All published articles of this journal are available on ScienceDirect.

Perspectives of Dental Practitioners Regarding Their Readiness for Medical Emergencies: A Study in Saudi Arabia
Authors Info & Affiliations
Abstract
Background:
Training dental practitioners on emergency preparedness and response is essential for the successful management of medical emergencies.
Objectives:
To assess the perceptions of dental practitioners in Saudi Arabia about their readiness to manage medical emergencies in the dental practices.
Methods:
This cross-sectional survey was conducted among dental practitioners working in 52 dental centers in Saudi Arabia. Questionnaires mainly gathered data on the measures taken by dental practitioners to prevent medical emergencies, BLS certification, availability of essential drugs and equipment, and perceptions of dental practitioners regarding the adequacy of their training for medical emergencies.
Results:
Of the total 270 participants, the majority reported that they take medical history (94%), perform visual inspection (90%), consult with patients’ physician when needed (89%), and modify treatment plan as necessary (94%). However, only 19% of them routinely take baseline vital signs for their patients and 52.6% have valid BLS certification. Only 29.6% and 16.3% of dental practitioners have reported that they have all essential drugs and equipment, respectively.
Conclusion:
The preventive measures for medical emergency appears to be deficient because most dental practitioners are not routinely taking baseline vital signs for their patients. This important issue is combined with shortage of BLS certification among dental practitioners and inadequate availability of all medical emergency drugs and equipment in dental practices.
1. INTRODUCTION
Life-threatening medical emergencies can and do occur in dental practices with considerable frequency [1, 2]. Therefore, training dental practitioners on emergency preparedness and response is essential for the successful management of medical emergencies.
The readiness of dental practitioners should include thorough patient evaluation, reviewing medical history, adequate training on medical emergencies, valid BLS certification, and the availability of appropriate emergency drugs & equipment [3-7]. International guidelines suggest that dentists should participate regularly in annual or bi-annual practical training on how to recognize and manage medical emergencies, including those that require Cardiopulmonary Resuscitation (CPR) and the use of Automated External Defibrillator (AED) [8]. However, the requirement for the availability of medical emergency drugs and equipment in dental offices differs from country to country [9]. The European and UK Resuscitation Council recommends that immediate access to basic resuscitation drugs and equipment (emergency medications, bag-valve-mask device, oxygen tank, and suction tips) and an AED should be readily available for all dental practitioners in their dental practices [9, 10].The availability of an AED in dental practice is mandatory in New York, Mississippi, and Massachusetts in the United States [11]. Furthermore, the American Dental Association council recommends that at least the basic recommended emergency drugs and equipment should be attainable in dental practices [4].
The general consensus regarding the preparedness of handling a medical emergency in dental practice has been found to be inadequate among dental practitioners in many countries [12-14]. In Saudi Arabia it was found that dental personnel do not feel competent to perform CPR on their patients and have a deficiency in performing certain emergency procedures. In addition, the availability of emergency protocols together with essential drugs and equipment in dental practices was also found to be deficient [15-17].
The aim of this study is to assess dental practitioners’ perceptions regarding their readiness for medical emergencies in dental practice. This was carried out by assessing the preventive measures taken by dental practitioners when evaluating dental patients, the availability of medical emergency drugs, and equipment in dental clinics. Likewise, their perceptions regarding the adequacy of their training on medical emergencies, together with their recommendations regarding the issue.
2. MATERIALS AND METHODS
The present study was approved by the ethics committee of our research center in Saudi Arabia (RC14.017). The confidential, anonymous, and self-administered questionnaires were formulated in English and then distributed in person to 52 different dental practices in Saudi Arabia. Random sampling was achieved by choosing dental settings from different geographic locations in the Eastern, Central, and Western regions of Saudi Arabia. Two hundred and seventy dental practitioners voluntarily agreed to participate in this study. Sample size was calculated using Raosoft, Inc. sample size calculator. Considering 95% Confidence Interval, expected number of dental practitioners was 250; the sample size obtained was 270 with a 5% margin of error.
This study was carried out by assessing the preventive measures taken by dental practitioners when evaluating dental patients, the availability of medical emergency drugs, and equipment in dental clinics. Likewise, their perceptions regarding the adequacy of their training on medical emergencies, together with their recommendations regarding the issue.
The questionnaires consisted of 8 main areas: (1) Demographic data, (2) Type of medical emergencies encountered by dental practitioners, (3) Preventive measures taken by dental practitioners (complete medical history, taking of vital signs, performing a visual inspection, consulting the patient's physician when need be, and modifying the treatment plan when necessary), (4) BLS certification, (5) Availability of clear medical emergency protocols in their workplace, (6) Availability of medical emergency drugs (anti-allergy, histamine-blocker, vasodilator, bronchodilators, anti-platelet, anti-hypoglycemia), (7) Availability of emergency equipment (Tourniquets, Suction tips, Disposable syringes, Automated Cardiac Defibrillator, Magill intubation forceps, Bag-valve-mask device, Oxygen tank), and (8) Dental practitioners’ perceptions about their training to prevent, recognize, and manage medical emergencies in the dental office, together with their recommendations regarding the issue.
