All published articles of this journal are available on ScienceDirect.

The Attitude of Saudi Dentists Towards CAD/CAM in Restorative Dentistry
Authors Info & Affiliations
Abstract
Background:
The objective of this study was to investigate the attitude of Saudi dentists towards CAD/CAM (computer-aided design and computer-aided manufacturing) in restorative dentistry, investigate the existing knowledge and improve the practice accordingly.
Methods:
At random, electronic surveys were distributed to Saudi dental practitioners. The study received 500 questionnaires, with 425 being deemed valid. The following sections were included in the questionnaire: (i) Practitioner demographic information such as gender, practice level, and practice experience; (ii) CAD/CAM knowledge and benefits; (iii) CAD/CAM skills and training required; and (iv) CAD/CAM clinical overview. Descriptive statistics such as numbers and percentages were used to analyze the collected data. The Chi-square and Fisher's Exact tests were used to assess the results.
Results:
Males accounted for 292 (68.7%) of the participants, while females accounted for 133 (31.3%). General Practitioners accounted for the most subjects (253, or 59.5%), followed by consultants (91, or 21.4%) and specialists (81, or 19.1%). Among 425 dentists, 170 (40%) were aware of CAD/CAM, while 255 (60%) were not. Consultants and specialists demonstrated more significant levels of knowledge than general practitioners.
Furthermore, dentists with experience of more than ten years and experience of 5-10 years showed more understanding of CAD/CAM than dentists with less than five years of experience. Most participants (71.5%) do not use CAD/CAM in dental practice, whereas only less than one-third of them use it. Most participants (63.5%) plan to purchase CAD/CAM. Most dentists (74.4%) believe CAD/CAM technology is helpful in clinical procedures, while others believe it is useful in diagnostic and different functions. Most participants assume that CAD/CAM will eventually replace traditional methods. Most dentists assume that the use of CAD/CAM requires skills and training.
Conclusion:
The findings of this study show a prominent level of satisfaction and a favorable attitude among the surveyed dentists towards the usage of CAD/CAM technology in clinical practice.
1. INTRODUCTION
In dentistry, the usage and implementation of computer-aided design and manufacturing (CAD/CAM) technology have significantly increased during the last two decades [1]. Computer-aided design is abbreviated as CAD, and computer-aided manufacturing is abbreviated as CAM [2]. In dental technology, the phrase CAD/CAM is currently used as a synonym for restorations made by milling technology, which is not accurate [2]. Furthermore, the word CAD/ CAM does not specify any manufacturing technology [2]. CAD/CAM can be used efficiently to manufacture various restorative restorations such as inlays, onlays, veneers, crowns, and bridges [3].
CAD/CAM manufacturing of dental restorations can be divided into two primary ways: 1-Machining (Subtractive Manufacturing), often known as grinding or milling, is manufacturing an object by subtracting material from a block to achieve the required shape [4]. 2-Three-dimensional (3D) printing (Additive Manufacturing): this method creates an object by layering it one by one until it is fully completed [5]. Advanced CAD/CAM systems can be classified into three categories [6]: i) An in-office system in which a dentist digitally scans the prepped tooth, produces restorations chairside, and seats it all in one visit. ii) In-lab system allows laboratories to scan digital or physical models to construct restorations using CAD/CAM. iii) Centralized production: a dentist takes digital impressions in the chair and sends the data to the laboratory through the internet.
There are three parts to every CAD/CAM system: i) A scanner or digitalization tool that converts geometry into digital data that a computer can process ii) Data-processing software (CAD) that provides a data set for the product to be created, based on application, and iii) manufacturing technology (CAM) that converts the data set into the final products [2].
CAD/CAM technology has already established itself as an essential part of modern dentistry [7]. It has several advantages over traditional methods for dental restorations. Speed, quality, ease of use, chairside manufacturing of restorations in a shorter time, and a wider selection of materials are all advantages [2, 8]. It also enables more accessible and faster modification of the restoration form, shape, and shade to directly meet the patient's needs during the same mock-up visit. Additionally, the ceramic blocks have a transparent property that mimics enamel and are available in a wide variety of colours to provide a natural appearance [8]. Since CAD/CAM measurements and fabrication are so precise, the quality of restorations is incredibly high [9].
