All published articles of this journal are available on ScienceDirect.

Perspectives on Dental Caries: A Cross-Sectional Study among Parents of Primary School Children in Saudi Arabia
Authors Info & Affiliations
Abstract
Background:
Dental caries is one of the most prevalent chronic childhood diseases affecting many people worldwide. Many people do not recognize the early signs of dental caries or its causes, which is crucial for the prevention and early intervention of the disease and consequently less-invasive and cheaper treatment options.
Objective:
This study aimed to evaluate the perspectives of parents about the meaning, causes, and early signs of dental caries, the association of tooth discoloration with decay, and the effect of different socio-demographic variables on the knowledge of patients regarding caries.
Methods:
Questionnaires were distributed to parents of primary school children in the region of Madinah, Saudi Arabia. Meaning of dental caries, early signs, causes of tooth discoloration related to decay, and the effect of different socio-demographic variables were calculated. Multiple linear regression analysis was carried out to identify significant predictor variables associated with caries knowledge scores.
Results:
There was a total of 2690 respondents. The majority had average caries knowledge scores. Lighter shades of tooth discoloration were reported to be associated with stains and warranted home care only, while darker shades were associated with caries and yielded a necessity for a visit to the dentist. Different socio-demographic variables had an effect on the caries knowledge of the parents.
Conclusion:
There is a need for increased knowledge about the early signs of dental caries among parents. Delayed recognition of signs of dental caries has a detrimental effect on the teeth of children and leads to seeking dental care at the later stages of the disease process. Community-oriented programs are fundamental for improving caries knowledge, its clinical presentations starting from its early signs, causes, and prevention.
1. INTRODUCTION
Discoloration of teeth is a common cause for seeking oral healthcare among dental patients [1]. Tooth discoloration is a broad term linked to multiple extrinsic and intrinsic causes, including medications, hypoplasia, fluorosis, pulpal necrosis, and ageing [2]. Dental caries also leads to discoloration of teeth. The risk for caries results from the interplay between physical, biological, environmental, lifestyle, and dietary behaviors [3, 4]. In 2010, untreated deciduous teeth caries was one of the most prevalent conditions globally, affecting a wide range of children, with a prevalence of 9% of the population [5, 6]. A high prevalence of dental caries was reported among children in Saudi Arabia, estimated to be approximately 80% for the primary dentition and 70% for permanent dentition [7].
The color of carious lesions is one of the clinical criteria used for estimating the severity and progression of carious lesions [8]. As dental caries progresses from early to advanced stages, different shades varying from beige to black can be detected, where active lesions tend to be light yellow/beige, and slowly progressing or arrested lesions usually appear darker [9]. Dental caries begins with an incipient lesion confined to the enamel layer and is associated with plaque accumulation [10]. Incipient lesions manifest as chalky white areas of discoloration secondary to demineralization. As caries progresses into the dentin, the overlying translucent enamel reveals the color of underlying caries and appears yellowish brown. Extensive caries that involves the destruction of both enamel and dentin produces a color that ranges from light brown to dark brown or almost black [1].
Severe dental caries adversely affects the quality of life. Furthermore, untreated caries leads to local and systemic clinical complications related to the infectious process [11, 12]. Pulp involvement, fistula, abscess, and pain are significant complications [13, 14] that affect a child’s quality of life with compromised chewing efficiency, sleeping difficulties, poor appearance, low attention, low self-esteem, and social rejection [15]. However, dental caries is one of the common preventable childhood diseases where it can be arrested and potentially reversed in its early stages [12, 16, 17]. Parents’ perceptions and behaviors regarding the oral health of their children represent a cornerstone in establishing dental health and preventing caries [18].