The data were entered into a spreadsheet and analyzed using IBM SPSS Statistics for Windows, version 20.0 (IBM Corp, Armonk, NY, USA). The variables were expressed as mean and standard deviations and were explored to test for normality. The data set followed a non-normal (non-Gaussian) distribution. Therefore, results were also presented as medians and interquartile range, whereas the difference in dental practitioners’ perceptions with regard to their level of training (specialists versus non-specialists) was analyzed using non-parametric Wilcoxon’s Mann Whitney test for p-value calculations at the 5% level of significance. A P-value <0.05 was considered statistically significant.
3. RESULTS
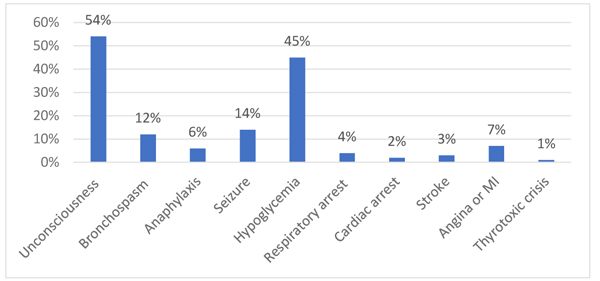
Out of the total 335 dental practitioners, 270 participated in the study giving a response rate of 80%. It was reported that 60% of dental practitioners had experienced a medical emergency in their workplace. The types of medical emergencies encountered reported were in the following frequencies: unconsciousness (54%), hypoglycemia (45%), seizure (14%), bronchospasm (12%), angina or myocardial infarction (MI) (7%), anaphylaxis (6%), respiratory arrest (4%), stroke (3%), cardiac arrest (2%), and thyrotoxic crisis (1%) (Fig. 1).
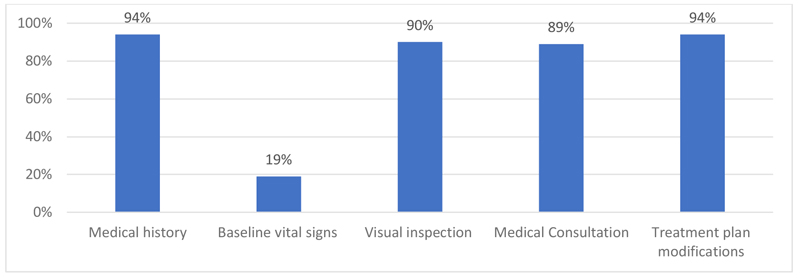
The routine measures taken by dental practitioners to prevent medical emergencies practiced were in the following frequencies: Ninety-four percent of dental practitioners always obtained a complete medical history for their patients, 90% perform a visual inspection, 89% carry out medical consultations with the patient’s physician when necessary, and 94% makes necessary modifications in the treatment plan of medically compromised patients. However, only 19% of participants reported taking baseline vital signs for their patients (Fig. 2). Furthermore, only 52.6% of the participants had a valid BLS certificate.
It was reported that 68% of dental practitioners had a clear medical emergency protocol available in their dental practices. Furthermore, it was reported that essential medical emergency drugs and equipment were available in the following frequencies: anti-allergy (68%), histamine-blocker (56%), vasodilator (53%), bronchodilator (23%), anti-platelet (59%), anti-hypoglycemic (70%), tourniquet (37%), suction tips (61%), disposable syringes (80%), AED (26%), Magill intubation forceps (20%), oxygen tank (70%), and bag-valve-mask device (46%) (Table 1).
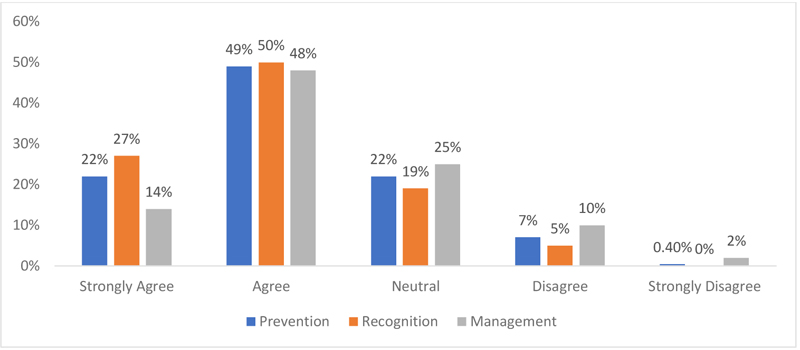
It should be noted, however, that only 29.6% and 16.3% of dental practitioners reported to have all essential drugs and equipment, respectively. When dental practitioners were asked about their training in medical emergency, the highest percentage reported to agree with the adequacy of their training to prevent (49%), recognize (50%), and manage (48%) medical emergencies (Fig. 3). Furthermore, 51.9% of practitioners recommended the need for additional training in medical emergencies, such as continuous education courses and workshops. No significant differences were found when comparing the perspectives of specialists and non-specialists’ dental practitioners, as shown in Table 2.