CAD/CAM systems are not free from drawbacks. The equipment and software are expensive initially, and the practitioner will need to invest time and money in training [8]. The disadvantages of CAD/CAM systems also include the cost of maintenance, fear of the unknown, a lack of willingness to learn a new concept, a refusal to change practice methods, a small number of users, and the size of the scanning device and the milling machine [10]. Additionally, due to software and manufacturing procedures, some applicability is limited [2].
Compared to traditional impression-making, most studies show that intra-oral scanning reduces chairside time, implying a more efficient clinical approach to CAD/CAM [11]. The overall accuracy of the CAD/CAM workflow is determined by two major correlated factors: the acquired image's accuracy and the definitive restoration's accuracy [11]. For partial scans and restorations, studies show that the digital workflow is as accurate as the traditional one [11]. Recent clinical studies have come up with contradictory results [11]. Regardless, both workflows are clinically acceptable in terms of accuracy [11]. The marginal and internal fit of single crowns (SCs) and Fixed Partial Denture (FPDs) produced using digital and traditional processes were compared in a systematic review [12]. While the included eleven research were mostly in-vitro, with just two clinical trials with a medium risk of bias, the study found that for SCs and FPDs, both digital and traditional procedures showed similar differences, with glass ceramics exhibiting the highest errors in both groups [12]. In the digital group, however, metal alloys had the fewest errors compared to glass ceramics and zirconia restorations [12]. The correctness of the final restoration was unaffected by whether the impressions were made with polyether or polyvinyl siloxane. The research findings back up those of a previous systematic review of twelve studies comparing the marginal fit of SCs made using digital and traditional methods [13]. There were no considerable differences in the marginal discrepancy of SCs across the methodologies with the reporting of the traditional and digital methods mean marginal fits of 59μm and 63μm, accordingly [13].
Operator difficulty perception and preference appear to be affected by clinical experience and operator rank [11]. A study composed of 30 experienced practitioners and 30 second-year dental students performed conventional and digital impressions of a single implant model; students indicated more severe difficulty with conventional impressions, whereas practitioners reported more incredible difficulty with intra-oral scanning [14]. This study also showed that 60% of students favoured digital scans against just 33% of experienced practitioners, indicating a significant difference in perception and choice between the two groups [14]. Furthermore, in one study, 50 dental students and 50 qualified practitioners were randomly assigned to either a conventional impression or a digital scan group to produce a bone-level implant impression/scan [15]. Intra-oral scanning was preferred by the majority of students (76%) and overqualified dentists (26%) [15].
In terms of current literature, few studies [16, 17] were published to determine dentists' attitudes and current practices regarding chair-side CAD/CAM technology in Riyadh city. Moreover, one published study [18] aimed to assess the knowledge of CAD/CAM among prosthodontic specialists. However, up to the authors' knowledge, no published research has been conducted to determine the CAD/CAM knowledge among Saudi dentists despite their classifications and city of practice. CAD/CAM usage in restorative dentistry has been a focus of attention of many researchers due to its importance in future practice. For this reason, it is crucial to conduct a study on CAD/CAM usage among dental practitioners in Saudi Arabia to investigate the current situation and fill the knowledge gap in this critical area to start further investigations. Additionally, that will help academicians determine the existing knowledge and improve the future outcomes regarding this crucial technology. Therefore, the current study aimed to investigate the attitude of Saudi dentists towards CAD/CAM in restorative dentistry, investigate the existing knowledge and improve the practice accordingly.
