All published articles of this journal are available on ScienceDirect.

Perception and Utilization of Artificial Intelligence (AI) among Dental Professionals in Saudi Arabia
Abstract
Objective:
Artificial intelligence (AI) is the new buzzword that is trendy in multiple branches of dentistry. The aim of this study was to assess perceptions and utilization of AI among dental professionals in Saudi Arabia.
Methods:
This was a cross-sectional study investigating 389 dental students and dentists from 22 cities in Saudi Arabia using a validated self-reported questionnaire.
Results:
A total of 49.4% of participants reported knowing what AI is; 44.5% reported having basic knowledge of AI principles, and 42.2% know of AI uses in dentistry. The most common AI information source was social media (66.07%). Out of 17 AI attitude items, 16 were scored above the midpoint. A total of 75.0% of participants agreed or strongly agreed AI will lead to major advances in dentistry. In contrast, 49.1% agreed or strongly agreed that AI could replace dentists in the future. There were no significant differences by gender or region, but students and interns had significantly higher attitude scores than did dentists. There was a widespread desire to take professional courses in dental AI use (69.7%), and some had used dental AI applications (25.4%) or taken an AI course (18.5%–20.3%). The most common barriers to dental AI use were non-availability of courses (73%) and lack of time (68.9%).
Conclusion:
Dental professionals in Saudi Arabia have moderate awareness levels and high rates of good attitudes about AI in dentistry. However, AI use in practice is limited. Incorporating AI in dental curricula is crucial due to the worldwide digital transformation.
1. INTRODUCTION
Artificial intelligence (AI) is the trendy new buzzword in science today, and many advancements use AI for technological improvements [1]. For instance, AI is anticipated to help create excellence in health care services [2]. AI can be defined as the utilization of computer systems to perform steps that up to now have required human intelligence, including things such as making decisions, problem-solving, speech recognition, visual perception, and language translation and understanding [3].
There are many daily uses of AI through large companies, such as Google’s search engine intelligence and smart device personal assistants [4]. The deep learning and machine learning of these applications are used in different aspects of health information systems [5, 6]. As an example, AI is used for making decisions in medical specialties that involve large amounts of data, such as pathology and radiography [7].
Deep learning, one of the models used for AI, is described as a collection of software methods that allow for finding latent information when investigating high volumes of data [8]. Deep learning has many clinical applications in health care [9] and has been used when a diagnosis is based on an image, such as radiographic assessment of bone maturity (age) [10, 11] or when diagnosing hip osteoarthritis [12], prostate cancer [13], lung cancer [14], or colorectal polyps [15]. Deep learning and AI has also been extensively used in oral care, for example, in caries diagnosis [16], cystic lesion identification [17], dental color selection [18], temporomandibular disorder diagnoses [19], identification of oral cancer [20], orthognathic treatment [21], periapical lesions [22], cephalometric analysis [23], removable partial denture design [24], root morphology [25], and periodontal diseases [26].
This heavy involvement with AI has made medical students feel threatened that AI will replace them [27]; however, this feeling was less prevalent among students in specialties where there is less AI involved [28]. Conversely, AI is seen by some as opening new horizons into better opportunities by creating more advancements [29].
Studies of AI use among dental professionals are rare due to it being a new and emerging field. A single study conducted on a national scale in Turkey found that less than half (48.40%) of dental students had basic knowledge about AI, while the majority (85.70%) agreed that AI will induce major changes in dental care [4]. Additionally, 28.60% believed that AI might replace them in the future [4]. Another study in Saudi Arabia indicated that dental students and dentists had favorable attitudes and awareness of AI and robotics in dentistry [30]. However, the study combined AI and robotics into one concept, which made it difficult to clearly investigate AI topics. Given the scarcity of this topic in the Saudi literature, the aim of this study was to assess AI perceptions and utilization among dental professionals in Saudi Arabia.
2. MATERIALS AND METHODS
The current study used a cross-sectional design with a self-reported questionnaire to assess perceptions and usages of AI among dental professionals in Saudi Arabia. Study participants were recruited using a convenience sampling technique. The invitations were sent as a Google form questionnaire distributed on different social media platforms, including Twitter, Facebook, WhatsApp, Instagram, and Telegram. They were sent to student groups at different Saudi universities, hospitals, and dental clinics. The inclusion criteria were that participants must be dental students or dentists who were currently studying or working in Saudi Arabia. Any respondent who did not sign the study’s informed consent notification was excluded from the study. The informed consent included information about all of the study details, and it was mandatory to agree to it before any questions could be answered. Data gathering was conducted from November 2021 to December 2021. The sample size calculation used an expected rate of 50% (to maximize the sample size), with an alpha level of 5% and a power of 90%, resulting in 271 participants required for this study.