A study conducted among Mexican immigrant caregivers of young children reported that the mothers of Mexican immigrants believed that the unrecognized causes of dental caries were related to poor oral hygiene and sweet food. The study also reported an association between the use of darker discoloration terms and severe dental caries. Seeking professional dental care was associated with teeth defined as both structurally damaged and dark in color. It also confirmed the need for increased knowledge about the early signs of dental caries [3]. Parent’s perception of early signs of dental caries in their children has not been widely explored in the literature, whereas this has an important impact on the early detection and prevention of this common chronic disease.
Therefore, the aims of this regional study were to assess the parents’ beliefs about the meaning and causes of dental caries, early signs and causes of tooth discoloration related to decay and determination of the need for dental care for their children based on evaluation of tooth discoloration. This study also aimed to measure the awareness of effective preventive measures and the understanding of the relationship between oral hygiene, diet and dental caries and evaluate the effect of different socio-demographic variables on caries knowledge levels of parents of primary school children in the region of Madinah, western Saudi Arabia.
2. MATERIALS AND METHODS
2.1. Study Design and Sample Size Calculation
This is a questionnaire-based cross-sectional survey conducted between December 2020 and January 2021. Ethical approval was obtained by Taibah University College of Dentistry Research Ethics Committee (TUCDREC/19092020). The survey was authorized for distribution by the Ministry of Education represented by the General Administration for Education in Al Madinah Al Munawwarah region. Inclusion criteria were primary caregivers of children attending primary schools in Al Madinah Al Munawwarah Region, including the cities of Madinah, Badr, Khaibar, Alhanakiah, and Mahd Althahab. The sample size was calculated to be 2332 participants associated with a confidence interval of 99.99% using Epi info software (TM 7.2.3.1, Trademark for Centers for Disease Control and Prevention (CDC), USA). This was established based on a population size of 161,327, which is the total number of current primary school students enrolled in the year 2020-2021 in the region, according to the Ministry of Education. The expected frequency was 50%, the margin of error was 4%, and the design effect and cluster size were both set at 1. An initial random sample of 2332 was determined for a 99.99% power of study; however, sending the survey to a randomized sample of schools was difficult. Therefore, the Ministry of Education distributed the questionnaire to all primary schools in Al Madinah Al Munawwarah Region through the Ministry’s formal online school platform “Madrasati.”
2.2. Questionnaire Design
The questionnaire construction was designed based on a previous similar study [3]. It was constructed in English before being translated into Arabic, which is the local language in Saudi Arabia. Piloting the study by distributing the Arabic questionnaire to pre-test for accuracy was conducted on a sample of 30 parents with demographic characteristics similar to those of the test population and re-administered after 2 weeks on the same sample. Revision and rephrasing were carried out whenever needed to ensure clarity and simplicity of the questionnaire. The Cappa test was found to be 0.795. Participants involved in the pilot study were excluded from the main study. A description of the study and confirmation that participation was completely voluntary was explained in the questionnaire. After consenting to participate, participants were given 45 close-ended questions grouped into 5 categories addressing demographics and socioeconomic factors, participants’ basic and advanced knowledge of dental caries, its causes, presentations, and the need for seeking dental care. The primary outcome measures included oral health knowledge of the parents pertaining to the meaning of dental caries, early signs and causes of tooth discoloration related to decay and awareness of the relationship between diet, oral hygiene measures and dental caries. Secondary outcome measures included the effect of different socio-demographic variables on this knowledge and awareness.
