All published articles of this journal are available on ScienceDirect.

Common Temporization of Access Cavity and Pulp Spacers Practiced by Endodontists in Saudi Arabia: A Cross-sectional Study
Abstract
Background:
Temporary restorations are necessary for preventing coronal leakage during and after treatment completion and must provide an effective barrier against salivary contamination of the root canal system. Endodontic spacers also help remove temporary restoration by avoiding the chances of unwanted intact tooth structure loss and perforation on the floor of the pulp chamber and prevent temporary restorative materials entrapment into the root canals resulting in canal blockage. However, the cotton pellet placed between the temporary and the root canal orifice can compromise the coronal seal by the reduction in thickness of temporary restoration.
Objective:
The primary aim of this investigation was to determine the most common temporary restoration used during and after endodontic treatment. The secondary aim is to know the percent preference for restorations with double seal and the frequency of spacer used.
Methods:
Four hundred fifty online questionnaires comprising 15 (four demographic questions and eleven questions related to the study objective) were sent to endodontists in Saudi Arabia via WhatsApp and Twitter. Statistical significance was set at P<0.05 when assessed using a chi-square test.
Results:
About 370 (82.22%) participants completed the survey. Glass ionomer cement (GIC) was most used as a temporary restoration among endodontists for both the anterior (53%) and posterior teeth (49.7%; P=0.001). In double seal, Cavit was most used as the temporary restoration, which was placed below the seal exposed orally 56.2% (P=0.001). GIC was most used as coronal seal material placed over Cavit in 71.9% of the participants (P=0.001). About 56.2% of the endodontists placed cotton pellets between visits but not after obturation (P=0.001). Polytetrafluoroethylene tape instead of cotton pellet was preferred by 30.3% of the participants (P=0.001).
Conclusion:
Glass ionomer cement (GIC) was most used as a temporary restoration. In double seal, GIC was most used as coronal seal material placed over Cavit. A pulp spacer was found to be the most commonly used between visits but not after obturation.
1. INTRODUCTION
To achieve a successful outcome in endodontic treatment, root canals need to be properly cleaned and shaped to remove debris and microorganisms; subsequently, the root canals should be sealed completely [1]. Temporary restorations are necessary to prevent coronal leakage during and immediately after treatment completion. Restoration materials temporarily seal the tooth and prevent the entry of debris, fluids, and microorganisms into the canals. Moreover, they prevent the escape of medications inserted in the pulp chamber and root canal system and aid in their retention. Coronal leakage is a major cause of root canal failure [2]. Unsatisfactory temporary restorations are ranked second among the factors associated with continuing pain after the initiation of endodontic treatment [3].
According to an in vitro investigation, no known obturation technique can ensure an impenetrable seal against leakage [4]. According to a few studies, coronal restoration is an essential factor determining the success of root canal treatment [5, 6]. A temporary restoration should be placed between the appointments to seal the endodontic access cavity and prevent microbial contamination attributed to oral fluids [7]. Temporary restorations are commonly placed after the completion of endodontic treatment and before the placement of the definitive restoration [7].
Temporary materials placed between the appointments or immediately after the root canal procedure cannot provide an impervious barrier for a long time. According to Balto [8], a vitro study evaluated the microbial leakage of Cavit (3M ESPE Dental AG, Seefeld/Ober- bay, Germany), Intermediate restorative material (IRM; L. D. Caulk Co., Milford, DE, USA), and Dyract (Dentsply-De Trey, Konstanz, Germany) when used as temporary filling materials after root canal treatment. Intermediate restorative material started to leak after 10 days, whereas Cavit and Dyract leaked after 2 weeks [8]. Cavit has been reported to have superior hardness, dimensional stability, and seal when compared with Cavit [7], which may affect the durability of the temporary filling and microbial contamination of the access cavity. A good-quality coronal restoration significantly increased the odds of success by 11-fold [9]. The concept of a ‘double seal’ has also been described in the absence of a single ideal restorative material. A double seal is the placement of two temporary materials in the access cavity to gain the advantages of both materials, such as the sealing ability of one material and the strength of another [10].
