All published articles of this journal are available on ScienceDirect.

Evaluation of Variations in Root Canal Anatomy and Morphology of Permanent Maxillary Premolars among the Emirate Population using CBCT
Authors Info & Affiliations
Abstract
Background:
Many types of research have revealed that root canal anatomy differs by race and country based on various national populations, but no study has been conducted on the UAE population.
Objectives:
Identifying the most common morphology of the upper premolars in a group of local and non-local people in the UAE.
Methods:
Cone-beam computed tomography (CBCT) images of 215 intact maxillary premolars were analyzed. The Pearson Chi-squared test and the two samples t-test were applied.
Results:
Most of the maxillary first premolars were two-root formed (90%). Single-rooted teeth were less common (8%). Three-rooted maxillary first premolars represented a low frequency of 1.9%. Most of the maxillary second premolar teeth studied in this research (52%) had two roots. Almost all local and non-local populations had two canals for both first and second maxillary premolar. Only two maxillary first premolars (0.2%) had the three-canal morphology. The most frequent canal morphology in the maxillary first premolar group among local UAE and non-local was type V. The maxillary second premolar group among local UAE was type II (32%). In non-local UAE, type V (25%). In addition, six types of uncommon canal anatomic variants (types 1-2-3, 2-3-2, 3-2-1, 1-2-3-2, 2-1-2-1, and 3-2) were discovered in 3.7% of local UAE and 36.3% of non-local UAE.
Conclusion:
The results suggest a more quantitative approach to maxillary first and second premolar access cavity preparation in the UAE population to prevent errors and iatrogenic damage when identifying the canals.
1. INTRODUCTION
Endodontology addresses the dental pulp and periradicular area in healthy, diseased, injured situations and encompasses how it functions, prevention and treatment [1]. The two common reasons for endodontic treatment failure misunderstand tooth anatomy and technical competence [2]. As a result, a thorough knowledge of pulp canal anatomy is critical for successful root canal treatment (RCT) [3, 4]. Additionally, the dentist must be armed with the creative skills to read radiographic images and examine the dental pulp and periapical tissue to reach the correct diagnosis [5]. The initial stage in pulp canal therapy is to access the root canal system through the pulp chamber [6]. The tooth anatomy varies between populations, persons, and races [7-10]. Most of the variation is seen in maxillary first and second bicuspid teeth [11-13]. The anatomy of the premolar teeth is complex and is an enigma [3, 14, 15]. Even so, the maxillary bicuspid tooth has an oval-shaped canal. It typically has more than one canal, but the maxillary premolars generally have roots correlated with the number of root canals [3]. In most cases, premolar teeth have multiple roots and multiple canals.
Recent studies have made many modifications to classify root canal configuration systems [16]. The most common one is the Vertucci classifications. Vertucci has categorized root canal morphology into eight distinct [9, 17]. Some research findings in the literature are consistent with previous investigations by Vertucci et al. (2005) [18]. Other study findings contradict previous research by Vertucci et al. (2005) [18]. Unfortunately, many investigations utilizing various classification methods have shown significant differences in assessing the root canal anatomy of maxillary premolars across different cultures [13, 17, 19]. Utilizing the present technique during root canal treatment lowers the rate of root canal treatment failure. A periapical radiograph has traditionally been used to visualize the dentition into two Dimension (2D) images for root canal anatomy and treatment [20]. Recently, CBCT has made it possible to visualize the dentition and surrounding structures in the anatomical 3D space in 3D images [21]. CBCT is a basic image to demonstrate and assess root canal morphology for a given population [22]. This study further investigates the location of the canal orifices, dimensions of the pulp chamber and variations in the number of roots and canals for the upper first and second premolars due to their challenging morphology in clinical endodontics. The majority of research has found substantial differences in the root canal morphology of maxillary premolars among populations. However, there are no published studies with detailed data on the root canal anatomy of the maxillary first and second premolars in the UAE population. Thus, this research aimed to examine the root canal architecture of maxillary first and second premolars in the UAE population and compare the results to previous studies in other populations.
2. MATERIALS AND METHODS
2.1. Sample Collection
From January 2015 to December 2020, researchers from University Dental Hospital Sharjah (UDHS) performed a retrospective study. CBCT scans from patients who came to UDHS for different reasons were examined. CBCT scans of maxillary first and second premolars were examined for this research. The UDHS institutional review board granted ethical clearance (REC-20-03-03-01-S). The radiology archives of the hospital were used to acquire all of the scans. Sampling was performed at random, and the sample size was calculated using a previous study [23] with a confidence level of 95%. The sample size for maxillary first premolars was 88, while the sample size for maxillary second premolars was 98. We needed 107 maxillary first premolars and 108 maxillary second premolars to adjust for observational error.