The items on the study questionnaire were derived from previous studies [4, 31], with modifications. The questionnaire was composed of 47 questions distributed in four sections. Section one gathered demographic data about gender, age, qualifications, city of residence, university/hospital affiliation, region of residence, nationality, and whether the participant knew what AI is. Section two started with a definition of AI (including instructions not to change their previous answer), and then participants were asked about the basics of AI, uses of AI in dentistry, and five potential sources of AI information. Section three included 17 attitude statements about AI assessed using a Likert scale with answers ranging from 1 (strongly disagree) to 5 (strongly agree). Section four included four questions about current experiences with AI in dentistry. Section five assessed nine different potential reasons for not learning about AI. The answer options for sections two, four, and five were dichotomous (Yes/No). The questionnaire was validated for understanding, logic, flow, syntax, and grammar by a pilot of nine dental practitioners before the final version was created. It took an average of 10 minutes to complete the questionnaire.
The collected data were tabulated and analyzed using Microsoft Excel software and SPPS version 27 (IBM Corp., Armonk, NY, USA). The descriptive analysis included the mean (m), standard deviation (SD), frequency, and percentages. The inferential tests included a t-test and ANOVA. A p-value of 0.05 was set as the level of significance. The questionnaires had nothing that could identify participants, in order to protect their privacy. All data were accessed by the main author only, and data were stored in a protected computer at Umm Al-Qura University (UQU). Ethical approval was given by the research ethics committee at Umm Al-Qura University with the number HAPO-02-K-012-2021-11-827.
3. RESULTS
In this study, a data set of responses from 389 dental students and dentists were analyzed. Participants had a mean age of 26.19 years, with an SD of 4.85. The participants were from 22 cities in Saudi Arabia: Abha, Albaha, Alhasa, Alhofuf, Dammam, Duba, Haql, Jeddah, Khamis Mushait, Kharj, Khaybar, Khober, Madinah, Makkah, Najran, Qurayat, Riyadh, Safwa, Sakaka, Tabuk, Taif, and Yanbu. Participants’ gender, qualification, region, and nationality are provided in Table 1.
| Variable | - |
Number of Participants |
Percentage of Participants |
|---|---|---|---|
| Gender | Male | 111 | 28.50% |
| Female | 278 | 71.50% | |
| Qualification | Dental student | 167 | 42.90% |
| Dental intern | 63 | 16.20% | |
| Graduated dentist | 124 | 31.90% | |
| Dental specialist | 27 | 6.90% | |
| Dental consultant | 8 | 2.10% | |
| Region | Western | 257 | 66.10% |
| Central | 26 | 6.70% | |
| Eastern | 40 | 10.30% | |
| Southern | 39 | 10.00% | |
| Northern | 27 | 6.90% | |
| Nationality | Saudi | 367 | 94.30% |
| Non-Saudi | 22 | 5.70% |
In regard to AI knowledge, 49.40% of respondents reported knowing about AI, 29% were not sure, and 21.6% had none. In addition, 44.5% reported having basic knowledge about the working principle of AI, and 42.2% reported being aware of the uses of AI in dentistry. Participants reported different sources of information about AI, and those results are shown in Table 2.
Participants’ attitudes about AI were measured with 17 statements, as shown in Table 3. A t-test revealed no significant differences between males and females on any of the 17 items except for “AI can replace dentists/physicians in the future,” where males (m = 3.47, SD = 1.29) agreed with the statement at significantly higher rates (t = 2.475(387), p = 0.012) than females (m = 3.1, SD = 1.35). A t-test also showed that on most of the items, dental students and interns had higher scores than dentists, as shown in Table 3. ANOVA revealed no significant differences for any of the 17 items based on different regions.
