All published articles of this journal are available on ScienceDirect.

Non-surgical Treatment of a Late Adolescent Patient with Skeletal Class II Malocclusion Using Clear Aligners: A Case Report
Abstract
Background/Introduction:
There are a variety of treatment modalities for orthodontic treatment of patients with skeletal Class II malocclusions in late adolescence. These treatment modalities may include surgical intervention, camouflage treatment, functional appliances, extraction of teeth, and/or Class II elastics mechanics. Most Class II mechanics produce retroclination of the upper incisors and proclination of lower incisors. These dentoalveolar effects limit the possibility for forward mandibular projection/growth, hence minimizing skeletal improvement.
Case Presentation:
To present a unique case report that was treated with a new perspective in maximizing skeletal improvement in a late adolescent male with skeletal Class II malocclusion and deep overbite.
A 15-year-old male presented with a skeletal Class II pattern due to mandibular retrognathism was treated with non-extraction, non-surgical technique using clear aligners in two phases. Phase 1 was designed to decompensate the compensated inclination of his anterior teeth, and phase II was planned to correct his skeletal and dental Class II malocclusion/mal relation. Results: Maxillary incisors decompensation of the inclination of the upper and lower incisors and posterior teeth intrusion allowed forward mandibular projection that led to skeletal and dental correction of his malocclusion and improvement of his chin forward projection.
Conclusion:
This case report shows successful treatment of a Class II malocclusion in alate adolescent male. This method could perhaps be used for similar cases, avoiding the need to extract teeth or include surgical intervention.
1. INTRODUCTION
Class II malocclusions in teenage patients are commonly seen in daily orthodontic practice. Many patients in this age group now prefer clear aligners over braces [1]. Most orthodontic practitioners are very familiar with clear aligners, however, correcting the Class II buccal relationship and increased overbite may still be an area where many clinicians would hesitate to offer clear aligners. It can be challenging to treat patients with a skeletal Class II occlusal relationship that are beyond the age in which functional appliances are recommended. There are a variety of different mechanics and adjuncts that can be used to assist with the Class II correction. These mechanical adjuncts include fixed Class II correctors, temporary anchorage devices, extractions, etc [2]. Many case reports have shown that Invisalign clear aligners can improve Class II malocclusions either by upper arch distalization or premolar extraction [3-7]. However, a recent systematic review on the effectiveness of Invisalign clear aligners reported that clear aligners may produce clinically acceptable outcomes that could be comparable to fixed appliance therapy for the buccolingual inclination of the upper and lower incisors in mild to moderate malocclusions. However, not all potential clinical scenarios have been assessed in the included studies [8]. A recent systematic review suggested that retroclination of upper incisors occurs in all groups treated with fixed Class II correctors; however, there is a conflicting report on their effects on minimizing the proclination of lower incisors [9]. The intrusion of the posterior teeth to allow forward autorotation of the mandible using Invisalign clear aligners has been recently reported [10, 11]. This case report aims to evaluate if upper anterior teeth proclination with posterior intrusion using clear aligners can improve skeletal and dental Class II malocclusion with deep overbite in a late adolescent male. This case study shows an example of a patient treated with clear aligners in non-conventional, new methods to facilitate the Class II and overbite correction. The rationale of this new concept is to maximize skeletal Class II improvement by decompensating anterior teeth and intruding posterior teeth to allow Class II malocclusion correction by maximum possible mandibular forward projection.
