All published articles of this journal are available on ScienceDirect.

Radicular Dens in Dente: Review of the Literature with Report of a Rare Case in a Child
Authors Info & Affiliations
Abstract
Introduction:
Dens invaginatus is an extremely rare developmental disturbance that can occur in primary, permanent, or supernumerary teeth due to invagination of the enamel organ into the dental papilla during tooth development. The clinical recognition of the radicular variant of dens in the dente is challenging as it is mostly asymptomatic with a normal-appearing clinical crown and is incidentally discovered in radiographs.
Case presentation:
This report describes a case of the radicular variant of dens in dente that involved the mandibular lateral incisor in an 8-year-old child. The affected tooth was symptomatic and was extracted as a part of treatment.
Conclusion:
Although the present case required extraction since it was associated with periapical infection, in other cases, treatment may be rendered with appropriate restorative/endodontic procedures with a keen intent to avoid sacrificing the involved tooth as has been reported earlier and reviewed herein.
1. INTRODUCTION
Dens invaginatus is a developmental disturbance that can occur in primary, permanent, or supernumerary teeth due to invagination of the enamel organ into the dental papilla during tooth development [1].
This entity was first reported in the literature by a dentist named “Socrates,” who documented his findings in the Dentists Register in 1856. Busch, in 1897, coined the term “Dens in Dente” supposing the involvement of two dental ‘elements’ [2]. Dens invaginatus is also familiarly known by its various synonyms like invaginated odontome, dilated gestant odontome, dilated composite odontome, deep foramen caecum, tooth inclusion, dentoid in dente, gestant odontome, and dents telescopes [1]. While the permanent maxillary lateral incisors are most commonly involved, premolars, canines, and less frequently, the molars are also seen to be affected by dens in dente [3, 4]. Most of the reported cases show no gender predilection, whereas female predominance has been reported in a few cases [5].
Depending on the site of invagination, dens in the dente may be categorized as having coronal and radicular variants, with the latter thought to arise secondary to a proliferation of Hertwig’s root sheath into the dental papilla after completion of root development, which is being rarely reported in the literature [3].
The present case is unique in the occurrence of the comparatively rare radicular variant of dens in the dente involving the mandibular lateral incisor.
2. CASE PRESENTATION
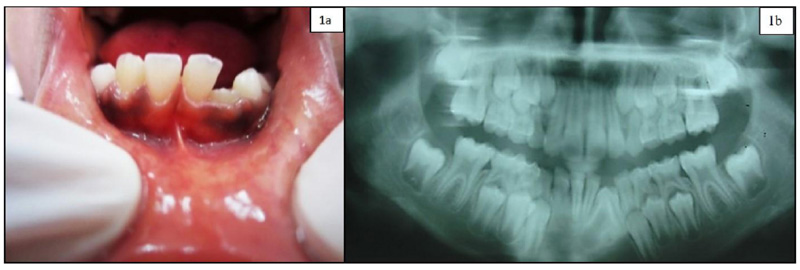
An 8-year-old female presented with the chief complaint of severe pain in the lower anterior region of the jaws for 4 days. She reported mild to moderate pain with associated swelling in the same region in the last 1 month and narrated a history of trauma in the same site four years prior for which no dental/medical consultation was made.
An extraoral non-descript swelling that was tender on palpation and firm in consistency was noted in the region of the chin. Bilaterally, the submandibular lymph nodes were mobile and tender. Intraoral examination revealed obliteration of the vestibular space from the left deciduous second molar to the right canine and tenderness to percussion in the corresponding teeth, prompting a clinical diagnosis of ‘acute periapical abscess i.r. to permanent mandibular left lateral incisor (tooth number 32)’.
Radiographic examination revealed incomplete root formation of the partially erupted permanent mandibular left lateral incisor with radicular dilation bordered by radio-opaque lines (Fig. 1a, 1b), suggesting a radiographic diagnosis of ‘Supernumerary tooth/ Odontome/Traumatic malformation of 32’. The involved tooth was extracted, following which the specimen was sent for histopathological examination.