CBCT images were obtained using the Sirona Galileos machine (Sirona Dental Systems, Bensheim, Germany). Three Dimension (3D) reconstruction was performed using Galaxix (Sirona Dental Systems, Bensheim, Germany). All exposures were performed with 85 kV/10 mA, 14 S. Exposure protocol: Volume II to reduce image noise and patient dose. The fixed Field of View (FOV) was 15 cm x 15 cm over the entire dentition with a voxel size of 0.075 mm. All images were collected according to the manufacturer’s instructions by an experienced radiologist (SWA). On a 17-inch display, cross-sectional pictures were collected and reconstructed in the axial, coronal, and sagittal planes.
2.2. Inclusion Criteria
The inclusion criteria were as follows: evaluation of maxillary bicuspids of males and females in the UAE aged 12-70 years who provided informed consent. For non-local (South Asian) samples were selected from (Pakistan, India, Bangladesh, Srilanka, Afghanistan, Bhutan, Nepal and Maldives); Patients were included in the current study if they required CBCT examination for treatment planning or dental diagnosis at UDHS, had fully developed roots, were not treated endodontically, and had no resorbed roots or calcified canals. The study excluded teeth with significant crown and root caries lesions, substantial metal restorations, fractures, orthodontic wires, veneers, immature root tips, and endodontic treatment. Pictures with low image quality were also excluded.
2.3. Radiographic Evaluation
Two experienced endodontists performed all data measurements. Each investigator assessed the CBCT pictures twice and computed the average value with a two-week delay between assessments. When agreement could not be achieved, endodontists and radiologist’s assisted in decision-making. The following observational data were recorded during the examination of the teeth: (1) facial-lingual width of pulp chamber landmarks and morphologic measurements related to furcation, (2) number and configuration of roots, (3) number of root canals and canal configuration based on Vertucci’s classification.
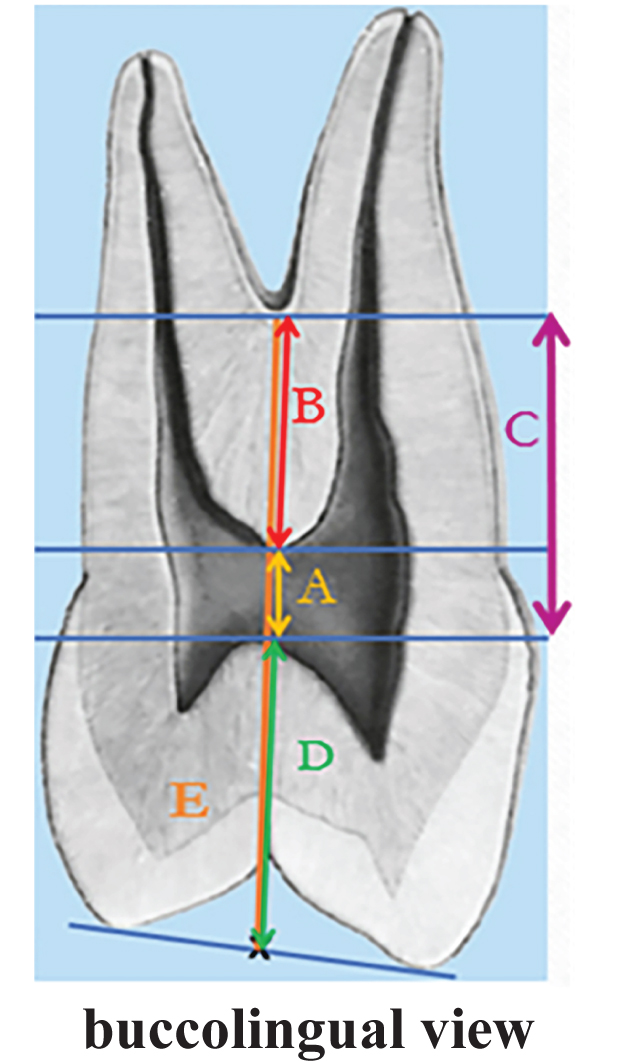
Teeth were radiographed in buccal and palatal views to allow direct morphological measurements related to furcation and to show cusp tips and furcation in one radiograph [24]. To reduce the possibility of perforating the furcation, the dentist should know where they are. Therefore, the most coronal landmark was selected for measurement [24-26]. A horizontal line was drawn parallel to each landmark, and six measurements were taken in millimetres (mm) from these landmark lines. First, consider the midpoint of a line that connects the two cusps points. The five measures were denoted by A, B, C, D, and E. In detail, A is the space between the apical point on the pulp chamber roof and the coronal point on the pulp chamber floor. B is the distance between the coronal point at the pulp chamber’s floor and the coronal at the root furcation. C is the distance obtained by adding A and B, i.e., the space between the apical point on the pulp chamber ceiling and the coronal position on the root furcation. D is the space between the midpoint of a line connecting the two cusp points and the apical point on the pulp chamber’s ceiling. E is the space between the midpoints of two cusp tips and the coronal point to the root furcation itself (Fig. 1).