2. CASE REPORT
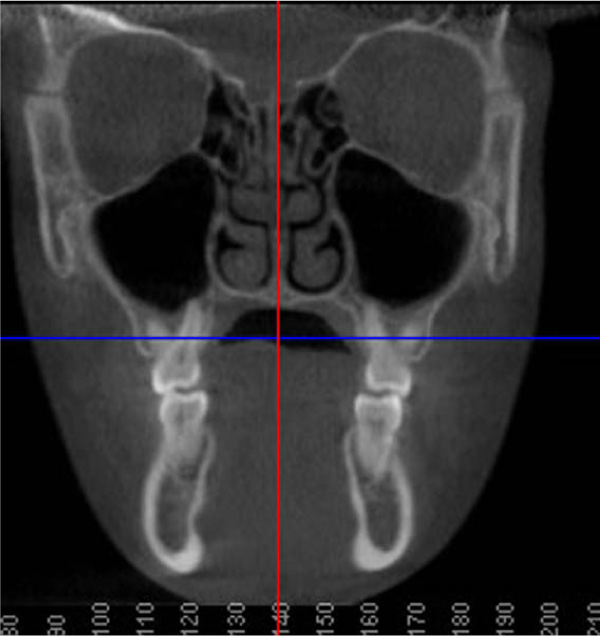
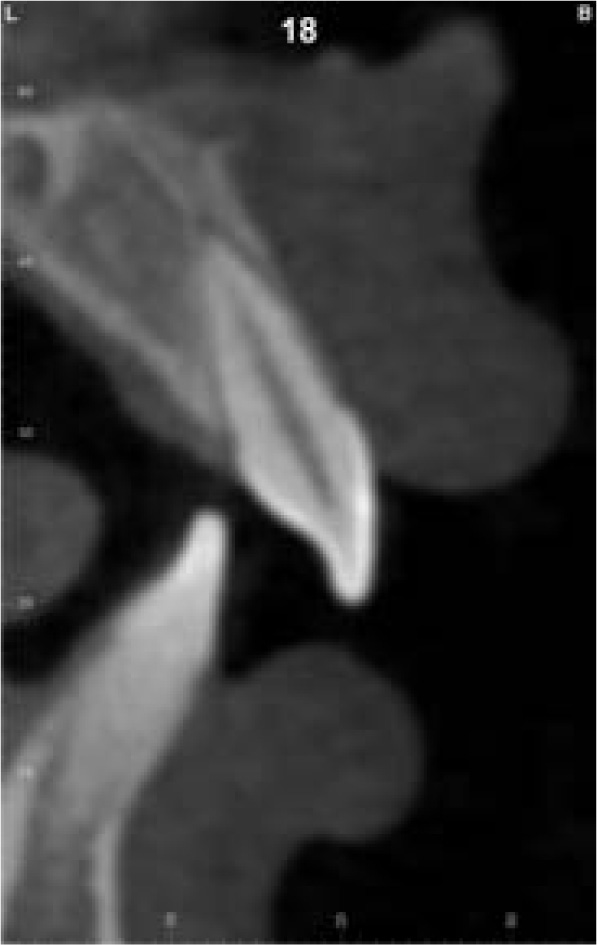
A fourteen-year and five-month-old male patient presented with a chief complaint of crowded teeth, deep overbite, and recessive chin. No medical or general health concerns were reported. His initial clinical records showed that he had a Class II malocclusion of skeletal and dental etiology. His molar relationship was full cusp Class II on both right and left sides. Overbite was measured at 80% and overjet was measured at 6mm. Cephalometric analysis revealed that he had a skeletal Class II apical base relationship with a retrognathic mandible (ANB= 9.4 degrees. Wits appraisal =5.9 mm) and forward growth direction (Y-axis = 60.9 degrees, FMA =22.2 degrees). In addition, his initial tomographic evaluation revealed a forward growth trend of the mandible as indicated by the direction of the mandibular condyle [12]. His cervical vertebral maturation (CVM) was estimated to be at stage 5/V [13-15]. His upper incisors were retroclined (UI-SN= 89 degrees) and retruded (U1-NA =0.5 mm). His lower incisors were proclined and protruded (IMPA =103 degrees and L1-NB =8.5 mm). The patient had narrow upper and lower arches and low tongue posture (Figs. 1 and 2a, Table 1).
The skeletal treatment objectives were to improve the retrognathic mandible and chin projection. The dental treatment objectives were to level and align the upper and lower arches, correct the Class II occlusal relationship, level the curve of Spee, improve the increased overbite, and improve the upper and lower incisor positions and inclinations. The soft tissue treatment objective was to improve the convex soft tissue profile.



Discussion of various treatment possibilities was completed in a case presentation with the patient and his parent. The patient and parent were provided with the options of fixed orthodontic appliance treatment in combination with orthognathic surgery (mandibular advancement), fixed orthodontic appliance treatment in combination with a fixed Class II corrector, or clear aligner treatment with elastics. The differences between these options were described, and the patient and his parent explained that they were not interested in any type of surgical treatment option. The patient showed that his preference would be the clear aligner therapy.