| Source of AI information | No. | Percentage |
|---|---|---|
| Social media (Twitter, Instagram, etc.) | 257 | 66.07% |
| Lectures at the university, conferences, continuing education | 150 | 38.56% |
| Family or friends | 134 | 34.45% |
| TV | 125 | 32.13% |
| Newspapers or magazines | 100 | 25.71% |
| I have not gotten any information about AI from any source | 35 | 0.9% |
| Statement |
Strongly Disagree N (%) |
Disagree N (%) |
Neutral N (%) |
Agree N (%) |
Strongly Agree N (%) |
Overall Mean (SD) |
Dental Student or Intern mean (SD) |
Dentist Mean (SD) |
p-value |
|---|---|---|---|---|---|---|---|---|---|
| I think AI will lead to major advances in dentistry and medicine. | 12 (3.1%) |
12 (3.1%) |
70 (18%) | 99 (25.4%) | 196 (50.4%) | 4.17 (1.03) | 4.24 (0.99) | 4.07 (1.07) | 0.115 |
| AI applications in dentistry are aligned with Saudi Arabia’s Vision 2030. | 10 (2.6%) |
12 (3.1%) |
76 (19.5%) |
125 (32.1%) |
166 (42.7%) |
4.09 (0.99) |
4.18 (0.93) |
3.97 (1.05) |
0.044 |
| Learning AI will open up better job opportunities for dentists. | 11 (2.8%) |
15 (3.9%) |
73 (18.8%) |
122 (31.4%) |
168 (43.2%) |
4.08 (1.01) |
4.19 (0.93) |
3.93 (1.11) |
0.017 |
| AI applications should be part of postgraduate dental training. | 11 (2.8%) |
19 (4.9%) |
75 (19.3%) |
124 (31.9%) |
160 (41.1%) |
4.04 (1.03) |
4.11 (1) |
3.93 (1.06) |
0.096 |
| AI can be used in 3-dimensional implant positioning and planning. | 8 (2.1%) |
20 (5.1%) |
81 (20.8%) |
124 (31.9%) |
156 (40.1%) |
4.03 (1) |
4.15 (0.89) |
3.86 (1.12) |
0.006 |
| AI can be used for radiographic diagnosis of tooth caries. | 12 (3.1%) |
19 (4.9%) |
83 (21.3%) |
135 (34.7%) |
140 (36%) |
3.96 (1.02) |
4.07 (0.92) |
3.79 (1.14) |
0.009 |
| AI can be used as a quality control tool to assess the success of treatments. | 10 (2.6%) |
21 (5.4%) |
91 (23.4%) |
134 (34.4%) |
133 (34.2%) |
3.92 (1.01) |
4.01 (0.94) |
3.80 (1.1) |
0.050 |
| AI can be used in the radiographic diagnosis of pathologies in the jaw. | 13 (3.3%) |
18 (4.6%) |
86 (22.1%) |
146 (37.5%) |
126 (32.4%) |
3.91 (1.01) |
4.00 (0.96) |
3.77 (1.08) |
0.031 |
| AI applications should be part of undergraduate dental training. | 16 (4.1%) |
22 (5.7%) |
87 (22.4%) |
124 (31.9%) |
140 (36%) |
3.90 (1.08) |
4.01 (1.01) |
3.74 (1.17) |
0.020 |
| AI can be used in the radiographic diagnosis of periodontal diseases. | 13 (3.3%) |
18 (4.6%) |
92 (23.7%) |
137 (35.2%) |
129 (33.2%) |
3.90 (1.02) |
4.00 (0.95) |
3.75 (1.11) |
0.022 |
| I find the use of AI in dentistry and medicine exciting. | 18 (4.6%) |
20 (5.1%) |
92 (23.7%) |
120 (30.8%) |
139 (35.7%) |
3.88 (1.1) |
3.97 (1.06) |
3.74 (1.14) |
0.043 |
| AI can be used in forensic dentistry. | 14 (3.6%) |
18 (4.6%) |
100 (25.7%) |
128 (32.9%) |
129 (33.2%) |
3.87 (1.04) |
4.02 (0.94) |
3.66 (1.14) |
0.001 |
| AI can be used for the diagnosis of soft tissue lesions in the mouth. | 20 (5.1%) |
20 (5.1%) |
93 (23.9%) |
130 (33.4%) |
126 (32.4%) |
3.83 (1.1) |
3.92 (1.07) |
3.69 (1.12) |
0.044 |
| AI can be used as a treatment planning tool in dentistry. | 20 (5.1%) |
24 (6.2%) |
81 (20.8%) |
144 (37%) |
120 (30.8%) |
3.82 (1.09) |
3.96 (1.02) |
3.63 (1.17) |
0.005 |
| AI can be used as a prognostic tool to predict the course of a disease and determine whether there is a chance of recovery. | 12 (3.1%) |
19 (4.9%) |
110 (28.3%) |
138 (35.5%) |
110 (28.3%) |
3.81 (1) |
3.94 (0.91) |
3.62 (1.1) |
0.002 |
