Objective:
To evaluate the immediate and delayed shear bond strength of two types of repaired hybrid resin composites using different chemical and mechanical surface treatments.
Methods:
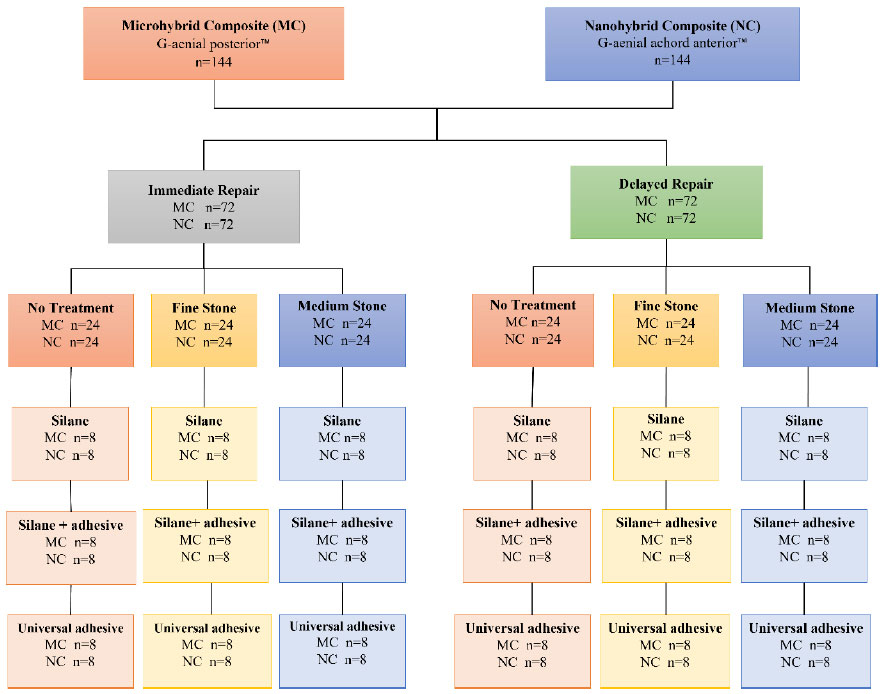
Two types of hybrid resin composites, micro-hybrid resin composite and nanohybrid resin composite, were used to prepare 288 pre-polymerized resin composite specimens. After polymerization, repair was done after 24 hours and 6 months. Each hybrid resin composite group was divided into 3 groups according to surface treatment used to repair the substrate: group 1: no surface treatment, group 2: treated by medium abrasive stone, and group 3: treated by fine abrasive stone. Each group was further subdivided into 3 subgroups according to different agents used for repair: group 1: Silane, group 2: Universal adhesive, and group 3: Silane + adhesive. Shear bond strengths of the repaired specimens were measured using a Universal testing machine. Failure modes were evaluated under a stereomicroscope.
Results:
Different chemical and mechanical surface treatments had a significant effect on the shear bond strength values of all groups (p ≤ 0.05). The highest mean shear bond strength values were found in nano-hybrid composites immediately repaired by silane after treatment by a medium abrasive stone while the lowest mean shear bond strength values were found in micro-hybrid composites with delayed repair and no surface treatment.
Conclusion:
Diamond burs using silane with adhesive improved the repair bond strength of the tested hybrid composites. In composite repair, using abrasive mechanical pretreatment followed by adhesive conditioning is crucial for the success of the repair restoration.
1. INTRODUCTION
Composite resin restorations are most commonly used as direct and indirect restorations due to the improvement in the clinical performance of these materials and the development of new adhesive systems. Moreover, the enhanced esthetic outcome and non-invasive conservative treatment approach, as well as satisfying mechanical properties, have made them a popular choice. However, these restorations are subjected to failure due to fracture, caries or discoloration, and the treatment of choice is either complete replacement or repair of the existing restoration. Since minimally invasive intervention has become an important aspect of modern adhesive dentistry, total replacement is undesirable as it is more time-consuming and less conservative. Hence, repair is the better solution in these cases whenever possible [1].