2. MATERIALS AND METHODS
A cross-sectional study was undertaken on Saudi dentists. The Ethical Committee of the University of Hail approved the study, which was carried out as per the principles of the Helsinki Declaration. The subject's privacy was fully respected. The study's estimated sample size was 400, according to the OpenEpi® sample size calculator, with a power of 84 percent and a P=5 percent. Dental practitioners are included in this study.
A total of 1000 Saudi Arabian practitioners were randomly selected and given a self-explanatory questionnaire as part of the study. Based on their observations and experiences, practitioners were given questionnaires to fill out. Participants gave their informed consent before any data were obtained.
The study received 500 questionnaires, with 425 deemed valid. All selected dental practitioners were emailed the survey and a cover letter emphasizing that all responses would be treated anonymously. Survey technology was used to notify non-responders four times at one-week intervals. Between July and September 2021, surveys were distributed.
A pilot survey of 20 dental practitioners was conducted using a self-administered structured questionnaire of 15 questions. At random, electronic surveys were distributed to Saudi dental practitioners. No changes to the questionnaire were required because of their feedback. The following sections were included in the questionnaire: (i) Practitioner demographic information such as gender, practice level, and practice experience; (ii) CAD/CAM knowledge and benefits; (iii) CAD/CAM skills and training required; and (iv) CAD/CAM clinical overview (Supplemental 1).
The significance of gender, practice level, and experience differences in the attitude toward CAD/CAM in restorative dentistry among Saudi dentists were determined using frequencies, crosstabs, Chi-Square, and Fisher's Exact tests. These submitted questionnaires were imported into Microsoft Excel and statistically analysed using the Social Sciences version 28 software (IBM SPS Statistics). Descriptive statistics such as numbers and percentages were used to analyse the collected data.
3. RESULTS
The questionnaire was filled out by 425 dentists in total. Males accounted for 292 (68.7%) of the participants, while females accounted for 133 (31.3%). General Practitioners accounted for the most subjects (253, or 59.5%), followed by consultants (91, or 21.4%) and specialists (81, or 19.1%).
Table 1 shows the distribution of questions and scores linked to CAD/CAM knowledge. Tables 2-4 show the impact of gender, experience, and practice level on CAD/CAM knowledge. Among 425 dentists, 170 (40%) were aware of CAD/CAM, while 255 (60%) were not. Table 2 shows significant variations in perceptions of CAD/CAM between men and women (p < 0.05). Moreover, as shown in Table 4, consultants and specialists demonstrated more significant levels of knowledge than general practitioners (p <0.01). Furthermore, dentists with experience of more than ten years and experience of 5-10 years showed more understanding of CAD/CAM than dentists with less than five years of experience, as shown in Table 3 (p <0.01).
Regarding the use of CAD/CAM in dental practice, most participants (71.5%) do not use it, whereas only less than one-third of them use it. The use of CAD/CAM in dental office show significant difference depending on gender, experience, and level of practice, as shown in Tables 2-4 (p < 0.01). Moreover, most participants (63.5%) plan to purchase CAD/CAM with the same mentioned factors difference (p < 0.05) as CAD/CAM in daily dental practice.