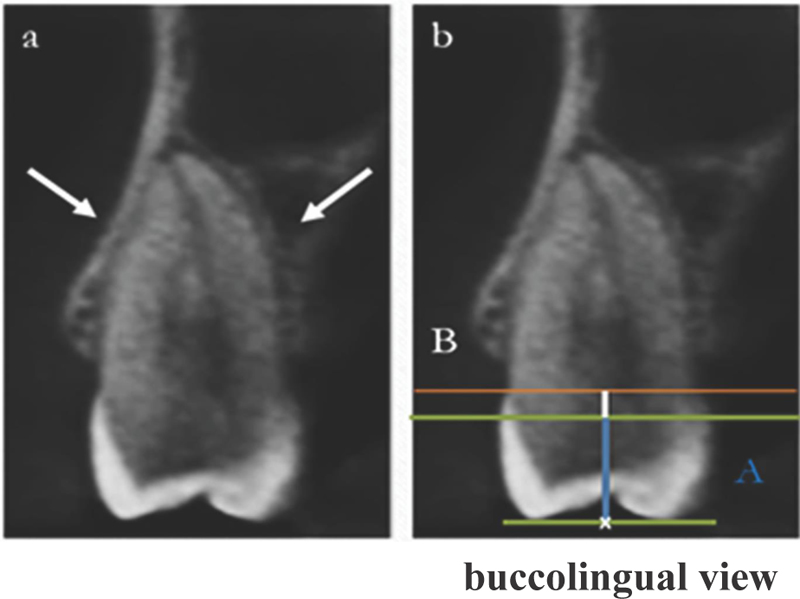
While measurements for single-rooted maxillary premolars are obtained from the lines of these landmarks, in detail, A is the space between the midpoint of a line connecting the two cusp points and the apical point on the pulp chamber’s ceiling. B is the space between the pulp chamber’s apical point at the Cementoenamel junction (CEJ) level to the furcation itself (Fig. 2).
According to Krasner and Rankow (2004), the dental pulp chamber’s mesiodistal width in an axial view of CBCT scans was measured in an area showing the centricity of the pulp chamber at the CEJ along the horizontal plane running from mesial to distal of the pulp chamber for each upper premolar [27].
2.4. Statistical Analysis
Analysis was performed using SPSS, version 26 (IBM, Armonk, NY, USA). Means and standard deviations (SD) were reported for numerical variables. Frequencies with percentages were reported for categorical variables. Pearson’s Chi-squared test was used to examine the association between categorical variables. Independent-sample t-tests were used to compare the means of different numerical variables. Statistical significance was set at p < 0.05.
3. RESULTS
A total of 107 bilateral Maxillary first permanent premolars (MFPPs) with 108 bilateral Maxillary second permanent premolars (MSPPs) were examined. Table 1 shows 52% male cases and 51% cases from a local ethnic group. Table 2 shows the maxillary 1st and 2nd premolar roots distribution by gender and ethnicity. The majority of the maxillary first premolars (90%) had two roots; this was observed in 92% of females, 88% of males, 83% of locals, and 96% of non-locals. Similarly, most of the maxillary second (52%) premolars were two rooted in 47% of females, 56% of males, 38% of locals, and 67% of non-locals. There were only 2 cases of three roots among local males. The prevalence of one root in the maxillary second premolar was significantly higher among locals (63%) than non-locals (33%). The prevalence of two roots in second bicuspids was higher among non-locals (67%) than locals (37%), both p = 0.002.
Table 3 shows no significant differences in the number of roots distributed according to tooth position (left/right for first and second premolars, p > 0.05).