2.1. Intervention
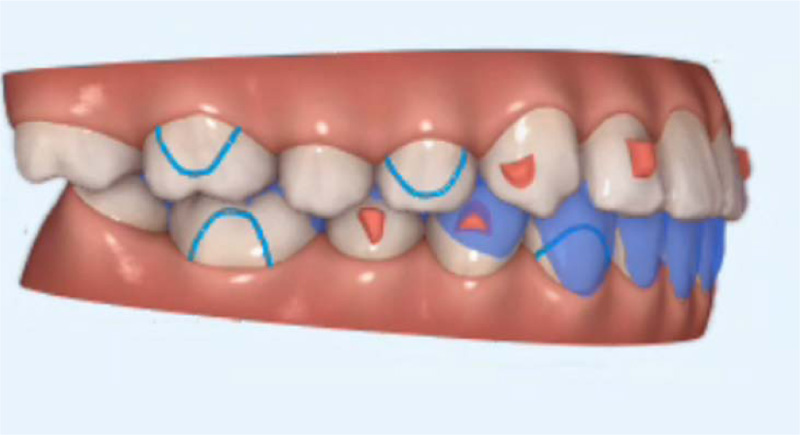
The initial digital treatment plan ClinCheck® (Align Technology, Inc. San Jose, California, USA) included decompensation of his upper and lower incisors by proclination of the upper incisors using power ridges. Intrusion of the upper molars and premolars was prescribed to allow a vertical bite jump and forward autorotation of the mandible. The lower arch began with the intrusion of the lower incisors, followed by intrusion of the lower molars and premolars to allow for a vertical bite jump. Precision cuts for both Class II and Class III elastics were included in the aligners. This initial digital treatment plan provided 50 active aligners (Fig. 3). The set-up involved the expansion of the upper arch to accommodate the forward positioning of the lower arch. Moreover, expansion of the lower arch to provide space to move lower incisors lingually.
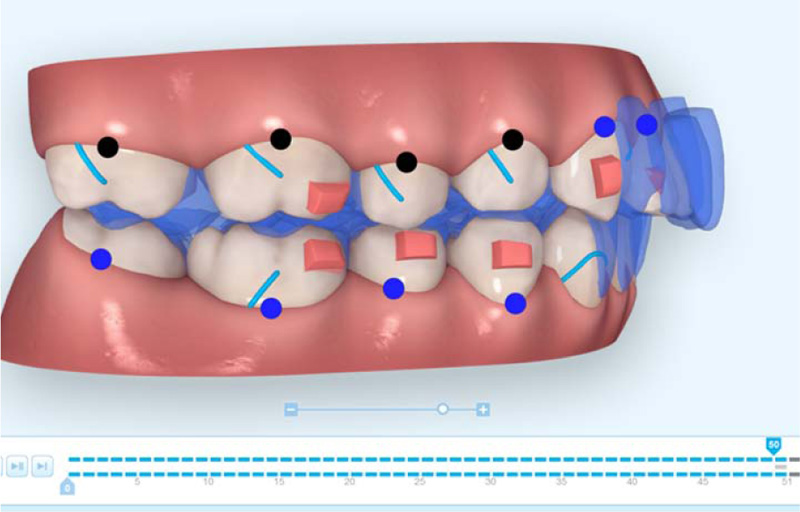
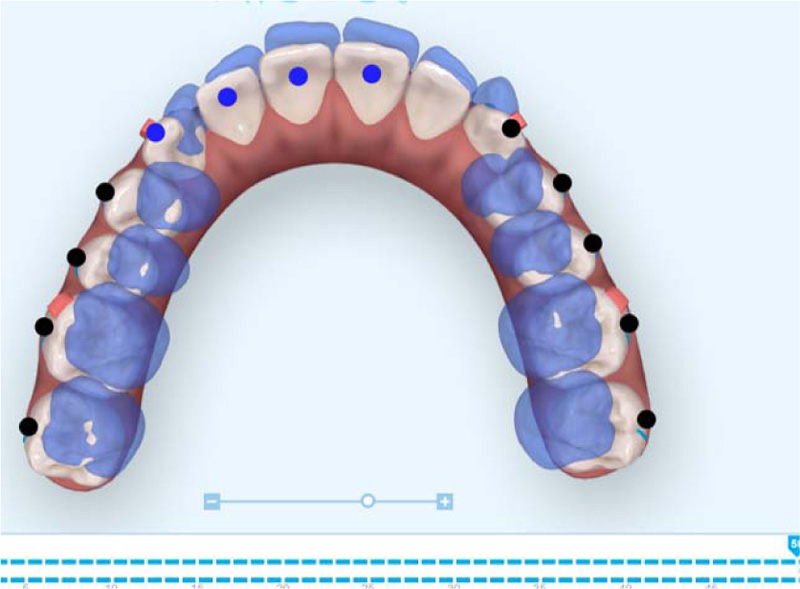

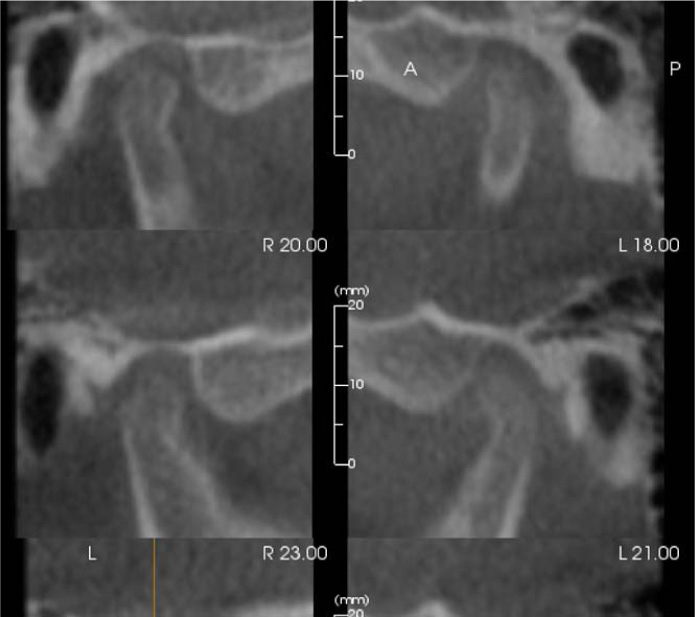
Treatment began with weekly changes of the invisalign aligners in addition to Class III elastics (From upper first molars to lower canines cutouts) (Fig. 3a) (5/16” 4oz full time) that were extended from the upper first molars to the lower canines. The reason for beginning with Class III elastics was to improve the inclination of the upper and lower incisors prior to the Class II correction. The Class III elastics assisted with proclining the upper incisors and retroclining the lower incisors to provide sufficient anterior clearance for the future Class II correction. Progress records were taken approximately 1 year into treatment. The inclination of the upper and lower incisors had improved at the time of the progress records and was assessed using the lateral cephalometric radiograph as well as cone-beam computed tomographic (CBCT) (i-CAT FLX, DEXIS, Hatfield, PA, USA) slices of the upper and lower