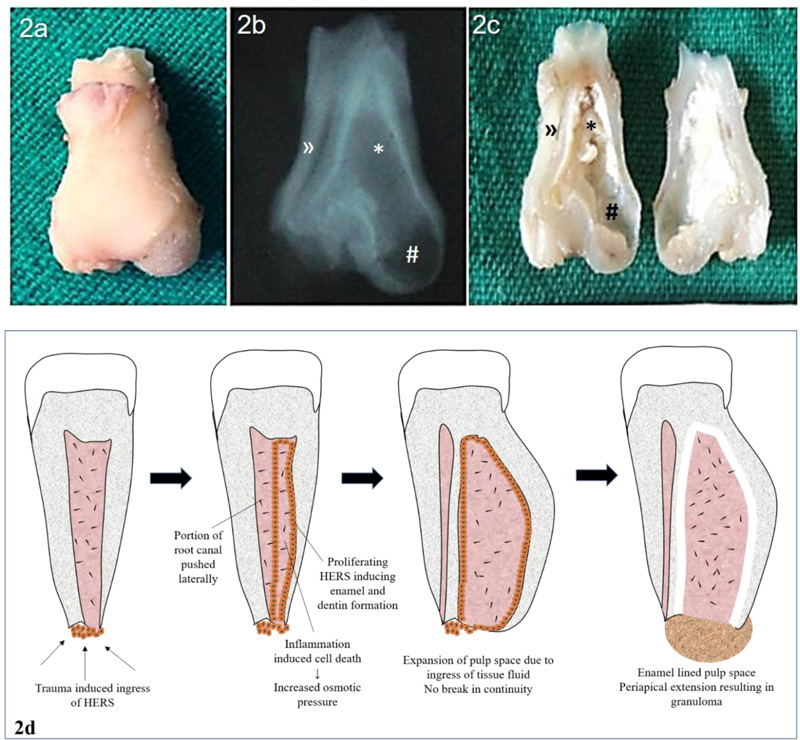
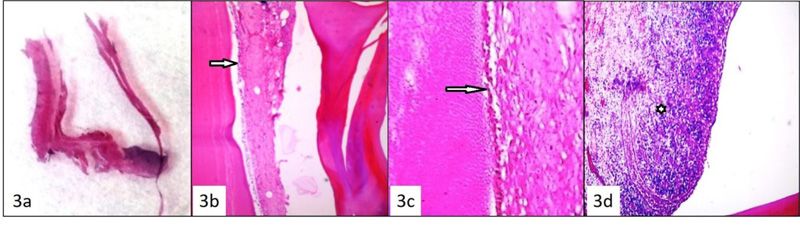
Grossly, the tooth specimen (32) showed a dilated root surrounded by soft tissue. Upon decalcification and longitudinal bisection, the tooth specimen showed the presence of two root canals (one large and one small) (Fig. 2a, 2c). Microscopic examination of the decalcified tooth specimen showed odontoblasts bordering the pulp cavity (Fig. 3b, 3c), arrow).