Repair is done by placing a new resin composite over the old one. A good bond between old and new composites is very important for the success of repair and many studies stated that it is unpredictable. This is because the durability of the bond between the existing and repaired resin composite becomes compromised due to water uptake, leaching of the constituents, and enzymatic degradation of the restoration surface [2].
In case of immediate repair, there is an oxygen-inhibited layer containing unreacted acrylate groups, which enhances bonding between the newly polymerized composite and the old composite restoration. While in the case of delayed repair, there is no oxygen-inhibited layer and no unreacted groups for bonding between aged composite and fresh composite, which represents a great challenge [3]. Indeed, studies have consistently found lower repair bond strength values for aged composites compared to fresh composites [4,5].
Different types of surface treatments (chemical and mechanical) and adhesive systems were evaluated to assess the bond strength of repaired resin composites, and it was found that surface roughness had a great effect. Using diamond burs or sandblasting along with bonding agents produced a greater effect than using bonding agents alone [6, 7]. Many researches have been undertaken to investigate the highest quality repair protocols and bonding techniques; however, there still exists a gap between experimental strategies and those used in day-to-day restorative practice [8-10].
Although many studies have investigated the bond strength of repaired composite resin, different composite materials are evolving, and the improvement in the adhesive systems has led to newer materials being introduced in the market. Indeed, GC Corporation Tokyo, Japan introduced new nano and micro-hybrid resin composites: G-ӕnial achord anterior ™ and G-ӕnial posterior ™, respectively, which provide improved mechanical and physical properties compared to conventional resin composites that have been extensively tested in the literature. The quantity and the dispersion of the fillers in these new materials may play a role in enhancing their performance from a mechanical point of view. Thus, the aim of this study was to compare the effect of different mechanical surface treatments, bonding agents and filler size on the immediate and delayed repair bond strength of two new hybrid resin composites. The null hypothesis is that there is no difference between the different mechanical surface treatment and bonding agents and filler size on the immediate and delayed repair bond strength of the two hybrid resin composites.
2. MATERIALS AND METHODS
2.1. Specimen Preparation
The sample size was calculated using G-power 3.1.9.7(8). At least a sample size of 8 should be used to determine a difference at 5% significance. The effect size was 0.4, α=0.05 and Power (β) of 0.85. According to this, two hundred eighty-eight specimens were prepared from two types of hybrid resin composite, one hundred forty-four specimens from micro-hybrid resin composite, namely G-ӕnial posterior ™(GC Corporation Tokyo, Japan) and one hundred forty-four from nanohybrid resin composite namely G-ӕnial Achord ™(GC Corporation Tokyo, Japan), and used as pre-polymerized resin composite specimens. The specimens were fabricated by placing the uncured resin composite in a mold with dimensions 14×14 and 2 mm height. The surface was covered with a mylar strip to create a smooth, flat, polished surface to ensure standardization of the specimen surface. Then, photopolymeri-zation was done using an LED polymerization unit (Ivoclar Vivadent Inc., Amherst, N.Y., USA) of 1200 mW/cm2 for 20 sec. All the steps were done by the same operator. Table 1 illustrates the materials used in the study.