incisors (Fig. 4). The next step of treatment involved switching to Class II elastics (RMO, Denver, Colorado, USA) from the upper canines to the lower molars to begin the Class II correction. Class II elastics of 5/16”, 4.5oz were worn during the day, and Class II elastics of 3/16”, 4.5oz were worn during the night. This Class II elastic design was used for three months. Next, mini brackets with hooks were bonded to the upper first premolars and lower first molars, and Class II elastics of 3/16”, 8oz were used full time with the remaining aligner trays of the initial digital treatment plan. When the initial set of aligners was finished, a refinement scan for additional aligners was completed. This second digital treatment plan (Fig. 5) was designed to increase the palatal root torque on the maxillary central and lateral incisors and improve the rotation of the maxillary left canine. The mini brackets were left in their positions on the teeth, and the patient wore the same 3/16”, 8oz Class II elastics with the additional 17 active aligners.


3. RESULTS
(Fig. 6 and 8) and Table 1 show improvement of the patient’s profile and occlusion. The skeletal treatment results included a reduction in the ANB angle from 9.4 degrees to 6.4 degrees, and Wits appraisal was improved from 5.9mm to 2 mm. The dental treatment results included correction of the upper incisor inclination with an improvement in the UI-SN angle from 89.0 degrees to 103.4 degrees. The lower incisor inclination improved compared to the initial, with a LI-GoGn angle from 103.0 degrees to 101.0 degrees. The Class II molar relationship was corrected with a resulting improvement in the overbite and overjet. The soft tissue profile and chin-throat depth also improved due to the forward rotation of the mandible. Follow-up photographs were taken one year after treatment to record the stability of the treatment results. The patient was very happy with his treatment results.