Table 1.
| Bilateral Maxillary First Permanent Premolar, N=107 | Bilateral Maxillary Second Prmanent Premolar, N=108 | |
| Gender | ||
| Male | 57 (48.3) | 61 (51.7) |
| Female | 50 (51.5) | 47 (48.5) |
| Ethnicity | ||
| Local | 54 (49.1) | 56 (50.9) |
| Non-Local | 53 (50.5) | 52 (49.5) |
Table 2.
| One Root | Two Roots | Three Roots | P-Value | |
| First Premolars | ||||
| Male | 5 (8.8) | 50 (87.7) | 2 (3.5) | 0.401 |
| Female | 4 (8) | 46 (92) | 0 | |
| Total | 9 (8.4) | 96 (89.7) | 2 (1.9) | |
| Second Premolars | ||||
| Male | 27 (44.3) | 34 (55.7) | 0 | 0.357 |
| Female | 25 (53.2) | 22 (46.8) | 0 | |
| Total | 52 (48.1) | 56 (51.9) | 0 | |
| First Premolars | ||||
| Local | 7 (13) | 45 (83.3) | 2 (3.7) | 0.076 |
| Non-Local | 2 (3.8) | 51 (96.2) | 0 | |
| Total | 9 (8.4) | 96 (89.7) | 2 (1.9) | |
| Second Premolars | ||||
| Local | 35 (62.5) | 21 (37.5) | 0 | 0.002 |
| Non-Local | 17 (32.7) | 35 (67.3) | 0 | |
| Total | 52 (48.1) | 56 (51.9) | 0 | |
| Tooth Position | One Root | Two Roots | Three Roots | P-Value |
| N (%) | N (%) | N (%) | ||
| First premolars | ||||
| Right | 4 (7.5) | 48 (90.6) | 1 (1.9) | 0.95 |
| Left | 5 (9.3) | 48 (88.9) | 1 (1.9) | |
| Total | 9 (5.3) | 96 (89.7) | 2 (1.9) | |
| Second premolars | ||||
| Right | 25 (47.2) | 28 (52.8) | 0 | 0.842 |
| Left | 27 (49.1) | 28 (50.9) | 0 | |
| Total | 52 (48.1) | 56 (51.9) | 0 | |
54 maxillary first premolars and 56 maxillary second premolars in the local UAE population and 53 maxillary first premolars and 52 maxillary second premolars in the non-local UAE population were analyzed for the number of roots, root canals, and type of canal configurations. The results are presented in Tables 4 & 5.
Table 4 shows that one root in a maxillary first premolar was detected in 17% of local UAE subjects and 11% of non-local UAE subjects. Two roots in maxillary first premolar were present in 68% of local UAE and 59% of non-local UAE (p < 0.0001). Three roots were only found in 2 teeth in the first premolar. Almost all local and non-local groups had two canals for the first and second maxillary premolars.
A single root was found in the maxillary second premolar in 83% of local UAE subjects and 90% of non-local UAE subjects. Two roots in maxillary second premolars were found in 32% of local UAE subjects and 41% of non-local UAE subjects (Table 4).
Table 5 shows the distribution of different canal morphologies in maxillary premolars.
The dominant canal morphology in the maxillary second premolar group among local UAE subjects was type II (32%), followed by type III (27%) and type V (20%).
Based on the Vertucci classification, the most common canal morphology in the maxillary first premolar group among non-local UAE subjects was type V (59%), followed by type IV (9%) and type VI (8%). An additional type, 7 (13.2%), was also identified and unrelated to the Vertucci classification.
The most common canal morphology in the maxillary first premolar group among local UAE was type V (52%), followed by type IV (26%) and type II (6%). An additional type, 2 (3.7%), was also identified and is not related to the Vertucci classification.
In the maxillary second premolar group among non-local UAE subjects, the dominant canal morphology was type V (25%), followed by type III (15.4%) and type VII (13.5%). Based on the Vertucci classification, an additional type, 12 (23.1%), was also identified and not related to the Vertucci classification.
Table 6 compares various morphological measurements recorded from single-rooted maxillary premolar CBCTs. There was a statistically significant difference in the distance from the facial to the lingual pulp chamber in the single-rooted maxillary premolar CBCTs between the local UAE (1.26 ± 0.27 mm) and South Asian population (1.10 ± 0.32 mm, p = 0.037).
There was no statistically significant difference in the distance from the midpoint of a line connecting the two cusp tips to the apical point on the roof of the pulp chamber in single-rooted maxillary premolar CBCTs for the local UAE population (5.58 ± 0.72 mm) and South Asian population (5.31 ± 1.08 mm, p = 0.252).
There was a significant difference between the distance from the apical point on the pulp chamber roof to the CEJ in the single-rooted maxillary premolar CBCT for local UAE subjects (1.36 ± 0.75 mm) and South Asian subjects (1 ± 0.27 mm, p = 0.049).