| Demographics | Number (%) |
|---|---|
|
Gender of Parent Male Female |
749 (27.8%) 1941 (72.2%) |
|
Nationality Saudi Non-Saudi |
2270 (84.4%) 420 (15.6%) |
|
School Type Private Private and public Public |
146 (5.4%) 48 (2.8%) 2496 (92.8%) |
|
School Location Madinah City Outside Madinah |
2419 (89.9%) 271 (10.1%) |
|
Number of Children 1-3 4-6 |
1180 (43) 1510 (57) |
|
Age of Youngest Child in Family <6 6-12 |
1757 (65.3) 933 (34.7) |
|
Age of Oldest Child in Family <6 6-12 13-18 |
20 (0.7) 1309 (48.7) 1361 (50.6) |
|
Father’s Education Primary school or less High school Diploma University Higher education |
575 (21.4%) 819 (30.4%) 186 (6.9%) 923 (34.3%) 187 (7.0%) |
|
Mother’s Education Primary school or less High school Diploma University Higher education |
584 (21.7%) 767 (28.5%) 163 (6.1%) 1079 (40.1%) 97 (3.6%) |
|
Monthly Family Income 5K or less 5K-15K more than 15K |
1167 (43.4%) 1238 (46.0%) 285 (10.6%) |
|
Marital Status Married Divorced Widow |
2509 (93.3%) 113 (4.2%) 68 (2.5%) |
|
Father’s Occupation Public sector employee Private sector employee Self employed Student Unemployed |
1481 (55.1%) 426 (15.8%) 248 (9.2%) 25 (.9%) 510 (19.0%) |
|
Mother’s Occupation Public sector employee Private sector employee Self employed Student House wife |
441 (16.4%) 93 (3.5%) 43 (1.6%) 29 (1.1%) 2084 (77.5%) |
|
Medical and Dental Insurance Yes No |
414 (15.4%) 2276 (84.6%) |
2.3. Statistical Analysis
The collected data were statistically analyzed using (IBM-SPSS Statistics for Windows, Version 21.0. IBM Corp. Released 2012. Armonk, NY, USA). Various socio-demographics of parents and their children were calculated and presented as absolute numbers and percentages. Responses to knowledge questions on caries (these were divided into basic and advanced) were given marks for acceptable answers that defined the level of basic and advanced knowledge of dental caries. Paired sample t-test was used to identify if there was a significant difference between basic and advanced knowledge scores for individuals. Student’s t-test and ANOVA (with LSD post-test) were used to explore significant differences in total scores (these are sums of basic and advanced caries knowledge scores) when grouped according to different socio-demographic variables. Moreover, multiple linear regression analysis was carried out to identify significant predictor variables associated with basic and advanced caries knowledge scores separately. Significance was set at p ≤ 0.05.
3. RESULTS
A total of 3292 parents attempted to respond to the questionnaire. However, there were 602 who did not consent to participate and hence did not complete the questionnaire. These were excluded from the study sample resulting in a total of 2690 responses, constituting 81.7% of the total responses. Table 1 displays the demographics of children and parents. Most respondents (72.2%) were mothers of targeted school children, as shown in Table 1. Moreover, the majority of respondents (84.4%) were Saudi nationals. Most children (92.8%) were enrolled in public schools, and most schools (89.9%) were in the city of Madinah.
Table 2 shows questions on basic and advanced knowledge regarding dental caries. For basic and advanced knowledge questions on dental caries, respondents were given marks for each correct answer they provided. This produced marks for basic knowledge ranging from 0-7 (maximum possible score), and for advanced knowledge, the marks ranged from 0-9 (which is the maximum possible score). Regarding basic caries knowledge, when asked about what dental caries mean, around half of the respondents (53%) identified caries as discoloration while the majority (78.8%) identified caries as cavitation. Unfortunately, a high percentage (87.0%) did not relate dental caries with bacterial activity. When asked about the first signs of caries, around 49.2% identified this as changes in surface color, while 44.0% reported cavitation to be the first sign of caries.