Several investigators have examined the leakage of temporary restorative materials using various methods, including dyes [11, 12], radioisotopes [13, 14], bacteria penetration methods [15, 16], and fluid filtration [17, 18]. Most of the studies that examined the effectiveness of these materials used artificial conditions, which were not representative of clinical conditions [19].
Cotton pellets, which are commonly placed beneath temporary fillings, aid in the removal of the temporary restoration, and help in identifying the root canal orifices and preventing unwanted materials from entering and blocking the canal space [20, 21]
Dentists, restorative dentists, and prosthodontists preferred that endodontists place cotton pellets in the pulp chamber. Dillard et al. [22], in a survey of licensed endodontists, reported that 62.5% of general practitioners and 80% of restorative dentists preferred using cotton pellet as pulp spacer when the endodontist finished the root canal treatment to facilitate the temporary filling removal. Placement of cotton pellets in the pulp chamber can decrease the thickness of the temporary restoration, which compromises the coronal seal. Ideally, access spacers should enhance or at least not compromise the sealing ability of the temporary restoration [23].
A thick interim restoration of more than 4 mm is required for effective sealing [24]. However, the spacer acts as a cushion permitting material deterioration upon mastication and entraps fibers at the margins of the restoration, which compromises the coronal seal [25, 26]. Previously, the quality of the temporary restoration seal was shown to significantly decrease by small amounts of cotton trapped in between the glass tube wall and temporary restoration materials [25]. An ideal temporary restoration should ensure easy and convenient placement and removal, minimize bacterial leakage, and inhibit bacterial growth [27]. It should also be inorganic, inexpensive, readily available, and autoclavable with a minimum volume [28].
Since the use of a cotton spacer also poses a clinical problem, the frequency of using double seals is less practiced among the diplomats of the American Board of Endodontists [20].
The primary aim of this investigation was to determine the most common temporary restoration used during and after endodontic treatment. The secondary aim was to know the percent preference for restorations with double seals and the frequency of spacer use.
2. MATERIALS AND METHODS
2.1. Study Population and Sample Size
This cross-sectional study was conducted according to the World Medical Association Declaration of Helsinki guidelines after approval from Majmaah University for Research Ethics Committee (MUREC) (HA-01-R-088). An online survey was conducted via Twitter and WhatsApp from January 1, 2022, to March 1, 2022, among active endodontists registered with the Saudi Commission of Health Specialties.
A total of 450 online questionnaires were sent to endodontists in Saudi Arabia. In the sample size calculation, considering the assumption that 50% of the participants in the study population have the factor of interest (i.e., they know the possible pulp spacer complications), the study needed a sample of 370 participants for estimating the expected proportion along with 5% absolute precision and 95% confidence.
This sample size was calculated using the following formula:
 |
where z is the z score, ε is the margin of error, n is the sample size required, and P is the assumed prevalence ratio.
The questionnaires used were pretested and adapted from previous studies [20, 22, 29]. Informed consent ensured strict voluntary participation; moreover, it included information regarding the type of questions and expected time needed and comprised four demographic questions (nationality, qualification, experience years, and graduation place) and 11 questions related to the study’s objectives concerning the use of temporary restorations in endodontic treatment (temporary material used to close anterior and posterior access openings; when using cotton pellet under temporary restoration; the primary, secondary, and tertiary reasons are for using cotton pellet after obturation; the primary and secondary reasons are for not using cotton pellet after obturation; the material used instead of cotton pellet placed under the temporary restoration after obturation; the temporary material used for a double seal; and whether referring dentists, restorative dentists, and prosthodontists prefer endodontists to place cotton pellet in the pulp chamber between the gutta-percha and temporary restoration).
This study was reported in accordance with the STROBE guidelines.