| Variable | - | Practice Level | P-value | ||
|---|---|---|---|---|---|
| GP | Specialist | Consultant | |||
| Tried CAD/CAM before | Yes | 65(25.7) | 43(53.1) | 62(68.1) | 0.000 |
| No | 188(74.3) | 38(46.9) | 29(31.9) | ||
| Use of CAD/CAM in Dental Office | Yes | 42(16.6) | 36(44.4) | 43(47.3) | 0.000 |
| No | 211(83.4) | 45(55.6) | 48(52.7) | ||
| Plan to purchase CAD/CAM | Yes | 163(64.4) | 48(59.3) | 59(64.8) | 0.049 |
| No | 90(35.6) | 33(40.7) | 32(35.2) | ||
| CAD/CAM useful in | Diagnostic | 65(25.7) | 6(7.4) | 6(6.6) | 0.000 |
| Clinical | 173(68.4) | 65(80.2) | 78(85.7) | ||
| Others | 15(5.9) | 10(12.3) | 7(7.7) | ||
| CAD/CAM can improve | Patient satisfaction | 4(1.6) | 0(0) | 1(1.1) | 0.018 |
| Quality of treatment | 5(2) | 2(2.5) | 1(1.1) | ||
| Time | 11(4.3) | 5(6.2) | 6(6.6) | ||
| Treatment efficiency | 2(0.8) | 2(2.5) | 0(0) | ||
| Accuracy | 4(1.6) | 1(1.2) | 2(2.2) | ||
| Predictably outcome | 3(1.2) | 1(1.2) | 1(1.1) | ||
| More than one answer | 224(88.5) | 70(86.4) | 80(87.9) | ||
| Prefer CAD/CAM in restorations production | Yes | 204(80.6) | 64(79) | 62(68.1) | 0.004 |
| No | 49(19.4) | 17(21) | 29(31.9) | ||
| Replace traditional | Yes | 187(73.9) | 58(71.6) | 57(62.6) | 0.008 |
| No | 66(26.1) | 23(28.4) | 34(37.4) | ||
| Improve quality compared to traditional restoration | yes | 233(92.1) | 68(84) | 69(75.8) | 0.000 |
| no | 20(7.9) | 13(16) | 22(24.2) | ||
| Save time | yes | 240(94.9) | 74(91.4) | 78(85.7) | 0.002 |
| No | 13(5.1) | 7(8.6) | 13(14.3) | ||
| More aesthetic | Yes | 195(77.1) | 43(53.1) | 43(47.3) | 0.000 |
| No | 58(22.9) | 38(46.9) | 48(52.7) | ||
| Require skills and training | Yes | 233(92.1) | 76(93.8) | 89(97.8) | 0.016 |
| No | 20(7.9) | 5(6.2) | 2(2.2) | ||
| Better production of temporary restorations | Milling | 50(19.8) | 22(27.2) | 23(25.3) | 0.004 |
| 3D Printing | 86(34) | 26(32.1) | 41(45.1) | ||
| Conventional | 33(13) | 9(11.1) | 13(14.3) | ||
| No idea | 84(33.2) | 24(29.6) | 14(15.4) | ||
| Variable | - | Response n (%) |
|---|---|---|
| Tried CAD/CAM before | Yes | 170(40) |
| No | 255(60) | |
| Use of CAD/CAM in Dental Office | Yes | 121(28.5) |
| No | 304(71.5) | |
| Plan to purchase CAD/CAM | Yes | 270(63.5) |
| No | 155(36.5) | |
| CAD/CAM useful in | Diagnostic | 77(18.1) |
| Clinical | 316(74.4) | |
| Others | 32(7.5) | |
| CAD/CAM can improve | Patient satisfaction | 5(1.2) |
| Quality of treatment | 8(1.9) | |
| Time | 22(5.2) | |
| Treatment efficiency | 4(0.9) | |
| Accuracy | 7(1.6) | |
| Outcome predictability | 5(1.2) | |
| More than one answer | 374(88) | |
| Prefer CAD/CAM in restorations production | Yes | 330(77.6) |
| No | 95(22.4) | |
| Replace traditional | Yes | 302(71.1) |
| No | 123(28.9) | |
| Improve quality compared to traditional restoration | Yes | 370(87.1) 987.1 0 |