| Basic caries knowledge | - | Advanced caries knowledge | - |
| Questions and answers | Marks given for answers | Questions and answers | Marks given for answers |
| Frequency and (%) | Frequency and (%) | ||
| What does dental caries mean to you? | Meaning of white discoloration | ||
| Stains 902 (33.5%) | 1 | ||
| Color change | Caries 749 (27.8%) | 0 | |
| No 1263 (47.0%) | 0 | Pulp inflammation 128 (4.8%) | 0 |
| Yes1427 (53.0%) | 1 | Don't know 911 (33.9%) | 0 |
| Cavitation | Meaning of beige discoloration | ||
| No 570 (21.2%) | 0 | Stains 1262 (46.9%) | 1 |
| Yes 2120 (78.8%) | 1 | Caries 565 (21.0%) | 0 |
| Pulp inflammation 184 (6.8%) | 0 | ||
| Don't know 679 (25.2%) | 0 | ||
| Bacterial activity | Meaning of yellow discoloration | ||
| No 2341 (87.0%) | 0 | Stains 1415 (52.6%) | 0 |
| Yes 349 (13.0%) | 1 | Caries 431 (16.0%) | 1 |
| Pulp inflammation 171 (6.4%) | 0 | ||
| Don't know 673 (25.0%) | 0 | ||
| Don’t know | Meaning of brown discoloration | ||
| 138 (5.1%) | 0 | Stains 393 (14.6%) | 0 |
| Caries 1308 (48.6%) | 1 | ||
| Pulp inflammation 314 (11.7%) | 0 | ||
| Don't know 675 (25.1%) | 0 | ||
| What are first signs of caries? | Meaning of black discoloration | ||
| Don't know 182 (6.8%) | 0 | Stains 77 (2.9%) | 0 |
| Change in surface color 1324 (49.2%) | 1 | Caries 2065 (76.8%) | 1 |
| Cavitation 1184 (44.0%) | 0 | Pulp inflammation 236 (8.8%) | 0 |
| Don't know 312 (11.6%) | 0 | ||
| What are the causes of dental caries? | Response to white and beige discoloration | ||
| Poor oral hygiene | Nothing serious 263 (9.8%) | 0 | |
| No 1002 (37.2%) | 0 | Ask the dentist 560 (20.8%) | 1 |
| Yes 1688 (62.8%) | 1 | Home care suffices 1073 (39.9%) | 1 |
| I go to the dentist 794 (29.5%) | 1 | ||
| Sugar intake | Response to yellow discoloration | ||
| No 526 (19.6%) | 0 | Nothing serious 257 (9.6%) | 0 |
| Yes 2164 (80.4%) | 1 | Ask the dentist 604 (22.5%) | 1 |
| Home care suffices 1154 (42.9%) | 0 | ||
| I go to the dentist 675 (25.1%) | 1 | ||
| Nursing bottle | Response to brown discoloration | ||
| No 2146 (79.8%) | 0 | Nothing serious 149 (5.5%) | 0 |
| Yes 544 (20.2%) | 1 | Ask the dentist 607 (22.6%) | 1 |
| Home care suffices 670 (24.9%) | 0 | ||
| I go to the dentist 1264 (47.0%) | 1 | ||
| Response to black discoloration | |||
| Nothing serious 90 (3.3%) | 0 | ||
| Ask the dentist 359 (13.3%) | 1 | ||
| Home care suffices 359 (13.3%) | 0 | ||
| I go to the dentist 1882 (70.0%) | 1 | ||
| Total possible marks | 7 | 9 |
| Scores of basic caries knowledge |
No of the respondents obtaining the score % |
Scores of advanced caries knowledge |
No of the respondents obtaining the score % |
|---|---|---|---|
| 0 | 32 (1.2%) | 0 | 31 (1.2%) |
| 1 | 140 (5.2%) | 1 | 105 (3.9%) |
| 2 | 471 (17.5%) | 2 | 170 (6.3%) |
| 3 | 659 (24.5%) | 3 | 273 (10.1%) |
| 4 | 655 (24.3%) | 4 | 517 (19.2%) |
| 5 | 501 (18.6%) | 5 | 708 (26.3%) |
| 6 | 192 (7.1%) | 6 | 565 (21.0%) |
| 7 | 40 (1.5%) | 7 | 251 (9.3%) |
| 8 | 51 (1.9%) | ||
| 9 | 19 (.7%) | ||
| Mean of marks (calculated as a percent) | 51.8±19.6 | 52.7±18.0 |
| Model 14 | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | 95.0% Conf. Interv. for B | Collinearity Statistics | |||
|---|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | Tol. | VIF. | |||
| (Constant) | 1.826 | .234 | 7.796 | .000 | 1.37 | 2.285 | |||