Table 7 compares various morphological measurements recorded from multiple rooted maxillary premolars in CBCTs. There were statistically significant differences in all measurements in multiple rooted maxillary premolar CBCT between the local UAE and South Asian populations (p-value <0.05).
| - | Local UAE | Non-local UAE (South Asian) | ||||
| - | Maxillary First Premolar (n=54) | Maxillary Second Premolar (n=56) | P value | Maxillary First Premolar (n=53) | Maxillary Second Premolar (n=52) | P Value |
| Number of Roots | ||||||
| One | 7 (16.7) | 35 (83.3) | < 0.0001 | 2 (10.5) | 17 (89.5) | < 0.0001 |
| Two | 45 (68.2) | 21 (31.8) | 51 (59.3) | 35 (40.7) | ||
| Three | 2 (100) | 0 | 0 | 0 | ||
| Number of canals | ||||||
| One | 0 | 1 (100) | 0.218 | 0 | 0 | 1 |
| Two | 52 (48.6) | 55 (51.4) | 53 (50.5) | 52 (49.5) | ||
| Three | 2 (100) | 0 | 0 | 0 | ||
| Local UAE | Non-local UAE (South Asian) | |||
| Canal Morphology | Maxillary First Premolar | Maxillary Second Premolar | Maxillary First Premolar | Maxillary Second Premolar |
| Type I | 1 (1.9) | 1 (1.8) | 1 (1.9) | 0 |
| Type II | 3 (5.6) | 18 (32.1) | 1 (1.9) | 4 (7.7) |
| Type III | 3 (5.6) | 15 (26.8) | 0 | 8 (15.4) |
| Type IV | 14 (25.9) | 6 (10.7) | 5 (9.4) | 3 (5.8) |
| Type V | 28 (51.9) | 11 (19.6) | 31 (58.5) | 13 (25) |
| Type VI | 2 (3.7) | 4 (7.1) | 4 (7.5) | 5 (9.6) |
| Type VII | 1 (1.9) | 1 (1.8) | 4 (7.5) | 7 (13.5) |
| Others | 2 (3.7) | 0 | 7 (13.2) | 12 (23.1) |
| Total | 54(100) | 56 (100) | 53 (100) | 52 (100) |
| Distances | Single Rooted Maxillary Premolars | Single Rooted Maxillary Premolars | Mean Difference | T Statistic | P-Value |
| (mm) | CBCT for local UAE, mean (SD) | CBCT for non-local, mean (SD) | |||
| Distance from mesial to distal of the pulp chamber | 1.26 (0.27) | 1.10 (0.32) | 0.17 | 2.14 | 0.037 |
| Distance from the middle of a line connecting the two cusp tips to the apical point on the pulp chamber roof. | 5.58 (0.72) | 5.31 (1.08) | 0.27 | 1.16 | 0.252 |
| Distance from the apical point on the roof of the pulp chamber to the CEJ. | 1.36 (0.75) | 1 (0.27) | 0.36 | 2.01 | 0.049 |
| Distances | Multiple Rooted Mxillary Premolars | Multiple Rooted Maxillary Premolars | Mean Difference | T Statistic | P-Value |
| (mm) | CBCT for local UAE (mean ± SD) | CBCT for South Asian (mean ± SD) | |||
| Distance from mesial to distal of the pulp chamber | 1.21 (0.27) | 1.06 (0.25) | 0.16 | 3.66 | < 0.0001 |
| Distance from the apical point on the pulp chamber roof to the coronal point on the pulp chamber floor. | 2.57 (0.88) | 2.24 (0.78) | 0.33 | 2.47 | 0.015 |
| Distance from coronal point on floor of the pulp chamber to the coronal point on the root furcation. | 2 (0.74) | 1.31 (0.49) | 0.45 | 7.14 | < 0.0001 |
| Distance from the apical point on the pulp chamber roof to the coronal point on the root furcation. | 4.57 (1.05) | 3.55 (1.01) | 1.02 | 6.11 | < 0.0001 |
| Distance from the midpoint of a line connecting the two cusp tips to the apical point on the pulp chamber roof. | 6.11 (0.99) | 5.75 (0.90) | 0.35 | 2.34 | 0.02 |
| Distance from the midpoint of a line connecting the two cusp tips to the coronal point on the root furcation. | 10.83 (1.33) | 9.77 (1.24) | 1.06 | 5.09 | < 0.0001 |
4. DISCUSSION
Endodontic procedures are typically challenging procedures in daily dental practice. Therefore, an understanding and determination of root canal anatomy are required for a successful RCT. Many variations were seen in anatomical structures in maxillary first and second bicuspid teeth [11].
The majority of the problems encountered while treating the root canal in maxillary premolars due to variations in the architecture of the root canal systems; thus, maxillary premolars were selected for the current research.
This study is the first study to investigate the root and canal morphologies of maxillary first and second premolar simultaneously in a UAE population using a pattern of CBCT images. We hoped that our research would assist in improving effective root canal treatment in the UAE and contribute to the literature on root canal morphology and symmetry of permanent teeth in the South Asian population.