| No | 55(12.9) | |
| Save time | Yes | 392(92.2) |
| No | 33(7.8) | |
| More aesthetic | Yes | 281(66.1) |
| No | 144(33.9) | |
| Require skills and training | Yes | 398(93.6) |
| No | 27(6.4) | |
| Better production of temporary restorations | Milling | 95(22.4) |
| 3D printing | 153(36) | |
| Conventional | 55(12.9) | |
| No idea | 122(28.7) |
| Variable | - | Dental Experience | P-value | ||
|---|---|---|---|---|---|
| <5 Years | 5-10 Years | >10 Years | |||
| Tried CAD/CAM before | Yes | 68(27.4) | 45(51.1) | 57(64) | 0.000 |
| No | 180(72.6) | 43(48.9) | 32(36) | ||
| Use of CAD/CAM in Dental Office | Yes | 47(19) | 35(39.8) | 39(43.8) | 0.000 |
| No | 201(81) | 53(60.2) | 50(56.2) | ||
| Plan to purchase CAD/CAM | Yes | 157(63.3) | 59(67) | 54(60.7) | 0.048 |
| No | 91(36.7) | 29(33) | 35(39.3) | ||
| CAD/CAM useful in | Diagnostic | 58(23.4) | 12(13.6) | 7(7.9) | 0.000 |
| Clinical | 175(70.6) | 68(77.3) | 73(82) | ||
| Other | 15(6) | 8(9.1) | 9(10.1) | ||
| CAD/CAM can improve | Patient satisfaction | 3(1.2) | 1(1.1) | 1(1.1) | 0.013 |
| Quality of treatment | 3(1.2) | 3(3.4) | 2(2.2) | ||
| Time | 11(4.4) | 5(5.7) | 6(6.7) | ||
| Treatment efficiency | 4(1.6) | 0(0) | 0(0) | ||
| Accuracy | 4(1.6) | 1(1.1) | 2(2.2) | ||
| Outcome predictability | 3(1.2) | 0(0) | 2(2.2) | ||
| More than one answer | 220(88.7) | 78(88.6) | 76(85.4) | ||
| Prefer CAD/CAM in restorations production | Yes | 201(81) | 67(76.1) | 62(69.7) | 0.005 |
| No | 47(19) | 21(23.9) | 27(30.3) | ||
| Replace traditional | Yes | 185(74.6) | 63(71.6) | 54(60.7) | 0.003 |
| No | 63(25.4) | 25(28.4) | 35(39.3) | ||
| Improve quality compared to traditional restoration | Yes | 230(92.7) | 71(80.7) | 69(77.5) | 0.000 |
| No | 18(7.3) | 17(9.3) | 20(22.5) | ||
| Save time | Yes | 234(94.4) | 78(88.6) | 80(89.9) | 0.023 |
| No | 14(5.6) | 10(11.4) | 9(10.1) | ||
| More aesthetic | Yes | 181(73) | 49(55.7) | 51(57.3) | 0.000 |
| No | 67(27) | 39(44.3) | 38(42.7) | ||
| Require skills and training | Yes | 226(91.1) | 85(96.6) | 87(97.8) | 0.004 |
| No | 22(8.9) | 3(3.4) | 2(2.2) | ||
| Better production of temporary restorations | Milling | 57(23) | 19(21.6) | 19(21.3) | 0.040 |
| 3D printing | 78(31.5) | 33(37.5) | 42(47.2) | ||
| Conventional | 29(11.7) | 14(15.9) | 12(13.5) | ||
| No idea | 84(33.9) | 22(25) | 16(18) | ||
| Variable | - | Practice Level | P-value | ||
|---|---|---|---|---|---|
| GP | Specialist | Consultant | |||
| Tried CAD/CAM before | Yes | 65(25.7) | 43(53.1) | 62(68.1) | 0.000 |
| No | 188(74.3) | 38(46.9) | 29(31.9) | ||
| Use of CAD/CAM in Dental Office | Yes | 42(16.6) | 36(44.4) | 43(47.3) | 0.000 |
| No | 211(83.4) | 45(55.6) | 48(52.7) | ||
| Plan to purchase CAD/CAM | Yes | 163(64.4) | 48(59.3) | 59(64.8) | 0.049 |
| No | 90(35.6) | 33(40.7) | 32(35.2) | ||