| Income | .231 | .045 | .107 | 5.136 | .000 | .143 | .319 | .898 | 1.114 |
| Parents who examine their childrens’ teeth | .393 | .092 | .086 | 4.257 | .000 | .212 | .574 | .953 | 1.049 |
| Age child starts brushing | -.081 | .019 | -.087 | -4.20 | .000 | -.119 | -.043 | .906 | 1.103 |
| Children who use fluoride toothpaste | .129 | .041 | .063 | 3.136 | .002 | .048 | .209 | .973 | 1.027 |
| Children who do not visit the dentist due to high cost | .755 | .080 | .259 | 9.455 | .000 | .599 | .912 | .516 | 1.938 |
| Children who visit the dentist | .923 | .097 | .303 | 9.540 | .000 | .733 | 1.113 | .385 | 2.598 |
| Children who fear dentists | .693 | .078 | .221 | 8.842 | .000 | .539 | .847 | .623 | 1.606 |
| Parents who think milk teeth require no treatment | .541 | .085 | .135 | 6.330 | .000 | .373 | .708 | .847 | 1.180 |
| Children who do not visit the dentist due to clinics are far away | .323 | .099 | .067 | 3.250 | .001 | .128 | .518 | .910 | 1.099 |
| Duration of brushing | .196 | .059 | .066 | 3.292 | .001 | .079 | .313 | .976 | 1.025 |
| Children who have caries | -.222 | .072 | -.065 | -3.08 | .002 | -.363 | -.081 | .884 | 1.132 |
| Gender | .182 | .064 | .056 | 2.823 | .005 | .056 | .308 | .970 | 1.031 |
| Variables of the regression model |
Unstandard Coeffs |
Stand. Coeffs |
t | Sig. | 95.0% Conf. Interv. for B | Collinearity Statistics | |||
|---|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | Tol. | VIF | |||
| (Constant) | 3.489 | .241 | 14.5 | .000 | 3.017 | 3.961 | |||
| Number of times child brushes per day | .296 | .039 | .156 | 7.64 | .000 | .220 | .372 | .927 | 1.078 |
| Parents who examine their childrens' teeth | .650 | .106 | .125 | 6.12 | .000 | .442 | .859 | .931 | 1.074 |
| Children who visit the dentist | .174 | .031 | .115 | 5.63 | .000 | .113 | .234 | .919 | 1.088 |
| Children who have caries | -.292 | .081 | -.074 | -3.59 | .000 | -.452 | -.133 | .899 | 1.113 |
| Number of children in primary edu | -.133 | .040 | -.066 | -3.30 | .001 | -.212 | -.054 | .960 | 1.042 |
| Income | .103 | .053 | .042 | 1.95 | .051 | -.001 | .206 | .846 | 1.182 |
| Parents who help their children brush | .236 | .088 | .053 | 2.69 | .007 | .064 | .408 | .982 | 1.018 |
| Duration of brushing | .178 | .068 | .052 | 2.63 | .009 | .045 | .311 | .976 | 1.025 |
| Nationality | -.190 | .090 | -.043 | -2.10 | .036 | -.367 | -.013 | .910 | 1.099 |
| Children who do not visit the dentist due to high cost | -.142 | .069 | -.043 | -2.04 | .041 | -.278 | -.006 | .886 | 1.128 |
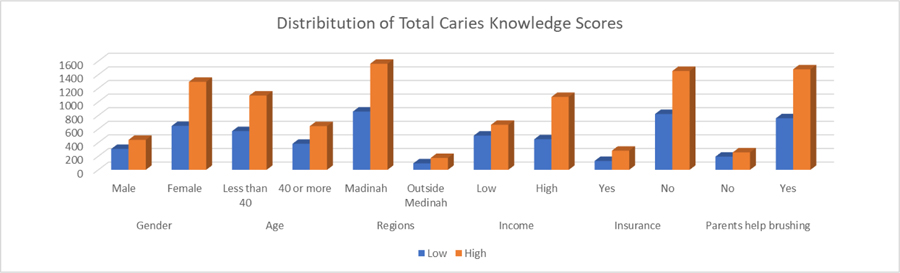
Regarding causes of dental caries, a high percentage of respondents identified poor oral hygiene (62.8%) and sugar intake (80.4%) to be factors contributing to dental caries, while the nursing bottle (79.8%) was not reported to be associated with dental caries. Advanced caries knowledge was defined as the ability to correlate different colors of tooth discolouration with caries and responses to these. It was found that white (33.5%), beige (46.9%), and yellow (52.6%) discoloration were more associated with stains rather than caries; however, a significant percentage did not know what these shades of discoloration meant (Table 2). Brown (48.6%) and black (76.8%) discoloration were associated with caries rather than stains. Responses to white (39.9%), beige (39.7%), and yellow (42.9%) discoloration warranted home