The bulk of previous anatomic investigations discovered that the most common type of maxillary first premolars is the two-rooted form, and the incidence of three-rooted forms is rare [7, 17, 22, 28-37]. The current study verifies this.
In the current study, 90% of the maxillary first premolars had two roots, indicating that the two-root shape was the most common root anatomy in a UAE population (Table 2). This rate was similar to Neelakantan et al. (2011), who discovered that 86% of the teeth in a mostly Indian population had two roots [29]. In comparison, the result was significantly higher than in Saudi Arabia in 2008 (80.9%) [30], Brazil (80.2%) [31], Saudi Arabia 2013 (71.7%) [32], Kosovo (70.14%) [33], Turkey (70.8%) [34], Jordan [35] and Pakistan [36] (68.6%), Germany [37] and Israel [22] (62%), Saudi Arabia 2019 [17] and Turkey 1998 (61%) [7] populations. Single-rooted teeth were less common (8%), ranging from 11.7% to 37.3% [17, 22, 29-37]. Three-rooted maxillary first premolars were found in just two of teeth, representing a low frequency of 1.9% (Table 2). Three-rooted maxillary first premolars are uncommon in general [8]. Despite the modest number of three-rooted first premolars, clinicians must not ignore the third root and its internal canal.
According to Ingle et al. (2019), most anatomic investigations have shown that the most common type of maxillary second premolar is the single-rooted form, with the frequency of three-rooted forms ranging from 0% to 1% [28]. Two-rooted maxillary second premolars ranged from 1.6% to 20.4% [28].
When compared to work by Ingle et al. (2019) [28], research by others shows that the maxillary second premolar has a greater incidence of two rooted maxillary second premolars among the Jordan (about 44.2%) [18], the Turkey [7] and Saudi Arabia [38] (30%), the Brazil (28%) [31], and Saudi Arabia populations (23.6%) [32].
Most of the teeth studied in this research (52%) had two roots, whereas the remaining teeth (48%) had a single root. The proportion of two-rooted teeth was greater than in prior research reported by other groups [7, 18, 31, 32, 38]. These differences emphasize the impact of ethnic background, evaluation techniques, and sample sizes on root morphology studies in maxillary premolars.
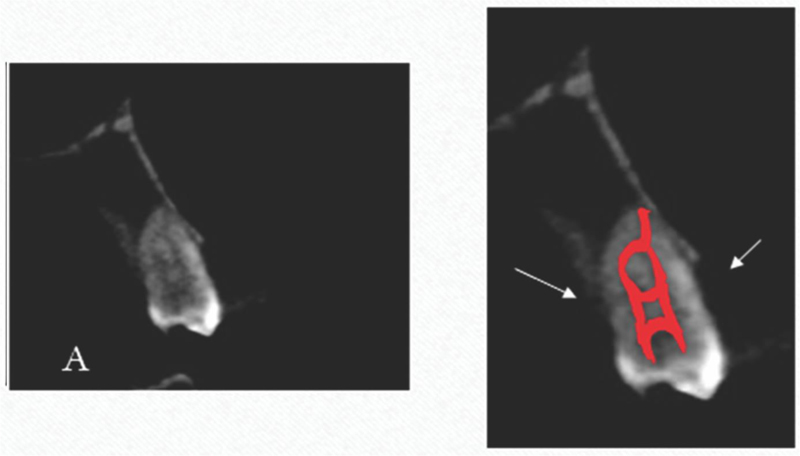
Root canal configurations vary from tooth to tooth and from population to population. In our study, almost all local and non-local populations had two canals in the first and second maxillary premolars (Table 4). This share lies within the range mentioned in research on the usage of CBCT or clearing techniques [7, 8, 19, 23, 29, 36, 38-40]. Only two maxillary first premolars (0.2%) had the three-canal morphology close to the previously described range of 0.4% to 3.3% [4, 7, 23, 35, 41, 42]. Vertucci (1984) found that the maxillary first premolar was the only tooth with all eight kinds of canal morphology [9]. The current investigation confirmed that root canal networks have a wide range of structural diversity. In addition, six types of uncommon canal anatomic variants (types 1-2-3, 2-3-2, 3-2-1, 1-2-3-2, 2-1-2-1, and 3-2) were discovered in both maxillary first and second premolars. According to Sert and Bayirli’s classification of canal configurations [43], type 2-1-2-1 was designated as type Nineteen (XIX) (Fig. 3), type 3-2 as type XV, type 1-2-3-2 as type X, type 2-3-2, type 1-2-3 (Fig. 4) and type 3-2-1 as a new type.