| AI can be used as a definitive diagnostic tool in the diagnosis of diseases. | 31 (8%) |
23 (5.9%) |
103 (26.5%) |
123 (31.6%) |
109 (28%) |
3.66 (1.18) |
3.73 (1.15) |
3.55 (1.22) |
0.127 |
| AI could replace dentists/physicians in the future. | 65 (16.7%) |
53 (13.6%) |
80 (20.6%) |
117 (30.1%) |
74 (19%) |
3.21 (1.35) |
3.26 (1.35) |
3.14 (1.35) |
0.423 |
| Question | No. | Percentage |
|---|---|---|
| Do you want to take a professional course about AI related to dentistry? | 271 | 69.70% |
| Have you ever used any AI software or application in dentistry? | 99 | 25.40% |
| Have you taken any professional courses about AI related to dentistry? | 79 | 20.30% |
| Have you taken any professional courses about AI in general? | 72 | 18.50% |
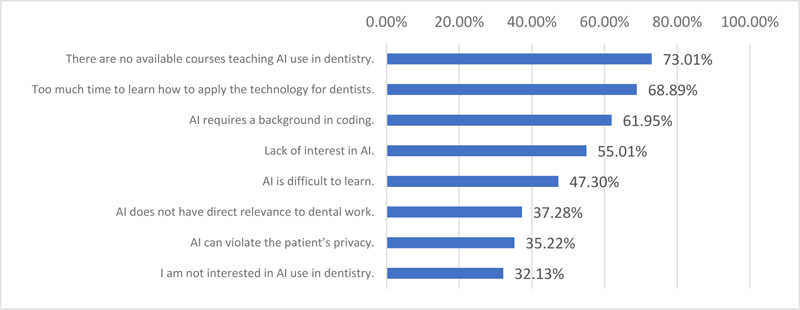
Participants’ answers regarding practicing AI are shown in Table 4. Participants also reported different barriers to using AI in dentistry, and those results are provided in Fig. (1).
4. DISCUSSION
The aim of this study was to assess perceptions and uses of AI among dental professionals in Saudi Arabia. Almost half of the participants reported knowing what AI means, and around half of them also reported having basic knowledge about AI principles and AI usage in dentistry. The most frequently reported source of information about AI was social media, followed by university lectures, conferences, and continuing education. Almost all AI attitude items had scores above the midpoint. In general, there were no significant differences in terms of gender or region, but dental students and interns had significantly higher attitude scores about AI in dentistry than dentists. Despite the widespread desire to take professional courses in AI related to dentistry, few respondents had used AI software or applications in dentistry or taken a course about AI. The most common barriers to using AI in dentistry were the lack of courses that teach the topic and the lack of time.
A total of 49.4% of the participants reported that they knew what AI is, while 44.5% also reported that they had basic knowledge about AI principles, and 42.2% answered that they knew of AI uses in dentistry. Our results were lower than previous studies conducted in central India (68%) [32] and North India (55.8%–77.4%) [33]. Nevertheless, our result is to some extent similar to a Turkish study that stated that 48.4% of their respondents had basic knowledge about AI and 78.9% had previously heard about AI [4]. More interestingly, a previous Saudi study stated that 90.7% had heard about robotics and AI in dentistry, but only 7% could differentiate between robotics and AI [30]. We argue that the prevalence of awareness in that prior study was inflated by the study’s design combining AI and robotics [30]. In addition, the previous study included different nationalities because participants were recruited at an international conference. Therefore, we claim that our result is more valid with regard to the level of awareness about AI in dentistry in Saudi Arabia. One of the reasons that the Indian studies had higher rates of respondents having knowledge and awareness of AI in dentistry might be the revolutionary and industrial activities and services in information technology in India. Nevertheless, the prevalence of AI is rising in the field of dentistry, and this variation in rates of knowledge and awareness may be due to the differences in educational curricula across countries and institutes.