| Material | Manufacturer | Composition | Lot Number |
|---|---|---|---|
| Micro-hybrid resin composite G-ӕnial posterior ™ |
GC Corporation Tokyo, Japan |
Methacrylate monomers (a mixture of urethane dimethacrylate (UDMA) and dimethacrylate co-monomers. G-ænial is bis-GMA free). Pre-polymerized filler 16-17 µm (silica containing-strontium lanthanoid fluoride containing: Inorganic filler >100 nm(flouroaluminosilicate) Inorganic filler<100 nm (fumed silica). Trace pigments and catalysts. The particle size of the filler of 0.7-2 μm |
2108261 |
| Nanohybrid resin composite G-ӕnial Achord anterior ™ |
GC Corporation Tokyo, Japan |
Methacrylate monomers (a mixture of urethane dimethacrylate (UDMA) and dimethacrylate co-monomers. G-ænial is bis-GMA free). Pre-polymerized filler 16-17 µm (silica containing-strontium lanthanoid fluoride containing: Inorganic filler >100 nm(silica). Inorganic filler <100 nm (fumed silica). Trace pigments and catalysts. Particle size is a range of micro and nano-sized filler 0.3-1 µm and 0.02-0.05μm respectively |
2106171 |
| Universal Adhesive Prime & Bond Universal ™ |
Dentsply Sirona, USA | PENTA(dipentaerythritol pentacrylate phosphate) and MDP, BisGMA and HEMA, Water-Isopropanol solvent | 2204000699 |
| Silane Porcelain Primer ™ |
BISCO, Inc. Schaumburg, IL The USA. |
Pre-hydrolyzed no-mix silane primer and Bis-Silane | 2200002145 |
2.2. Shear Bond Strength Test
After polymerization, half of the total prepared resin composite specimens for both types were stored in distilled water for 6 months for delayed repair (G-ӕnial posterior™ n=72, G-ӕnial Achord™ n=72). The other half of the prepared resin composite specimens were immediately repaired after 24 hours with the same hybrid resin composite using a hollow translucent polyethylene tube of 3 mm in diameter and 2 mm thickness. Each hybrid resin composite group was divided into 3 groups according to surface treatment used to repair the substrate as follows: group 1: twenty-four pre-polymerized substrate specimens were left intact with no surface treatment. Group 2: twenty- four pre-polymerized substrate specimens were treated by medium abrasive stone with grit size 107-126 μm (Kenda Dental Polishers™, Germany), group 3: twenty-four pre-polymerized substrate specimens were treated by fine abrasive stone with grit size 20 µm (Kenda Dental Polishers™, Germany),
Each group was further subdivided into 3 subgroups consisting of 8 specimens each according to different agents used for immediate repair, group (a): silane (Porcelain Primer™, Bisco, Schaumburg, USA), group (b): universal adhesive (Prime & Bond Universal™, Dentsply Sirona, USA), group (c): silane (Porcelain Primer™, Bisco, Schaumburg, USA) + adhesive (Prime & Bond Universal™, Dentsply Sirona, USA), as shown in Fig. (1).
For the delayed repair specimens, the pre-polymerized substrate specimens were repaired in the manner explained previously for immediate groups. The repaired specimens were stored in distilled water at 37°C for 24 h. After 24 h, specimens were subjected to a shear bond test using a Hounsfield Universal testing machine (Instron, USA) at a cross-head speed of 1 mm/min. The results were statistically analyzed.
2.3. Stereomicroscope Examination
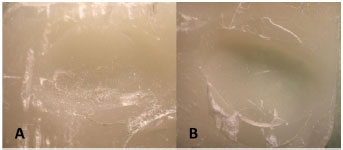
The debonded, fractured surfaces of the samples were evaluated at 20× magnification stereomicroscope (Olympus SZX16, Olympus, Tokyo, Japan.) to identify the failure mode, which was classified into one of the following categories: mixed, adhesive, and cohesive. Mixed failure was considered when both the adhesive interface and the composite material were involved (pre-polymerized specimens or newly repaired material). Adhesive failure was considered if it was observed at the resin/adhesive interface while cohesive failure was identified if it occurred within the old composite substrate or the newly repaired composite.
2.4. Statistical Analysis
Numerical data were assessed for normality by checking the data distribution. The mean and median values were calculated and Shapiro-Wilk tests were used for analysis. Mean and standard deviation (SD) values were used to represent the data due to parametric distribution. The effect of different tested variables and their interaction were evaluated using Three-way ANOVA. Main and simple effects were compared utilizing pairwise with Bonferroni correction. The significance level was set at p≤0.05 within all tests. Statistical analysis was performed with IBM® (IBM Corporation, NY, USA) SPSS® Statistics Version 26 for Windows (®SPSS, Inc., an IBM Company).