2.2. Statistical Analyses
In the present study, data were entered into Microsoft Excel 2007 (Microsoft Corp., Redmond, WA, USA) and analyzed using SPSS 23.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics investigated the relationship between demographic variables and practiced techniques. The difference between responses was assessed using the chi-square test at P-values <0.05. In general, the chi-square test statistic is calculated as follows:
 |
The questionnaire surveyed endodontists regarding the most common temporary material used in both the anterior and posterior teeth for sealing the access opening. In addition, endodontists were asked whether they traditionally used a double seal filling and whether they intentionally preferred cotton pellets in the form of spacers.
3. RESULTS
A high response rate of 369 (82%) was achieved in the study. Most of the participants comprised Saudi endodontists (62.70%). Whereas 48.9% of the total participants were board-certified (P=0.001; table 1).
Glass ionomer cement (GIC) was most used as a temporary restoration among endodontists for both the anterior (53%) and posterior teeth (49.7%; P=0.001). None of the participants used amalgam as the temporary filling material (Fig. 1).
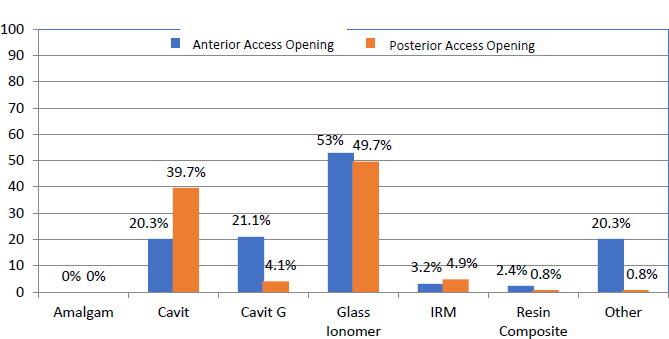
IRM, intermediate restorative material.
| Nationality | N % |
|---|---|
| Saudi | 138 (37.30%) |
| Non-Saudi | 232 (62.70%) |
| Place of Graduation | - |
| Saudi Arabia | 196 (52.97%) |
| East Asia | 67 (18.10%) |
| North America | 39 (10.54%) |
| Europe | 25 (6.75%) |
| Others | 24 (6.48%) |
| Middle East | 19 (5.13%) |
| Qualification | - |
| Diploma in Endodontics | 6 (1.6%) |
| Board-certified | 181 (48.9%) |
| Masters | 162 (43.8%) |
| PhD | 21 (5.7%) |
| Years of experience in the field of endodontics | - |
| 0 to 5 years | 126 (34.1%) |
| 6 to 10 years | 150 (40.5%) |
| 11 to 15 years | 49 (13.2%) |
| More than 16 years | 45 (12.2%) |
| Cotton Pellet Used | N % |
|---|---|
| Yes, between visits and no, after obturation | 208 (56.2%) |
| No, between visits and yes, after obturation | 0 (0%) |
| Yes, between visits and after obturation | 66 (17.8%) |
| Not at all | 96 (25.9%) |
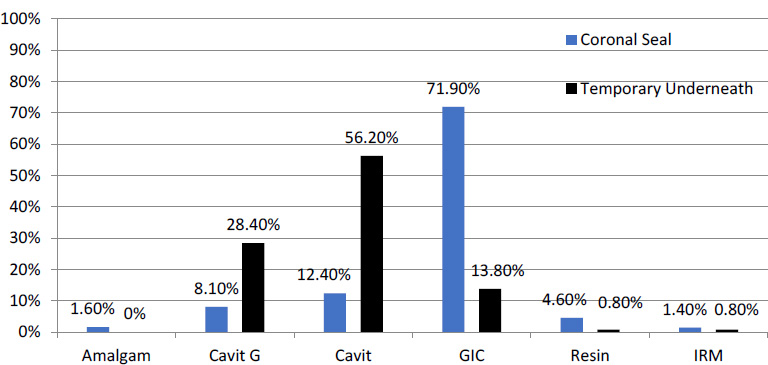
Double sealing was preferred by 4% of the participants (16 of 370) for the anterior teeth and 66% (248 of 370) for the posterior teeth (P=0.001). In the double sealing technique, Cavit was most commonly used as the temporary restoration, which was placed below the seal exposed orally at 56.2% (P=0.001). GIC was the most commonly used coronal seal material placed over Cavit in 71.9% of the participants (P=0.001; Fig. 2).