Several published investigations have identified multiple canals in maxillary bicuspids, similar to this research. Yi-Han Li et al., Elnour et al., and Jayasimha et al. reported type XIX canal configurations [14, 23, 38]. Elnour et al, and Senan et al, reported type 1-2-3, type 3-2-1, type 2-3-2 and type 3-2 canal configurations [19, 38]. The study’s most interesting findings were the new root canal types discovered in 3.7% of local UAE subjects and 36.3% non-local UAE subjects. These canal types account for a sizable proportion of the total. As a result, it is necessary to assume that therapy will be difficult. Type V (52%) was the most common canal configuration in maxillary first premolars among local UAE subjects, whereas type II (32%) was the most common canal configuration in second premolars. Moreover, type V (59%) was the most common canal configuration in maxillary first premolars among non-local UAE residents, and type V (25%) was the most common canal configuration in second premolars. This finding is consistent with previous findings [3, 14, 29, 37, 38, 44, 45].
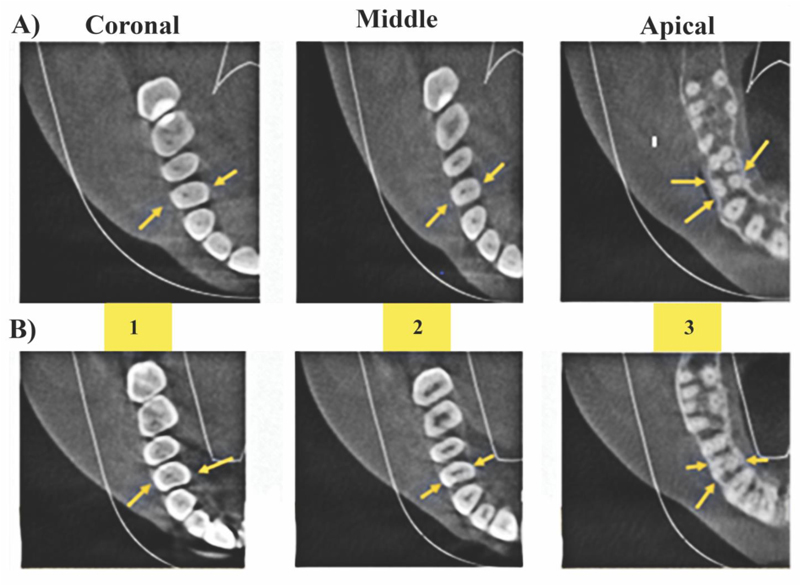
A) Axial view of CBCT scans for local maxillary first premolar. Yellow arrows point to the examined teeth showing 1 2 3 canal configurations type at different root levels.
B) Axial view of CBCT scans for non-local maxillary first premolar. Yellow arrows point to the examined teeth showing 1 2 3 canal configurations type at different root levels.
Understanding pulp chamber morphological measurements are important for proper access for successful endodontic treatment and avoiding errors such as perforation while locating the canals.
The anatomical landmark associated with the maxillary furcated bicuspids pulp chamber was measured for the first time in the Deutsch et al. (2005) study [24]. Then, in 2007, Venkateshbabu et al. observed that the morphological measurement of maxillary first premolars in the Indian population was equivalent to a previous study [25]. However, these furcated bicuspid teeth were significantly longer in the Nagpur population. In maxillary first premolars, the author observed that the CEJ corresponds to the ceiling of the pulp chamber, which is identical to the pulp chamber discovered by Deutsch et al. (2005) [26].
The distance between the midpoint of a line connecting the two cusp points and the furcation, according to Deutsch and Musikant (2005), is 11.55 mm [24]. The height of the pulp chamber is 2.76 mm, and the average distance between the midpoint of a line joining the two cusp suggestions and the roof of the pulp chamber is 6.94 mm. The authors found that the CEJ was constantly near the pulp chamber ceiling of the top furcated bicuspids.
The distance between the midpoint of a line connecting the two cusp points and the closest point to the furcation was 10.83 ± 1.33 mm in the local UAE population and 9.77 ± 1.24 mm in the non-local UAE population in our research. For maxillary second premolars, the average distance between the midpoint of a line connecting the two cusps and the ceiling of the pulp chamber was 6.11 ± 0.99 mm for local UAE subjects and 5.75 ± 0.90 mm for non-local UAE subjects. For maxillary first premolars, the mean distance between the midpoint of a line connecting the two cusps and the ceiling of the pulp chamber was 5.58 ± 0.72 mm for the local UAE population and 5.31 ± 1.08 mm for the non-local UAE population. The height of the pulp chamber was 2.57 ± 0.88 mm for local UAE subjects and 2.24 mm ± 0.78 mm for non-local UAE subjects.