The most frequently reported source of AI information in our study was social media (66.07%), which is similar to the Turkish study [4] that indicated social media was the most common (76.1%) source of information. This directs our attention to the significant role social media plays as a source of information about new technologies and advancements, filling the role previously held by magazines, newspapers, and even continuing education and lectures. This indicates that social media can be used more systematically to boost awareness and knowledge about AI in dentistry, especially given that some studies in Saudi Arabia have highlighted the role of social media as a learning approach for dental students [34, 35]. In fact, it has been reported that dental students spend a great amount of time on a daily basis using social media as a learning tool [36].
The results of our study show that dental students and dentists have positive attitudes about using AI in dentistry. This is similar to all the previous studies conducted in Kenya [37], Central India [32], Turkey [4], and Saudi Arabia [30]. Our study also showed that gender had no relationship with most of the attitude items, as was reported in a previous study [4]. In fact, our study and prior studies all showed that dental professionals are motivated to learn about AI and its uses in dentistry. For example, in the present study, 67.9% and 72% of the participants agreed or strongly agreed, respectively, that AI should be incorporated in dental training for postgraduate and undergraduates. These numbers are similar to a Turkish study that reported that 74.60% and 79.80% thought AI should be included in postgraduate and undergraduate curricula, respectively [4]. Furthermore, in the present study, 69.70% wanted to take professional courses in AI related to dentistry. This high percentage is not as high as the 93% that was previously reported in a Saudi Arabian study. The difference might be due to the previous study combining AI and robotics, but this nonetheless reveals a general affinity for learning about AI in dentistry among dental professionals in Saudi Arabia. It should be noted that AI is a new topic, and it might therefore be challenging to introduce it in a convenient way. This can be attributed to the complexity of the technical system and the variety of applications and operational methods of AI [38]. Additionally, our data revealed several challenges to learning about AI, including a lack of AI courses, lack of time, and the need to learn coding as part of the educational process, all of which have been reported in the literature [4]. Nevertheless, digital literacy will become a necessity with the world’s advancement and global technological movement. This is augmented by Saudi Arabia’s Vision 2030, which includes a digital transformation for the country as one of its main initiatives.
Despite the high rates of desire to take professional courses in AI for dentistry (69.7%), few of this study’s respondents had used software or applications related to AI in dentistry (25.4%) or had taken a course about AI (18.5%–20.3%). This highlight also that awareness might not be enough, and there may be an overestimation of the level of dental professional awareness about AI. Thus, it might be useful for courses and topics discussing AI to be provided in a more hands-on session to make AI and its uses more familiar for dental professionals.
In the present study, 49.1% of respondents agreed or strongly agreed that AI could replace dentists and physicians in the future. This had been reported as a major concern in previous studies in Kenya (64.2%) [37], Turkey (28.6%) [4], and Saudi Arabia (40.3%) [30]. This point has been discussed in the literature, with the conclusion that it would be difficult to completely replace medical practitioners with AI systems for several reasons, including patient–medical practitioner engaging discussions, trust, reassurance, empathy [39], and ethical issues related to data accessibility and privacy [40]. However, it has also been mentioned that medical practitioners could be replaced by those who are able to use AI and have advanced technological abilities [41]. This highlights the importance of introducing AI and its uses in dentistry as an important topic in dental education, not as a luxury but as a future necessity.
This study might be one of the few studies that has focused on AI awareness and attitudes in Saudi Arabia and which included participants from multiple cities. However, the questionnaire was self-reported, and the results cannot be generalized because the data might not be pertinent to all dental students and dentists in Saudi Arabia. Future studies might include more detailed questions about AI from a technical point of view, which could provide more insight into the true levels of knowledge about AI in dentistry.
CONCLUSION
There is a moderate level of awareness about AI in dentistry among dental professionals in Saudi Arabia, but there is a high level of positive attitudes toward the use of AI in the dental field. Nevertheless, there is a need for AI to receive more attention in dental education by including the topic in undergraduate, postgraduate, and even continuing education curricula in order to align with the expected digital advancements in the dental arena.
LIST OF ABBREVIATIONS
| AI | = Artificial Intelligence |
| SD | = Standard Deviation |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethical approval was given by the research ethics committee at Umm Al-Qura University with the number HAPO-02-K-012-2021-11-827.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All research steps involving humans were conducted in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975.
CONSENT FOR PUBLICATION
All participants in this study acknowledged their informed consent before participating.
STANDARDS OF REPORTING
STROBE guidelines have been followed.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available from the author and can be available upon reasonable request.
FUNDING
This study was self-funded.
CONFLICT OF INTEREST
The author declares no conflicts of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