A total of 56.2% of endodontists placed cotton pellets between visits but not after obturation (P=0.001; table 2).
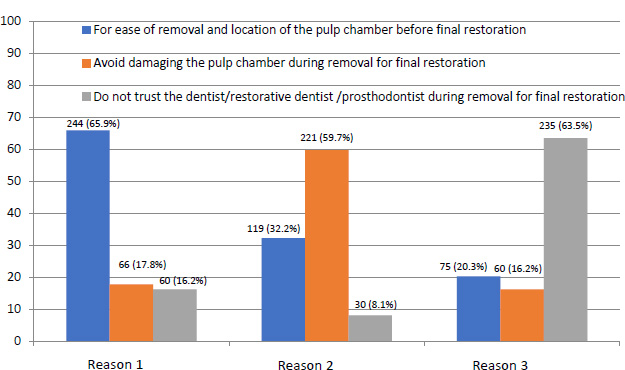
The primary reason for placing cotton pellets after obturation was easy removal of the restoration and locating the pulp chamber before the final restoration among 65.9% of the participants, whereas the secondary reason was to avoid damage to the pulp chamber during removal of the final restoration among 59.7% of the participants (P=0.001; Fig. 3).
A total of 66.5% of the endodontists did not prefer placing any material as a spacer beneath the temporary restoration after obturation (P=0.001). When the preferred material used as a spacer is considered, polytetrafluoroethylene tape instead of cotton pellet was preferred by 30.3% of the participants (P=0.001; table 3).
The primary reason for not placing cotton pellets after obturation was the deterioration of the sealing quality of the temporary restorations (leakage complication), as stated by 87.8% of the participants (P=0.001). The secondary reason was the weakening of the temporary restoration, as stated by 70.8% of the participants (P=0.001; Fig. 4). No significant difference was observed in the number of samples between the polytetrafluoroethylene (PTFE) and cotton pellet at days 7 and 14 (P > 0.05). However, on days 21 and 30, the number of leaked samples was significantly higher for the cotton pellet group (P < 0.05) [23].
A total of 68.4% of the dentists, restorative dentists, and prosthodontists preferred when endodontists placed cotton pellets in the pulp chamber (between the gutta-percha and temporary restoration) (P=0.001).
| Pulp Spacer | N (%) |
|---|---|
| Sponge | 6 (1.6%) |
| Poly-tetrafluoro-ethylene (Teflon) tape | 112 (30.3%) |
| Foam pellet | 6 (1.6%) |
| Nothing | 246 (66.5%) |
4. DISCUSSION
Loss of coronal seal due to fracture or loss of a restoration which may lead to coronal leakage can be overlooked by the patient for months since root-filled teeth lack the sensory innervation of the pulp. Therefore, it is important to regularly review root-filled teeth to prevent coronal leakage and monitor the periradicular status. The existence of gaps between the cavity wall and the temporary restoration can affect its marginal integrity and lead to leakage [30]. The type of restorative material selected to temporize the pulp chamber during and after endodontic treatment is based on the extent of the cavity, the anticipated duration of the restoration, and the characteristics required [31]. A temporary restorative material should provide an adequate seal for preventing fluids, bacteria, and organic materials from entering the root canals while impeding intracanal medicament seepage. Furthermore, temporary restorative materials should allow ease of placement and removal and provide esthetic value while protecting the tooth during the treatment. Generally, temporary restoration failure can be attributed to insufficient thickness of the material, its incorrect placement, and failure to evaluate the occlusion after its placement [19].