| CAD/CAM useful in | Diagnostic | 65(25.7) | 6(7.4) | 6(6.6) | 0.000 |
| Clinical | 173(68.4) | 65(80.2) | 78(85.7) | ||
| Others | 15(5.9) | 10(12.3) | 7(7.7) | ||
| CAD/CAM can improve | Patient satisfaction | 4(1.6) | 0(0) | 1(1.1) | 0.018 |
| Quality of treatment | 5(2) | 2(2.5) | 1(1.1) | ||
| Time | 11(4.3) | 5(6.2) | 6(6.6) | ||
| Treatment efficiency | 2(0.8) | 2(2.5) | 0(0) | ||
| Accuracy | 4(1.6) | 1(1.2) | 2(2.2) | ||
| Predictably outcome | 3(1.2) | 1(1.2) | 1(1.1) | ||
| More than one answer | 224(88.5) | 70(86.4) | 80(87.9) | ||
| Prefer CAD/CAM in restorations production | Yes | 204(80.6) | 64(79) | 62(68.1) | 0.004 |
| No | 49(19.4) | 17(21) | 29(31.9) | ||
| Replace traditional | Yes | 187(73.9) | 58(71.6) | 57(62.6) | 0.008 |
| No | 66(26.1) | 23(28.4) | 34(37.4) | ||
| Improve quality compared to traditional restoration | yes | 233(92.1) | 68(84) | 69(75.8) | 0.000 |
| no | 20(7.9) | 13(16) | 22(24.2) | ||
| Save time | yes | 240(94.9) | 74(91.4) | 78(85.7) | 0.002 |
| No | 13(5.1) | 7(8.6) | 13(14.3) | ||
| More aesthetic | Yes | 195(77.1) | 43(53.1) | 43(47.3) | 0.000 |
| No | 58(22.9) | 38(46.9) | 48(52.7) | ||
| Require skills and training | Yes | 233(92.1) | 76(93.8) | 89(97.8) | 0.016 |
| No | 20(7.9) | 5(6.2) | 2(2.2) | ||
| Better production of temporary restorations | Milling | 50(19.8) | 22(27.2) | 23(25.3) | 0.004 |
| 3D Printing | 86(34) | 26(32.1) | 41(45.1) | ||
| Conventional | 33(13) | 9(11.1) | 13(14.3) | ||
| No idea | 84(33.2) | 24(29.6) | 14(15.4) | ||
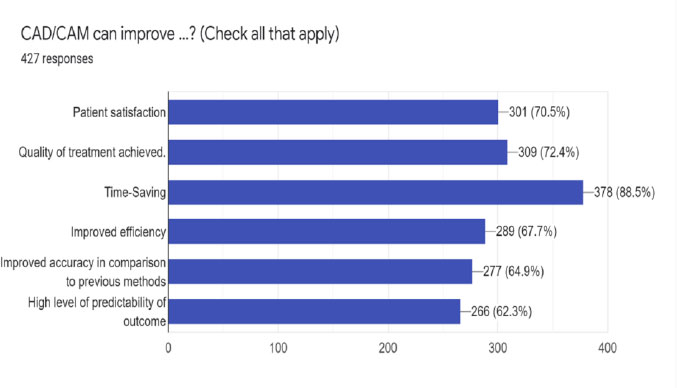
Most dentists (74.4%) believe CAD/CAM technology is helpful in clinical procedures, while others believe it is useful in diagnostic and different functions as shown in Fig. (1). The dentist experience and practice level show a significant difference in the use of CAD/CAM (p <0.01), whereas gender did not (p >0.05).
Most participants assume that CAD/CAM will eventually replace traditional methods. Furthermore, they feel that CAD/CAM will improve quality, save time, and be more aesthetically pleasing when compared to conventional methods. Again, there were statistically significant associations between the perception of CAD/CAM to replace traditional methods, improve quality, save time, and enhance aesthetics according to the experience and practice level of dentists (p <0.05). However, there is no significant association between gender and mentioned factors (p >0.05), except an association found with aesthetic aspects (p < 0.01).
Concerning using CAD/CAM in restorative procedures, most dentists prefer to use it with 77.6% compared to 22.4% who did not. Tables 2-4 illustrate the significant association between gender, experience, and level of practice for using CAD/CAM in restorative production (p <0.01).