3. RESULTS
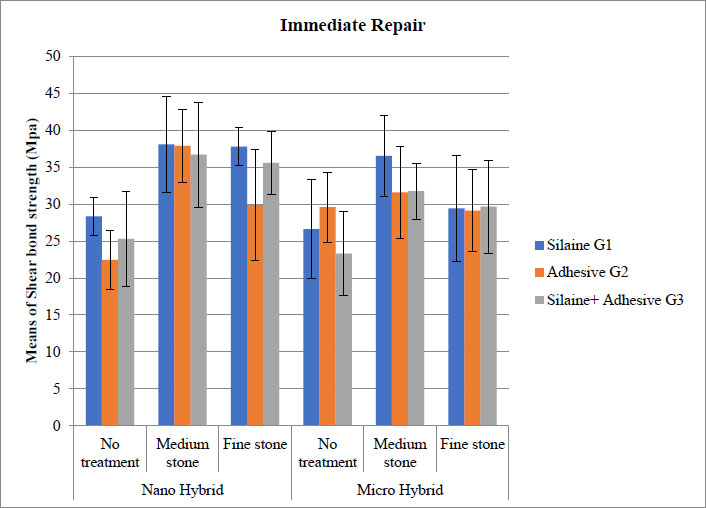
The mean shear bond strength (SBS) measured by Mega Pascal (MPa) values with a standard deviation of all the main groups are displayed in Figs. (2 and 3). When comparing the SBS values for the immediate repair groups, the highest mean SBS value was recorded for the nanohybrid composite group immediately repaired by silane after treatment by a medium abrasive stone 38.09 ± 6.50. This was followed by the nanohybrid composite group immediately repaired by universal adhesive after treatment with medium abrasive stone 37.88 ± 4.95, then the nanohybrid composite group immediately repaired by silane after treatment with fine abrasive stone 37.80 ± 2.60. The lowest mean SBS was recorded for the micro-hybrid composite group immediately repaired by silane and universal adhesive with no surface treatment 23.31 ± 5.65 (Table 2).
| Materials | Surface Treatment | Time Interval |
Silaine G1 (n=8) |
Adhesive G2 (n=8) | Silaine+ Adhesive G3 (n=8) |
|---|---|---|---|---|---|
| Nano Hybrid | No treatment | Immediate | 28.35 ± 2.54abcdef | 22.44 ± 4.03ef | 25.29 ± 6.43ef |
| Delayed | 27.22 ± 2.69cdef | 21.44 ± 4.03f | 26.16 ± 6.10def | - | |
| Medium stone | Immediate | 38.09 ± 6.50a | 37.88 ± 4.95ab | 36.69 ± 7.13abc | |
| Delayed | 28.71 ± 4.78abcdef | 31.38 ± 5.71abcdef | 31.31 ± 6.85abcdef | - | |
| Fine stone | Immediate | 37.80 ± 2.60ab | 29.86 ± 7.55abcdef | 35.58 ± 4.23abcd | |
| Delayed | 30.05 ± 6.35abcdef | 29.61 ± 7.50abcdef | 29.20 ± 4.72abcdef | - | |
| Micro Hybrid | No treatment | Immediate | 26.63 ± 6.72cdef | 29.58 ± 4.71abcdef | 23.31 ± 5.65ef |
| Delayed | 22.76 ± 4.43ef | 27.08 ± 2.64cdef | 22.93 ± 5.20ef | - | |
| Medium stone | Immediate | 36.53 ± 5.50abc | 31.60 ± 6.20abcdef | 31.76 ± 3.77abcde | |
| Delayed | 30.28 ± 2.38abcdef | 30.35 ± 4.70abcdef | 30.26 ± 1.76abcdef | - | |
| Fine stone | Immediate | 29.42 ± 7.14abcdef | 29.14 ± 5.55abcdef | 29.66 ± 6.30abcdef | |
| Delayed | 27.67 ± 5.70bcdef | 29.01 ± 5.70abcdef | 28.41 ± 4.61abcdef | - |
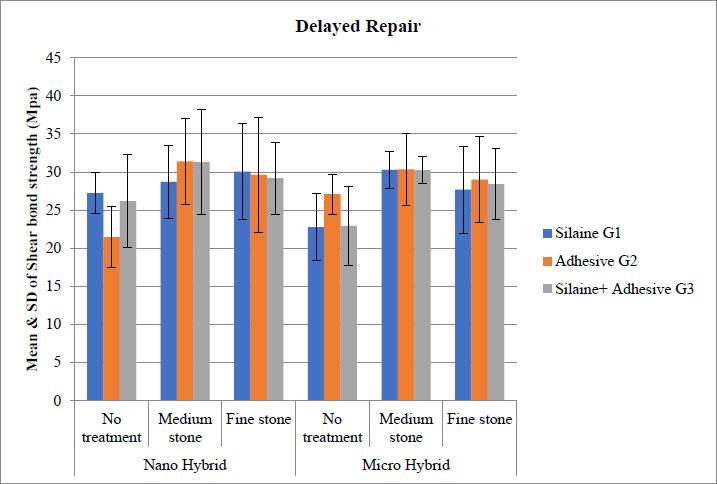
When comparing the SBS values for the delayed repair groups, the highest mean SBS value was recorded for the nanohybrid composite group repaired by adhesive after treatment with medium abrasive stone 31.38 ± 5.71. Followed by the nanohybrid composite repaired by silane + universal adhesive after treatment by medium abrasive stone 31.31 ± 6.85. The lowest mean bond strength values were displayed in the micro-hybrid composite repaired by silane and universal adhesive with no surface treatment 22.93 ± 5.20 (Table 2).