The survey was distributed to endodontists through social media applications, such as Twitter and WhatsApp. A similar method was used by Alroomy [32]. A good response rate was achieved in recruiting participants. The data collection method used for the participants was effective since every participant could directly communicate with the researchers.
In the present survey, cotton pellet was the most common pulp spacers used between visits, as stated by 56.2% of the participants. Similar findings were reported by Algahtani et al. [29]. They surveyed the temporization techniques practiced in Saudi Arabia by general dentists, dental specialists, and clinical trainees in undergraduate and postgraduate dental programs; however, only endodontists were surveyed in the current study. An in vitro study compared the effectiveness of cotton pellet, cellulose sponge, and PTFE tape as pulp spacer material. When used with medicament, cotton was the best followed by cellulose sponge. While in test groups where no medicament was used, PTFE tape was the most effective, and cotton showed the least potential against preventing bacterial uptake [33]. Placement of a cotton pellet below the temporary restoration is considered a common practice since it helps in the removal of the temporary restoration and facilitates the identification of the root canal orifices [20]. The cotton pellet should be of sufficient thickness to prevent the lodgment of temporary material inside the canals and simplify the access for endodontic procedure and restoration. Concurrently, it should also be thin enough to permit adequate space with the cavosurface margin of the access cavity. This space allows the placement of a sufficient thickness of the temporary material.
In our study, most of the endodontists (66.5%) chose not to use cotton pellets or any material as a spacer beneath the temporary restoration after obturation. According to AlSwayyed et al., 61% did not place a cotton pellet as a pulp spacer [34], while 5.7% of endodontists in Saudi Arabia chose not to place a spacer material. Barriers against bacterial leakage could increase when nothing is placed under the restorative material [25].
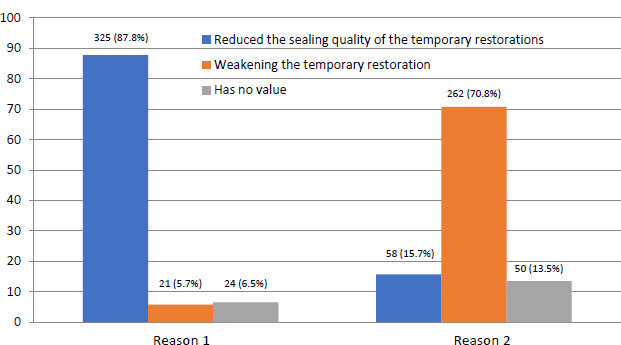
In our study, the most common reason for not placing a cotton pellet below the temporary filling was the deterioration of the sealing quality of the temporary restorations (leakage complication), followed by weakening of the temporary restoration (Fig. 4). Thus, the cotton pellet could act as a cushion, leading to material degradation during mastication and entrapped fibers at the restorative margins (Wick effect), thereby compromising the seal of the temporary restoration [25, 26]. The wicking effect of cotton might increase coronal leakage.
In our study, 30.3% of the respondents used polytetrafluoroethylene (Teflon) tape instead of cotton pellets, which is a higher rate than that reported by Algahtani et al. [29]. Based on accumulating evidence, polytetrafluoroethylene tape seems to be a superior alternative spacer material [35, 36]. An ex vivo study using micro-computed tomography determined the percentage volume of gaps and voids along the margins and within the Cavit restoration. The result of this study was that the type of spacer material placed beneath the Cavit restoration could influence the quality of temporization. The Polytetrafluoroethylene (Teflon) tape spacer was associated with a lower potential for gap formation between the Cavit restoration and the access cavity walls compared with the cotton pellet [37].
Dentists, restorative dentists, and prosthodontists preferred when endodontists placed cotton pellets in the pulp chamber (between the gutta-percha and temporary restoration), as endodontists reported in this survey. In a previous study [22], 62% of general dental practitioners and 80% of endodontists preferred using a cotton pellet as a spacer.