Many dentists assume that the use of CAD/CAM requires skills and training. There are significant variations in the experience and practice level of dentists and their concern about training, whereas gender shows no variations, as shown in Tables 2-4.
Regarding which production methods would be better for temporary restorations, 3D printing accounted for the highest answer, followed by no idea by some dentists. The best way to produce temporary restorations shows statistically significant differences between gender, practice level, and experience of dentists (p <0.05).
4. DISCUSSION
Digital dentistry, which employs CAD/CAM technology, has grown in popularity during the last three decades. CAD/CAM systems have been available in dentistry for over 30 years but have lately become considerably more predictable as scanning, design, and milling technology have advanced [19, 20]. With its enhanced simplicity of use, CAD/CAM dentistry enables dentists to give high-quality aesthetic indirect restorations to patients in many situations in a single session, eliminate long-term temporization of prepared teeth, and improve operational dental readiness. The one treatment session idea is the most significant advantage of CAD/CAM in dentistry from a practical standpoint. Therefore, this could enable single-session tooth preparation, optical impression capture, virtual design, precise milling, customization, and restorative implantation [21].
Digital workflow removes many time-consuming and invasive clinical processes and traditional dental laboratory treatments that are technique-sensitive and labour demanding [22]. It had solved the drawbacks of conventional procedures, particularly quality, labour, and time [23]. Consequently, it benefits both the dentist and the patients. According to a 2016 survey conducted by Saponaro et al. on patient satisfaction with CAD/CAM-generated full dentures, 70% of experienced complete denture patients believed that their new digital complete dentures were “better” than their prior set of complete dentures [24].
In recent years, there has been a greater emphasis in Saudi Arabia on the value and significance of digital dentistry [25]. Dental practitioners in Saudi Arabia can see the increased promotion of CAD/CAM technology at the level of dental enterprises and continuing professional development courses. Furthermore, several dental institutions in Saudi Arabia advertise the availability of a CAD/CAM system at their facility to their consumers as a symbol of distinguished oral care services. Despite the importance of CAD/CAM technology in modern dentistry practice, little is known about dentists' current practices and views on this cutting-edge technology.
About 40% of the dentists stated that they tried CAD/CAM in their practice, and only 28.5% of the dentists had seen a CAD/ CAM unit. These findings are consistent with a previous survey of widely used dental materials for indirect restorations among active members of the Saudi Dental Society, which revealed that 29.8% of respondents utilize a CAD/CAM system in their clinical practice [26]. Furthermore, a recent Saudi Arabian study discovered that more than a quarter of the surveyed dentists (27.2%) reported the existence of a chairside CAD/CAM system in their current workplace [16]. An online survey of UK dentists on using CAD/CAM technology for patient treatment indicated that 56% of respondents did not utilize any CAD/CAM component [27].
The findings revealed that most dentists polled did not employ any digital technology. The expensive expense of CAD/CAM technology and the lack of recognized benefits over older methods were viewed as impediments to its use.
There were also concerns about the quality of dental restorations generated using chair-side CAD/CAM. Nonetheless, most participating dentists believed that CAD/CAM technology would play an essential role in the future and expressed a desire to incorporate this technology into their clinical practice [27]. In Switzerland, a study of Swiss Dental Association members indicated that a chair-side CAD/CAM system was installed in 23% of the offices examined [28]. According to one research conducted among USA Navy dental clinics and laboratories, by June 2017, more than a third of the given indirect restorations (38.1 percent) were created using CAD/CAM technology [29]. Furthermore, an examination of the data revealed a gradual increase in CAD/CAM manufactured restorations during the previous five years. Because of the numerous benefits, the authors predicted that digital dentistry would be more widely used by Navy dentists in the future [29]. Few surveys were conducted among dental students to ascertain their perspectives about incorporating digital dentistry, including CAD/CAM technology, into dental education and clinical practice.