When comparing immediate and delayed repair groups together, higher SBS values were found in the immediately repaired groups compared to delayed repair groups, with a statistically significant difference between them (p = 0.03).
The nanohybrid composite for both immediate and delayed groups showed higher means SBS values compared to the microhybrid composite with a statistically significant difference between them (p =0.013).
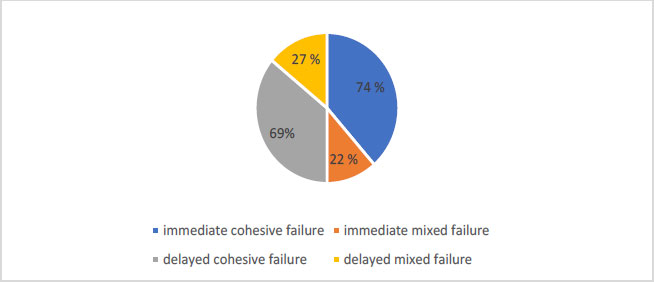
Failure modes in the immediately repaired groups displayed 74% (n=106) cohesive failure (Fig. 4A), while 22% (n=32) showed mixed failure (Fig. 4B). In the delayed repair group, 69% (n=100) showed cohesive failure, while 27% (n=39) showed mixed failure. No adhesive failure was identified. Failure modes are illustrated in Fig. (5).
Different small letters indicate significant difference at (p<0.05) among means, using Bonferroni correction for multiple comparisons
4. DISCUSSION
The null hypothesis stating that there is no difference between the different mechanical surface treatments, bonding agents, and filler size on the immediate and delayed repair bond strength of the two hybrid resin composites was rejected.
The trend towards minimal invasive dentistry means that more failing resin composite restorations are repaired rather than replaced. However, composite repair represents a challenge, as the bond between the old and new composites is very important for the success of repair [1].
Mechanical and/or chemical surface treatments were used to improve the repair bond strength of resin composites by roughening the surface. Mechanical surface treatment can be done by diamond bur [10], carbide bur, green carborundum stone, air abrasion with 50 µ aluminum oxide particles and silicon carbide paper [6, 7, 11, 12]. Chemical surface treatment involves the use of acid etching with 37% phosphoric acid gel, hydrofluoric acid, and 1.23% acidulated phosphate fluoride gel. This increases the surface area for adhesive resin bonding, hence improving the repair bond strength [13-16].
The surface treatment on an existing composite resin is intended to remove the superficial layer altered by saliva and increase the surface area available for bonding by creating surface irregularities [17, 18]. Hence, in this study, medium and fine abrasive diamond burs were used to roughen the surface mechanically. Previous studies concluded that this pretreatment provided the highest composite resin repair bond strength compared with roughening with different grit diamond rotary instruments [19, 20].
It was found that using bonding agents improved the repair bond strength of resin composites [21]. In this study, a universal adhesive (Prime & Bond universal ™, Dentsply Sirona) was tested. This was because most clinicians prefer to use the adhesive system already used in their daily clinical work rather than purchasing a special type for the repair procedure. The universal adhesive has become increasingly popular among the various types of adhesive systems due to convenience and improved performance. Additionally, it is the most simplified system that combines the functions of an etchant, primer, and adhesive into a single bottle that can be used in both self-etching and etch-and-rinse (total-etch) modes. Prime & Bond universal is a new version indicated for adhesion on different substrates containing MDP, which may enhance bonding quality [22].