Clinically, approximately 4.7 mm is available to perforate after reaching the pulp chamber’s roof (at the level of the CEJ). The addition of this distance to the 6.1 mm distance between the cusp tip and the pulp chamber ceiling for bicuspids yields 10.8 mm, approximately 11 mm. A drill should be marked at 11 mm, so the dentist understands where it is in the furcation to decrease the possibility of perforation in the furcation. These results were similar to those of Deutsch’s study [24].
As each year of life progressed, the size of the pulp chamber decreased due to calcification. Therefore, these measurements differed in ways that were either directly or indirectly related to the height of the pulp chamber.
CONCLUSION
Our study is the first to analyze the most common morphology of the upper premolars in a group of Emirati subpopulations. The results in the current study serve as a guide that can offer a more quantitative approach to maxillary first and second premolars to access cavity preparation in the UAE population to prevent errors and iatrogenic damage when identifying the canals; CBCT measurements can be advantageous for more precise access preparations.
In a nutshell, the following results were drawn from the research:
(1) Distribution of maxillary first and second premolar roots by gender and ethnicity reveals that most maxillary first premolars (90%) had two roots, with 92% of females, 88% of males, 83% locals, and 96% non-locals. Similarly, most maxillary second premolars (52%) were two roots, with 47% females, 56% males, 38% locals, and 67% non-locals. Only two instances of three roots were found among local men.
(2) No significant variations were seen in the distribution of roots based on tooth location (left/right for first and second premolars).
(354 maxillary first premolars and 56 maxillary second premolars from the UAE were examined, and the number of roots, root canals, and canal configurations were assessed. Results indicate that one root was discovered in 17% of the first premolar and 83% of the second premolar, and two roots were found in 68% of the first premolar and 32% of the second premolar. Three roots were discovered in just two teeth of the first premolar. Almost all local and non-local groups had two canals for the first and second maxillary premolars.
(4) Prevalence of different canal shapes in maxillary premolars: According to Vertucci categorization, the most frequent canal morphology in the maxillary first premolar group among local UAE residents was type V (52%), followed by type IV (26%), and type II (2%). The general canal morphology in the maxillary second premolar group among local UAE residents was type II (32%), followed by type III (27%) and type V (3%).
(5) Comparison of different morphological parameters obtained from CBCT of single-rooted maxillary premolars reveals the following results: distance from facial to lingual of the pulp chamber and measurement between single-rooted maxillary premolars CBCT for local UAE 1.26 mm (SD 0.27) and South Asian1.10 mm (SD 0.32) was statistically significant. There is a statistically significant difference in measurement of the distance from the apical point on the pulp chamber ceiling to the CEJ and measurement between single-rooted maxillary premolars CBCT for local UAE 1.36 mm (SD 0.75) and South Asian1mm (SD 0.27).
(6) Different morphological parameters obtained in CBCT from multiple rooted maxillary premolars showed statistically significant differences between multiple rooted maxillary CBCT for the UAE and South Asia.
LIST OF ABBREVIATIONS
| UAE | = United Arab Emirates |
| CBCT | = Cone Beam Computed Tomography |
| 2D | = Two Dimension |
| 3D | = Three Dimension |
| SD | = Standard Deviations |
| SPSS | = Statistical Package for the Social Sciences |
| RCT | = Root canal treatment |
| CEJ | = Cementoenamel Junction |
| MFPP | = Maxillary First Permanent Premolar |
| MSPP | = Maxillary Second Permanent Premolar |
| FOV | = Field of View |
| UDHS | = University Dental Hospital Sharjah |
| Nineteen | = XIX |
| mm | = millimetre |
AUTHORS’ CONTRIBUTIONS
H.A, Conceptualization, Methodology, Investigation, Data curation, Writing Original Draft; MG, Supervision, Investigation, Reviewing and Editing; SA, Methodology, Investigation, Reviewing and Editing; SWA, Supervision, Methodology, Data curation; IM, Supervision, Methodology, Data curation, Formal Analysis, Reviewing and Editing. The authors read and approved the final manuscript
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Local Research Ethics Committee approved this study without restrictions under the protocol number: REC-20-03-03-01-S. Through this approval, the research team had the required administrative permissions to access the data used in this research.
HUMANS AND ANIMAL RIGHTS
No animals were used for studies that are base of this research. All human procedures were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
For this type of retrospective study, and as recommended by the Research and Ethics Committee, formal consent is not required.
STANDARDS OF REPORTING
STROBE guidelines has been followed.
AVAILABILITY OF DATA AND MATERIALS
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
FUNDING
This study received no study from profit or not-for-profit organizations.
CONFLICT OF INTEREST
The authors declare no conflict of interest financial or otherwise.
ACKNOWLEDGEMENTS
The authors are grateful to the study participants.