care only, while brown (47.0%) and black (70.0%) discoloration yielded a necessity for communication or a visit to the dentist. Table 3 shows the performance of participants for both types of questions. The majority of participants had a score ranging between 2-5 out of a total of 7 for basic caries knowledge and 3-6 out of a total of 9 for advanced caries knowledge. Paired samples t-test showed no significant differences (P=0.062) between scores of basic and advanced caries knowledge (after being expressed as a percent) for individuals. T-test was calculated for total knowledge scores and showed that females and Saudi nationals had significantly higher total caries knowledge scores when compared to either males or non-Saudis (p= <0.001 and 0.002 respectively). The presence of medical insurance and the school sector did not show significant differences (P= 0.084 and 0.212 respectively) (Fig. 1).
ANOVA (with LSD post hock test) was used similarly to find significant differences in total caries knowledge (TCK) scores among variables with more than 2 groups. Results showed significantly higher total knowledge scores for higher-income groups (p<0.001 for all) (except between 5-15K SAR and more than 15 SAR with P=0.347). No significant differences in TCK Scores were observed for individuals residing in various regions of the province (P>0.05 for all). Generally, there were significantly higher TCK score levels with the increase in paternal and maternal education (p<0.05) (Fig. 1).
Regarding paternal careers, the lowest means for TCK scores were recorded by parents who were students (44.0%), followed by the unemployed and self-employed (with 49.6% each), followed by private sector employees (51.3%), while public sector employees had the highest means (52.9%) which were significantly different to all other career groups. Regarding maternal careers, the lowest means of TCK scores were registered similarly for student mothers (48.5%), followed by housewives (51.0%), followed by public sector employees (53.8%), and finally, private sector employees and the self-employed (nearly 54.5% each). Regarding the effect of marital status on TCK, widows and widowers registered the lowest mean TCK scores (45.7%), followed by married (51.6%) and divorced (54.4%). All marital status groups were significantly different to each other.
Multiple linear regression analysis was carried out separately for basic and advanced knowledge scores obtained by respondents to determine the correlation of different variables with the knowledge level. Table 4 shows variables that were included in the model as significant predictors for basic caries knowledge. In this regression model, R =0.329, R2 =0.108, adjusted R2=0.103, ANOVA of regression model was highly significant (P=0.000). Thus the model is capable of predicting 10.8% of the variance of basic caries knowledge scores. However, the Durban-Watson test (=1.132) points to a possible serial correlation. Table 5 shows the coefficients used to build the model. All of these variables shared in the model are significant, with a p-value <0.001 for most of them. 95% confidence interval shows valid limits of different variables where predictions of the regression model are most accurate. Tolerance (Tol.) shows values more than 0.2 for all the variables, indicating no serious multicollinearity.