Positive views were found, and a need for more exposure and incorporation of CAD/CAM technology into future dental training/education [30-32]. Because of the rising popularity of CAD/CAM technology in dental clinics and laboratories, the results of this survey show that the majority of dentists (93.6 percent) demand skills and training in CAD/CAM technology. Furthermore, this demonstrates a lack of practical understanding and clinical translation of information among undergrad students. Overall, undergraduates' knowledge of CAD/CAM has increased, but they still need to be educated on clinical applications to be prepared for the future of digital dentistry.
On the other hand, most dentists expressed a strong desire for a CAD/CAM system in the future (63.5%). This is consistent with the findings of the British survey, in which the majority of questioned dentists expressed an interest in using CAD/CAM technology in their future clinical practice [27].
The survey findings suggest that a significant proportion of responding dentists have some experience with CAD/CAM at the clinical practice level. It appears that CAD/CAM technology has invaded the workflow of Saudi dental clinics, with predictions of increased adoption across the more critical sector of dental practitioners in the future. On the level of satisfaction and attitude, the current survey results show widespread contentment and a favourable attitude among participating dentists about the usage and outcome of CAD/CAM in clinical practice. This surge in CAD/CAM and Ceramic/Resin restorations hints at a more significant trend in dentistry toward more aesthetically pleasing restorations and harnessing digital technology to improve dental practice.
The high quality of CAD/CAM digital restorations distinguishes them as safe alternatives to traditional dental treatment procedures. An increasing number of dentists are using CAD/CAM technology due to the efficiency of the digital workflow and the quality of the resulting restorations [13, 33, 34]. It should be mentioned that the majority of participants (71.1%) prefer the CAD/CAM approach on the traditional ways, and they value the benefits of the CAD/CAM system, which include time savings, increased income, and an increase in the number of patients in the clinic. In contrast to the sentiments of dentists in the UK study [27], the majority of dentists in this poll assessed the overall quality of dental restorations generated by a chair-side CAD/CAM system favourably. However, it appears that expert dentists are concerned about the overall quality of chair-side CAD/CAM restorations, which warrants additional examination. According to a UK survey, a significant number of dentists who utilize CAD/CAM technology in their clinical practice felt their training on this service was insufficient [27].
The current study has limitations because it is just cross-sectional. Additional longitudinal research is undoubtedly required to make more precise conclusions about the accuracy and clinical indications of CAD/CAM in prosthetic and implant dentistry and orthodontics. More randomized controlled trials on the use of CAD/CAM are required to provide an analysis that can rely on enough cases/patients treated adequately.
CONCLUSION
The findings of this study show a high level of satisfaction and a favourable attitude among the surveyed dentists towards the usage of CAD/CAM technology in clinical practice. It appears that CAD/CAM technology has invaded the workflow of Saudi dental clinics, with predictions of increased adoption across the more critical sector of dental practitioners in the future.
The high level of digitalization and the long successful history of CAD/CAM technologies may explain the increased usage in dental practice. However, in dental offices, the dentist's expertise may affect the availability of digital tools for patient care.
AUTHORS CONTRIBUTIONS
IKA and AAM contributed to the concept of the research, study design, statistical analysis, writing the original draft, and reading and editing the final paper. FAA and SMA contributed to data gathering and statistical analysis. The final manuscript was reviewed and approved by all writers.
ETHICS APPROVAL AND CONSENT PARTICIPATE
The Ethics Committee of Scientific Research, University of Hail, Saudi Arabia, approved the protocol of this study. All methods were performed in accordance with the declaration of Helsinki (Ethical number: H-2021-147).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Participants gave their informed consent before any data were obtained.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data that support the results of this study are accessible from the corresponding author [I.A-I] upon reasonable request.
FUNDING
Not applicable.
CONFLICT OF INTERESTS
The authors state that they have no conflicting interests.
ACKNOWLEDGEMENTS
Not applicable.
SUPPLEMENTARY MATERIALS
Supplementary material is available on the Publisher’s website.