| Measurement | Initial | Progress | Final | Norm |
| SNA (º) | 84.7 | 84 | 85.8 | 82 |
| SNB (º) | 75.3 | 75.8 | 78.3 | 80.9 |
| ANB (º) | 9.4 | 8.3 | 6.4 | 1.6 |
| Wits Appraisal (mm) | 5.9 | 7.3 | 2 | -1 |
| Y-Axis -- Downs (SGn-FH) (º) | 60.9 | 61.2 | 62.6 | 60.4 |
| SN - GoGn (º) | 30.3 | 31.9 | 27.8 | 32.9 |
| FMA (MP-FH) (º) | 22.2 | 23.3 | 23.4 | 24.2 |
| U1 - NA (mm) | -0.5 | 2.6 | 1.9 | 4.3 |
| U1 - SN (º) | 89 | 101.9 | 103.4 | 102.7 |
| L1 - NB (mm) | 8.5 | 6.2 | 8.8 | 4 |
| L1 - GoGn (º) | 103 | 99 | 101.1 | 93 |
| Lower Lip to E-Plane (mm) | 4 | -2.9 | 1.5 | -2 |
| Upper Lip to E-Plane (mm) | 1.6 | 0.2 | -0.5 | -5.3 |
| Nasolabial Angle (Col-Sn-UL) (º) | 97.1 | 93 | 91.1 | 102 |
4. DISCUSSION
Teenage patients that present beyond the age of a functional appliance with a significant Class II molar relationship may be a reason that a practitioner hesitates in offering clear aligner therapy as a treatment option. Previous attempts to minimize lower incisor proclination when using Class II mechanics include mechanics such as lower premolar extractions [18-20] or skeletal anchorage devices [21-25]. These mechanics have shown to be technique sensitive and may have little or minimal effect on the prevention of lower incisor proclination when used with Class II mechanics [26]. The mechanics used in this case (beginning with class III elastics) could be used as an alternative treatment option to skeletal anchorage or extraction of lower premolars to minimize lower incisor proclination during Class II mechanics. Using class III elastics to improve the inclination of the upper and lower incisors was the first step to correcting the Class II occlusal relationship in this case. Moving to the mini-bonded brackets allowed increased elastic strength, which allowed the dental changes necessary for this correction. Levelling the arches and intrusion of posterior teeth with a clear aligner allowed the vertical bite jump. This was incorporated into the digital treatment plan and allowed the mandible to autorotate forward, which also assisted in the Class II correction.



The increased overbite is another challenge in this case. A few factors in this case allowed us to achieve the desired overbite correction. Achieving the desired inclination of the upper incisors was attained by prescribing these movements in the digital treatment plan and was supported by Class III elastics. Intruding lower incisors was supported by rectangular horizontal bevelled attachments. The lower arch expansion created the space required to intrude the lower incisors.

Another important factor in the success of this case was developing the anterior clearance necessary to achieve the Class II correction. At first, this was achieved by improving the incisor inclination and levelling the upper and lower arches. At the end of the first set of aligners, the initial overjet we had created had been taken up by the Class II correction. Therefore, additional proclination of the upper incisors was prescribed in the second set of aligners. It is reasonable to plan a second set of aligners using a digital scan in these types of cases to re-evaluate the desired tooth movements [3]. It is often necessary to over-prescribe certain desired movements, as the clear aligner trays may not express the same extent as the digital treatment plan shows [5].
It is becoming more common that patients in this age group are requesting esthetic treatment options [1]. They often present the past point of using a functional appliance and may not want the risks associated with surgical treatment. This case report presents an esthetic treatment option that can achieve the desired results without the need for large devices such as fixed Class II correctors or skeletal anchorage. The treatment mechanics, in combination with patient compliance, can result in successful treatment outcomes for this type of occlusion.
Although the patient’s initial CVM was estimated at stage 5/V [13-15], forward mandibular positioning was achieved in this case. This agrees with recent studies that questioned the validity of the CVM in determining mandibular growth for treatment planning in skeletal Class II cases [16, 17].
It is to be noted that this new approach can eliminate the need for orthognathic surgery in similar cases. According to a recent systematic review, there is no difference between cases treated with camouflage orthodontics and those treated with orthognathic surgery. As a result, using nonsurgical techniques to reduce surgical complications, like those described in this case report, may be a recommended course of action for patients who are in their late adolescent years.
SUMMARY AND CONCLUSION
In summary, this treatment sequence provided an esthetic and minimally invasive approach. The mechanics used with the clear aligners and elastics allowed the desired treatment results to be achieved. This may be a treatment option to consider when a similar patient presents that does not want to undergo braces or surgical treatment.
LIST OF ABBREVIATION
| CBCT | = Bone-Beam Computed Tomographic |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Informed consent was obtained.
STANDARDS OF REPORTING
CARE guidelines were followed.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