A silane coupling agent (Porcelain Primer BISCO, Inc.Schaumburg, IL USA.) was also evaluated in this study as pre-hydrolyzed no-mix silane prime. Several studies found that silanization of resin composites before adhesive application improved the repair bond strength [23, 24] where silanes contain (1) silanol groups, which react with exposed inorganic filler particles of the old polymerized composite and (2) organofunctional groups, which react and co-polymerize with methacrylate groups of the repair material which means that using silane increases the reactivity of the surface and increases the wettability of the substrate and enhances diffusion of the bonding agent [25-27].
The results of this study showed that the highest mean SBS values were recorded in the nanohybrid composite groups immediately repaired by silane or universal adhesive after treatment by medium abrasive stone or fine abrasive stone. These results can be attributed to the surface irregularities created by the diamond abrasives that create a rough retentive surface, so the new composite interlocks with the pre-polymerized composite.
The micro-mechanical roughening produced by these abrasives depends on the abrasive particle size. Medium abrasive is 107-126 μm and fine abrasive is 20 μm. Hence, more surface roughness is expected of the medium abrasive stone. This explains the higher bond strength obtained by groups using medium abrasive stone.
Additionally in the clinical situations, these abrasives remove the superficial chemically altered surface due to exposure to saliva, resulting in a high surface energy surface of pre-polymerized composite. The result in this study is in agreement with other studies which found that surface roughness increases surface energy and creates mechanical interlocking in the substrate [6, 18]. Indeed, micro-retentive interlocking is the most critical factor in establishing a bond between old and repaired composites [20, 28, 29].
The results of this study showed that immediate repair SBS was higher than delayed SBS, with a significant difference between them. This can be attributed to the presence of free radicals which is important for adhesion between composite increments. The maximum activity of these free radicals is present during the first 24 hours after the polymerization of the composite [30]. This is in agreement with other studies which concluded that immediate repair bond strength was higher than the delayed one [31, 32].
Although the filler phase content plays an important role in the properties of resin composites, filler phase size and its distribution also affect the performance of dental composite materials. The results of this study showed that the nanohybrid composite in both intervals showed higher means of SBS values than the micro-hybrid composite, with statistically significant differences between them. This can be attributed to the filler size and distribution, which affects the degree of light scattering during photo-polymerization of the resin composite by the light cure unit. This increase in light scattering reduces the light intensity passing through the substrate, resulting in a lower degree of conversion (DC) and depth of cure. So, micron-sized filler particles increase the light scattering that leads to lower DC, while for nano-sized filler particles, a decrease in size reduces the light scattering, hence increasing the DC [33, 34].
This is an in-vitro study and clinical evaluation of composite resin restoration repair is essential as composite restorations intra-orally are exposed to pH changes, salivary enzymes, water sorption, and other factors that may alter the composition of the material and hence influence the repair bond strength. Further in-vitro investigations may include various protocols of intraoral repair systems including the potential of indirect aesthetic restorations, ceramic, feldspathic porcelain, and zirconia.
CONCLUSION
Immediate repair of resin composite restorations exhibited higher SBS compared to delayed repair. Furthermore, the smaller filler size of the nanohybrid composites displayed higher SBS compared to micro hybrid composites. Mechanical treatment of the composite surface using medium diamond burs followed by fine ones improved the repair bond strength of the tested hybrid composites. Mechanical pretreatment followed by adhesive conditioning is the key to the success of composite repair.
LIST OF ABBREVIATIONS
| UDMA | = urethane dimethacrylate |
| MC | = Microhybrid Composite |
| NC | = Nanohybrid Composite |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was gained from Ain Shams University Ethics Committee NO. (FDASU-Rec IR 042312). Consent to participate is not applicable in this study.
HUMAN AND ANIMAL RIGHTS
No humans/animals were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the current study are available from the corresponding author [D.H] on reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