It was found that significant predictor variables in the regression model of basic caries knowledge scores were: parents with a higher income, female gender, parents who examine their childrens’ teeth, children who start brushing at an earlier age and for a longer duration of time, children who use fluoride toothpaste, children who regularly visit the dentist, children who do not visit the dentist due to high cost, fear of dentists and because clinics are far away, parents who think milk teeth require no treatment and parents whose children have caries.
Multiple linear regression analysis was carried out to find significant predictor variables for scores of advanced caries knowledge (Table 5). Results of regression analysis shows the following: R= 0.111, R2= 0.107, Durban-Watson= 0.774, ANOVA<0.001. Table 5 shows coefficients of the regression model (Beta weights), which help interpret the unique contribution of each of the independent variables as predictors of the dependent variable. Tol (Tolerance)= 1/VIF (which is the variance inflation factor) values for all variables is more than 0.2, which points to the absence of multicollinearity.
It was found that parents with a higher income, parents who help their children brush, increased number of times child brushes per day and who brush for a longer duration of time, parents who examine their childrens’ teeth, children who visit the dentist, children who have caries, the lower the number of children in primary education, non-Saudi nationals, and children who do not visit the dentist due to high cost are all variables associated with a higher level of advanced caries knowledge scores.
4. DISCUSSION
Much research has been devoted to dental caries, its process, and its prevalence. However, tooth discoloration due to dental caries has been a less investigated feature in the caries pathological process [19]. This large scale regional cross-sectional study aimed to evaluate parents’ beliefs about the meaning and causes of dental caries, early signs of tooth discoloration related to decay, and determination of the need for dental care for their children based on a survey of 2690 parents of primary school children in the region of Madinah, Saudi Arabia.
In this study, basic caries knowledge was represented by the meaning of dental caries, early signs and causes of dental caries, while advanced caries knowledge delved into specific caries related tooth discoloration shades and its implications and responses of parents to different caries related tooth discoloration. The meaning of dental caries has been mostly associated with cavitation, with a lesser percentage associating it with discoloration and a rather high percentage not correlating dental caries with bacterial activity. Although no studies have focused exclusively on the meaning of dental caries to primary caregivers of children, studies have agreed that parents have limited or inaccurate knowledge of oral health [20-22]. When asked about the first sign of dental caries, around 49% identified this as changes in surface color, while 44% reported cavitation to be the first sign of caries. Observing the development of the first clinical signs of caries is crucial for the prevention and early treatment of the disease. Evidence suggests that parents or caregivers are not aware of the early signs of caries; hence, they seek dental care at the later stages of the disease process [23]. Others believe that tooth decay is inevitable despite taking any kind of preventive measures [24]. Another study found that caregivers of children with caries did not realize that their children had caries [25].
Additionally, some unexplored variables can have a significant influence on the oral environment. The use of probiotics and natural compounds can modify clinical and microbiological parameters, and they could also affect caries development. All these variables should be considered in future clinical trials [26, 27].
With regards to causes of dental caries, a high percentage of respondents have identified sugar intake and poor oral hygiene to be factors contributing to dental caries. Indeed, this is in line with most of the evidence in the literature where the significance of oral hygiene and dietary habits is well documented [24]. However, a high percentage of parents in the region did not perceive the nursing bottle to be associated with dental caries. In a study by Arora et al., many parents were found to have inaccurate knowledge regarding causes of dental caries where the majority linked their children’s dental caries with inadequate tooth brushing, whereas most parents did not realize that caries is also associated with inappropriate feeding habits including nursing bottles [28]. Information on practical ways to control the bedtime feeding practices of young children needs to be made available, and the importance of modifying dietary habits needs to be emphasized so that parents become more vigilant about their child’s oral health behaviors. Recent research showed that deposition of hydroxyapatite on polymeric composite resin could prevent secondary caries on the margins of restorations. The use of these emerging compounds could help parents in controlling hypomineralization and secondary caries risk [29].