4. DISCUSSION
As shown in the present study, 60% of dental practitioners had encountered medical emergencies in their dental practices. This result is not surprising since other previous reports have shown comparable data [1, 2, 16].However, when considering the shortcomings of the emergency medical services system in the Kingdom of Saudi Arabia [18], our results shed more light on the crucial need for appropriate readiness of dental practitioners for medical emergencies in their dental practices.
In the same context, dental practitioners in Saudi Arabia are anticipated to take strict preventive measures at all times since studies have shown that cardiovascular diseases are an increasing public health concern in the Middle East and the Gulf Council Countries (GCC) [19-21].The prevalence of hypertension, for instance, is relatively high (26.1%) in Saudi Arabia [22].This suggests that there is an apparent possibility of routinely treating dental patients with cardiovascular diseases. However, our present data showed that only 19% of dental practitioners had the baseline vital signs for their patients. This is in line with previous studies in Saudi Arabia who reported that only 12% of dental practices routinely take vital signs for their patients [17].
With regard to the availability of essential medical emergency drugs or equipment in dental practices, our study showed that only 29.6% and 16.3% of dental practitioners reported to have all essential drugs and equipment, respectively. All essential drugs or equipment should be readily available in dental clinics. Therefore, the availability of only some drugs or equipment is considered inadequate. Comparable data was shown in a previous study where the lack of essential drugs and equipment was found in the Western region of Saudi Arabia [15].
With regard to BLS training, 52.6% of participants indicated that they have a valid BLS certificate, which is considered inappropriate since all dental practitioners are required to have a valid BLS certificate at all times. This may negatively affect the prevention, recognition, and management of medical emergencies in dental practices. Furthermore, when the perspectives of dental practitioners regarding the adequacy of their training in medical emergencies were evaluated, a relatively small percentage of dental practitioners ranging from 14% to 22% tended to strongly agree compared to a higher percentage, ranging from 48% to 50%, who tend to agree. This is in agreement with the data of a previous report in Saudi Arabia, which indicated that only 45% of dental practitioners felt competent to perform cardiopulmonary resuscitation in case of a medical emergency [16]. It is suggested that dental practitioners in Saudi Arabia are not highly confident about their training in medical emergencies. Furthermore, when comparing the opinions of specialists and non-specialists regarding their training in medical emergencies, no significant differences were identified, which might suggest that additional training in different dental specialties does not improve their training in medical emergencies. However, further studies are needed to clarify this issue.
In summary, the readiness of dental practitioners for medical emergencies in Saudi Arabia is deficient. This deficiency has been clearly illustrated in many instances. In other words, not routinely taking vital signs for dental patients, not all dental practitioners have a valid BLS certificate, sporadic availability of a complete set of essential medical emergency drugs and equipment. Furthermore, the opinion of dental practitioners regarding the adequacy of their training was not strongly positive.
In light of the above, it is suggested that there is a crucial need to implement further administrative measures by health authorities in Saudi Arabia. These measures might include mandatory regular training courses on advanced medical emergencies, which was also recommended by 51.9% of dental practitioners, regular audits on the validity of BLS certification, and availability of essential medical emergency drugs and equipment in dental clinics. It is recommended that practical lessons or internships on the management of medical emergencies be included in the curriculum of the training of dental practitioners.
| Drugs | Frequency (n) | Percent (%) |
|---|---|---|
| Anti-allergy | 184 | 68% |
| Histamine-blocker | 151 | 56% |
| Vasodilator | 142 | 53% |
| Bronchodilator | 63 | 23% |
| Anti-platelet | 160 | 59% |
| Anti-hypoglycemic | 188 | 70% |
| Equipment | Frequency (n) | Percent (%) |
| Tourniquets | 100 | 37% |
| Suction tips | 165 | 61% |
| Disposable syringes | 216 | 80% |
| Automated External Defibrillator | 70 | 26% |
| Magill intubation forceps | 54 | 20% |
| Bag-valve mask device | 124 | 46% |
| Oxygen tank | 188 | 70% |
| Statements | Dental Practitioners' Level of Training | n | Median (IQR) | p value |
|---|---|---|---|---|
| I am adequately trained to prevent medical emergencies in the dental office. | Specialists | 108 | 1 (1-0) | 0.332 |
| Non-Specialists | 149 | 1 (2-0) | ||
| I am adequately trained to recognize medical emergencies in the dental office. | Specialists | 107 | 1 (1-1) | 0.511 |
| Non-Specialists | 149 | 1 (2-1) | ||
| I am adequately trained to manage medical emergencies in the dental office. | Specialists | 107 | 1 (1-0) | 0.126 |
| Non-Specialists | 148 | 1 (1-0) |
5. LIMITATIONS
The study limitations are a smaller sample size.
CONCLUSION
It was concluded that the preventive measures for medical emergency appears to be deficient because most dental practitioners are not routinely taking baseline vital signs for their patients. This important issue is combined with the shortage of BLS certification among dental practitioners and inadequate availability of all medical emergency drugs and equipment in dental practices.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The present study has been approved by the Ethics Committee of King Abdullah International Medical research Center in Saudi Arabia (RC14.017).
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
STANDARDS OF REPORTING
STROBE guidelines and methodologies were followed in this study.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We thank Intisar Ahmed Siddiqui for his help in statistical analysis.