The use of GIC as a temporary restoration in endodontic procedures has been studied [38]. A study that applied the fluid filtration technique found that the leakage values of GIC after 8 weeks were not significantly different compared with those in the intact crown values [38]. Another study also determined the use of GIC as the temporary restoration in 32% of the participants [29]. The antibacterial property of this material is attributed to its low pH and fluoride release, along with the presence of cations, such as strontium or zinc, in some of the cements. Owing to these favorable properties, GIC can be used as a suitable temporary restorative material in cases that need temporization for a longer time. It is one of the preferred materials for temporary restoration between visits [29]. GIC can chemically bond to enamel and dentine, which provides an efficient coronal seal. It also releases fluoride and re-absorbs fluoride from the oral environment.
The double seal technique, which combines the advantages of two types of temporary restorations to overcome the disadvantages of each individual type, was the most commonly used method to achieve a coronal seal [34]. In this study, it was found the double seal was the most commonly used technique following obturation, which involved placing Cavit in the deeper layer of the pulp chamber. Then, GIC was used in the outer layer that was exposed to the oral cavity. It was found that this combination was the most commonly used coronal restorative technique among restorative dentists and endodontists in Saudi Arabia; also, it was the most widely used technique across dentists with all clinical titles, as approximately 56% of all the patients were restored utilizing this technique [34].
Endodontists most frequently use GIC for both the anterior and posterior teeth following obturation. GIC is the most commonly used temporary filling material for the posterior teeth [39] because of the need for a good sealing quality of the temporary restorations (leakage complication). The regularly employed temporary restorative materials, such as intermediate restorative material (IRM) or Cavit, used between appointments, showed higher coronal leakage than GIC [40]. Cavit and IRM have routinely withstood testing and routine evaluation and can be used together as a “double seal.” GIC can be used in combination with Cavit for the desirable “double seal” [7, 29]. Cavit can ideally be used with GIC as a “double seal” restorative material during the root canal procedure and following root canal completion before the permanent restoration [41].
Consequently, GICs may be considered the materials of choice for temporary restorations. The double sealing technique using Cavit followed by GIC has certain advantages. First, the outer layer of the GIC has anticariogenic properties owing to its fluoride release property. It is thermally compatible with enamel and, thus, biocompatible. It is esthetic and has low toxicity. Second, the inner layer of Cavit protects the root canal system from any moisture contamination (i.e., saliva).
One of the limitations of this study was that the data were collected using a questionnaire through Twitter and WhatsApp. Thus, those without these platforms were automatically excluded from the study. Moreover, the data were gathered using self-reported questionnaires by the participants and may not reflect the actual practice [42]. Thus, observational studies are recommended to assess actual practice. This would be achieved in future studies by observing the practitioners directly under the nose of the study examiner during their practice.
An ideal temporary restorative material is required owing to the frequent failure of the currently available temporary materials. Moreover, further clinical studies need to prove the results.
CONCLUSION
Within the limitation of the study, the cotton pellet was only used between visits and not after obturation. GIC was used most commonly by endodontists for both the anterior as well as posterior teeth. In addition, double sealing with Cavit and GIC was the most commonly used technique to restore the access cavity after obturation.
LIST OF ABBREVIATIONS
| GIC | = Glass Ionomer Cement |
| IRM | = Intermediate Restorative Material |
ETHICAL STATEMENT
This cross-sectional study was performed according to the World Medical Association, Declaration of Helsinki guidelines after approval from Majmaah University for Research Ethics Committee (MUREC) (HA-01-R-088).
CONSENT FOR PUBLICATION
Informed consent ensured voluntary participation; moreover, it also included information on the type of questions and expected time needed.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article.
ACKNOWLEDGMENTS
The author would like to thank the Deanship of Scientific Research at Majmaah University for supporting this work under Project Number No. R-2023-546 as well as Professor Saad Al-Nazhan and Dr.Riyadh Alroomy for their valuable comments on the article.