| Author | Year | Age | Gender | Tooth | Periapical Radiolucency | Associated Signs and Symptoms |
|---|---|---|---|---|---|---|
| Bhatt AP, Dholakia H [6] | 1975 | 24 | F | 34 | Present | Associated with abscess and periapical infection |
| Soames JV, Kuyebi TA [10] | 1982 | 9 | F | 22 | Present | Rarefying osteitis |
| Chen RJ et al. [3] | 1986 | 21 | F | 18 | Present | Tooth decay, associated with supernumerary tooth, fusion |
| Schwartz SA, Schindler WG [4] | 1996 | 16 | F | 23 | Present | Throbbing pain, not tender on percussion |
| Sauveur G, Sobel M, Boucher Y [11] | 1997 | 22 | M | 22 | Osseous rarefaction at apical third | Swelling with sinus tract Mobility + (no pocket, caries, trauma) |
| Pandey SC, Pandey RK [12] | 2005 | 14 | F | 14 | Present | Mobile, painful, associated with crown like structure inside the tooth |
| Neves FS et al. [13] | 2010 | 24 | F | 22 | Present | Pain |
| Sabhlok S. et al. [14] | 2012 | 25 | F | 18 | Sinus tract Tender on percussion |
Pain with pus discharge Extraoral ulcer |
| Beena VT et al. [15] | 2012 | 20 | F | 45 | Present | Cuspal anomaly, pain on percussion, depressible in the socket |
| Verma et al. [16] | 2013 | 11 | M | 34,44 | Well-defined invagination into the pulp canal from the radicular portion of mandibular premolars | Spontaneous, severe, and nocturnal pain in the mandibular right posterior tooth (36 and 46), asymptomatic premolars |
| Gannepalli et al. [17] | 2014 | 38 | M | 18 | Abnormal 18 with a bulbous root with an apical crescent-shaped invagination associated with periapical radiolucency. | Severe continuous pain in the region of the upper right third molar area for 3 months. |
| Moreno APD et al. [18] | 2017 | 13 | M | 42 | Intraosseous position of the tooth with dysmorphic root | Pain in the region of unerupted 42, erythematous gingiva |
| Karuna et al. [19] | 2018 | 12 | F | 34,44 | Open apex with a well-defined invagination in the apical third of the root canal | Asymptomatic 34 and 44, Pain in the region of unerupted 47 |
| 12 | M | 34,44 | Open apex with a well-defined invagination in the apical third of the root canal |
Asymptomatic 34 and 44, Pain in the region of unerupted 35 |
Granulation tissue was composed chiefly of lymphocytes, plasma cells, macrophages, and proliferating endothelial cells in a loosely collagenous stroma with cord-like epithelial proliferation (Pic. 3d, Asterix) and was confined to the apical opening of the larger canal. A histologic diagnosis of dens in dente (Radicular variant) was thus made.
3. DISCUSSION
Radicular dens in dente is a developmental anomaly, where the invagination of the tooth structure is confined to the root. The clinical crown of the involved teeth often appears to be normal. The radicular variant of dens in the dente has been discussed by Bhatt and Dholakia [6], who theorized that radicular invagination usually results from infolding of Hertwig's Epithelial Root Sheath (HERS) and takes its origin within the root after development is complete [6, 7]. The involved root shows features like dilation and compression of the pulp space along with a small opening [4]. In-folding of Hertwig’s sheath in radicular dens in the dente is usually associated with pulpal necrosis and periapical lesions [8].
While Schulze C and Brand E, in 1972, proposed a 12-type classification of dens in the dente based on the clinical and radiographic appearance of the affected tooth, the classification by Oehlers FA, in 1957, was found to be more convenient for usage [9]. Furthermore, Oehlers, in 1958, noted two distinct types of radicular dens in the dente:
Type I manifests as an exaggerated infolding of the root lined by cementum.
Type II reveals a saccular dilated invagination within the root (also dilated) and lined by enamel [3].
Accordingly, the present case was termed Type II of radicular dens in the dente, where a saccular dilated invagination within the root lined by enamel was evident. While the crown showed mild distortion with no evidence of caries, the root was noted to be disproportionately dilated and enclosing two well-demarcated root canals bordered by dentin. The lining of the enamel was radiographically evident only in the larger dilated canal. Long strands of epithelium proliferating amidst the granulation tissue surrounding the apex lent credibility to the pathogenesis of radicular dens in the dente arising by means of ingrowth of HERS. Although this entity is rare in occurrence, a review of the reported cases has been summarized in the table below.