Correlating different shades of tooth discoloration with caries and responses to these were recorded and considered advanced caries knowledge. It was found that white, beige, and yellow discoloration were more associated with stains rather than caries. Brown and black discoloration were associated with caries rather than stains. Lighter shades warranted home care only, while darker shades yielded a necessity for communication or a visit to the dentist. This is consistent with the study by Masterson et al., where respondents associated darker shades of tooth discoloration with extensive caries and destruction of tooth structure [30]. These darker shades were more likely to generate a visit or care from a professional dental source, while teeth described to have a lighter shade resulted in either no action being taken or home care responses [30]. Discerning whether parents associated particular color shades with particular degrees of tooth decay and what actions they took, as a result, is essential as recognizing lighter shades such as white, beige, or yellow being early signs of dental caries, e.g., “white spot lesions” may induce earlier intervention and consequently less-invasive and cheaper treatment options. Moreover, this will help foster preventive protocol measures rather than restorative treatment.
When correlating different socio-demographic variables with the total caries knowledge scores, mothers were deemed to have higher scores compared to fathers. The findings of the study by Pani et al. seem to suggest that Saudi mothers have a relatively better understanding of the oral health of their children compared to fathers. This may be that mothers are thought to be more involved in childcare, despite recent literature suggesting that fathers are increasingly becoming more involved with childcare [31]. Saudi nationals and families with a higher income and education and parents with an occupation in the private or public sector also had higher scores. This is in agreement with the cumulative evidence pertaining to the relationship between parental education and socioeconomic status and the level of parental knowledge and awareness of oral health [32-34]. No difference in total caries knowledge scores was found between families living in the main city of Madinah compared to ones living in rural or suburban cities. Similarly, insurance was found not to make a difference, nor families with children enrolled in private or public schools. However, it is important to note that this may not reflect oral health behavior where differences may be detected.
Although this study involved a large sample size, a limitation is that it relied on self-perceived data, which could be a source of bias. Furthermore, including other regions in Saudi Arabia would have the potential benefit of comparison for regional differences. Further studies focusing exclusively on the meaning and signs of dental caries in other regions in Saudi Arabia and other countries are needed in addition to identify whether cultural factors have an effect on the recognition and interpretation of dental decay. Although many studies assessing the prevalence of dental caries in Saudi Arabia have been conducted extensively, it is important to understand how people recognize and interpret dental caries in Saudi Arabia. This baseline data is necessary for setting oral health goals for government and the dental profession officials in Saudi Arabia and planning a road map with a clear starting point when promoting oral public health programs and education, which are the most important caries preventive measures. It will also have an impact on oral health practices, dental service utilization, and communication with oral health professionals.
CONCLUSION
There is a need for increased knowledge about the early signs of dental caries among parents. Delayed recognition of signs of dental caries by parents has a detrimental effect on the teeth of their children and leads to seeking dental care at the later stages of the disease process. Socio-demographic factors influence knowledge of dental caries. A dynamic and practical community-oriented program is fundamental for improving the knowledge on dental caries and its clinical presentations, starting from its early signs, causes, and prevention.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was gained from Taibah University College of Dentistry Research Ethics Committee (TUCDREC/19092020/DHashem). Participants gave their written informed consent to participate in the questionnaire.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All research procedures on humans were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
CONSENT FOR PUBLICATION
All participants in the study gave their written informed consent for participation and publication of the data obtained from the study.
STANDARDS OF REPORTING
STROBE guidelines and methodologies were used in this study.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the current study are available from the corresponding author [D.H] on reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to thank the Ministry of Education represented by the General Administration for Education in the Al Madinah Al Munawwarah region for their assistance in distributing the questionnaire through their online education platform.