3.1. Our Proposed Hypothesis for the Lining of Enamel and Dilatation of the Root Canal
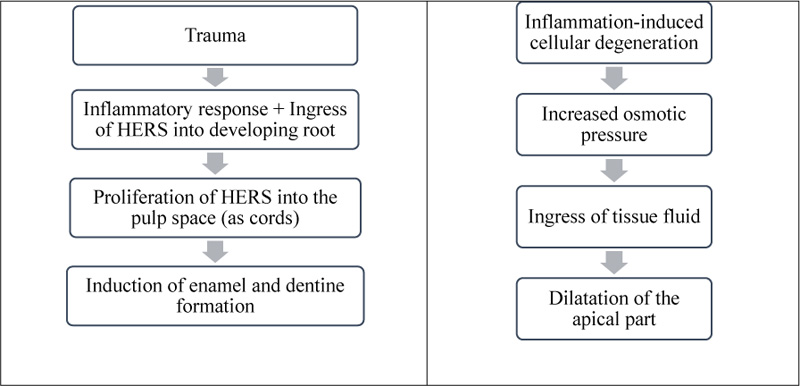
The history of previous trauma to the same region, coincident with the time of scheduled development of the involved tooth, may have forced the HERS to be aberrantly located within the root canal. Ensuing inflammation would have triggered the proliferation of HERS that would have reciprocally interacted with the dental mesenchyme, resulting in the formation of enamel within the root canal.
Furthermore, inflammation-associated cell death/ degeneration would have increased the osmotic pressure within the pulp chamber, leading to ingress of tissue fluid resulting in volumetric expansion, thereby leading to dilatation of the root. Further/ sustained increase in pressure might have led to the creation of ‘weak spots’ in the region of infolding, leading to the confluence of pulpal and periapical spaces (Fig. 2d).
3.2. Importance of Recognition of this Entity
The clinical recognition of the radicular variant of dens in the dente is challenging as it is mostly asymptomatic with a normal-appearing clinical crown and is incidentally discovered in radiographs. Most symptomatic cases are associated with pain and inflammation (Table 1). Few cases have been reported to be associated with dental caries, wherein the progress of caries would be relatively faster as ‘pathways’ for the spread of infection exist by virtue of the dilated root canal, thus contributing to a poor prognosis. A clinician suspecting a tooth to be involved by a radicular variant of dens in the dente may confirm the finding through thorough dental and radiographic examination, tests for tooth vitality, and evidence of discharge. Recently, clinicians have used spiral computed tomography to obtain better details regarding the root anatomy to facilitate better clinical outcomes [9]. Appropriate restorative/endodontic procedures need to be performed with a keen intent to avoid sacrificing the involved tooth [5]. However, in the present case, the wide-open apex (inflamed and infected) with granulation tissue precluded the possibility of conservation and the involved tooth was extracted.
CONCLUSION
The prognosis of a radicular variant of dens in the dente seems better in the case of Type I than Type II as the former has a root confined by an invaginated cementum, while the latter may not permit complete restoration due to the dilated root. Increasing reportage of this relatively rare dental anomaly may help in formulating guidelines on the management of the radicular variant of dens in the dente. A detailed case history, clinical examination, and a good diagnostic radiograph (preferably IOPA) aid in the preoperative diagnosis of this entity. Early diagnosis may help save the involved teeth by prompt intervention through appropriate restorative procedures. (Fig. 4)
LIST OF ABBREVIATIONS
| HERS | = Hertwig’s Epithelial Root Sheath |
| IOPA | = Intra-oral Peri-apical |
AUTHORS’ CONTRIBUTIONS
KB participated in the diagnosis, preparation, and editing of the manuscript. NM and SN contributed to the literature search and refining of the manuscript. SB participated in the process of diagnosis. NKP, AL, and SD contributed to reviewing and editing the manuscript.
ETHICAL STATEMENT
Ethical clearance was obtained from the ethics committee of Manipal College of Dental Sciences, India (Ref No. 13154). A copy of the IEC clearance is available.
CONSENT FOR PUBLICATION
Written informed consent was obtained from the patient’s next of kin for publication of this case report and any accompanying images. A copy of the written consent is available for review by the editor-in-chief of this journal.
AVAILABILITY OF DATA AND MATERIALS
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
STANDARDS OF REPORTING
CARE guidelines were followed
FUNDING
None.
CONFLICT OF INTEREST
The authors of this case report declare that they have no competing interests.
ACKNOWLEDGEMENTS
Declared none.

