All published articles of this journal are available on ScienceDirect.

Comparison of Surface Equivalent Dose in CBCT, Digital Panoramic and Intra-Oral X-Ray Generators Using InstadoseTM Device: An In-Vitro Study
Authors Info & Affiliations
Abstract
Background:
Radiation protection in the dental examination is often overlooked because the doses delivered are negligible. However, the volume of dental radiological examinations will constitute almost 15% of all the radiological examinations carried out in the medical field.
Aim:
This study aims to evaluate and compare the surface equivalent dose on various target organs from various radiology devices on the RINN phantom, and the effect of numerous scanning protocols on said dose using dosimetry badge (Instadose).
Objectives:
The main objective is to study surface equivalent doses delivered in various critical organ regions in the facial region with the help of an Instadose device and to compare the doses delivered between 2D programs against 3D programs.
Materials and Methods:
RINN phantom was mounted on a dental chair for use against Planmeca ProMax 3D Classic and Planmeca intraoral ProX. Models. An Instadose badge was placed on various anatomical landmarks, and radiographic exposure protocols were applied to vary the parameters. The equivalent dose was calculated by connecting the dosimeter to a laptop and performing an instant reading output on the Instadose software.
Results:
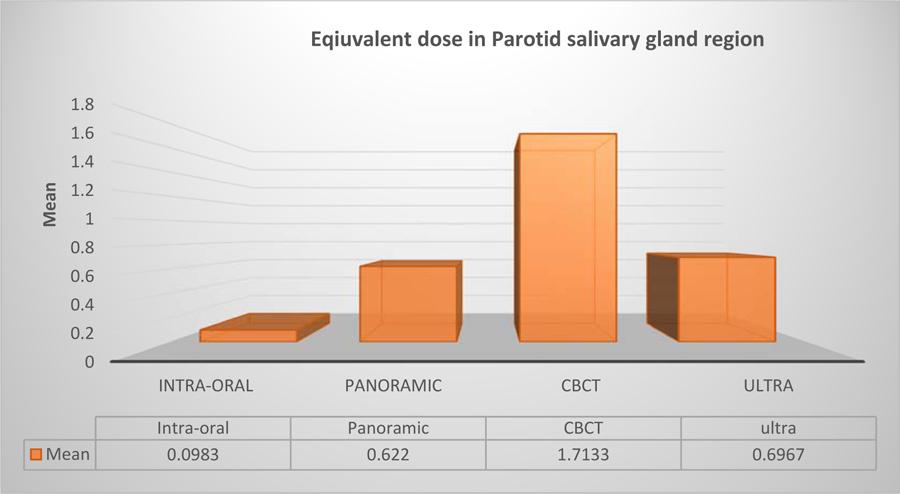
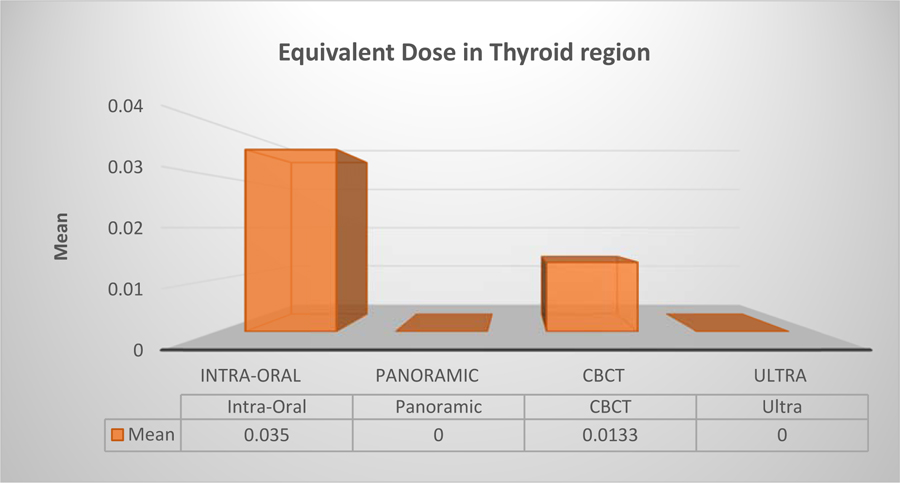
The Thyroid showed a mean of 0.350, 0.0000, 0.0133, and 0.0000 in response to exposure by intraoral machine ProX, Panoramic, CBCT, and CBCT in ULD mode respectively. The dose absorbed by the left salivary glands was found to be significantly lower than the right salivary glands in panoramic exposures.
Conclusion:
It was revealed that a significant reduction in the dose when applying the Ultra-Low Dose protocol was noticed, and it reached up to 100% in the thyroid. It was also noted that there is no need for a thyroid collar in CBCT and Panoramic exposures. Maintaining the KVp at a constant and the exposure time as a variant caused a change in the dose equivalent received by the floor of the mouth and the right salivary gland.
1. INTRODUCTION
All the radiological exposures pose the danger of adding the cumulative dose to patients. This weights down the dentist with the responsibility to warrant appropriate protection for the patient, dental personnel, and the general public. Therefore, any radiographic investigation should provide a clear potential advantage to the patient, weighing the diagnostic benefits against the risk that the exposure might cause [1]. The risk of radiation comes to be a striking community concern, mainly when multiplied by the vast number of patients being exposed to diagnostic imaging, whereas the hazard from maxillofacial imaging for an individual is not particularly high [1]
Since the radiographic examination is ranked as one of the most widely used examinations in investigative procedures in the last century, the focus on dose reduction to the patient is critical [2], for that reason, some attempts were made by machine manufactures in order to minimize the radiation dose to “As Low As Reasonably Achievable” or “As Low As Diagnostically Achievable” (ALADA) via implementation of certain practices and protocols [3]. The technical developments that were seen in the field of radiology protection in the past decade led to the development of this scientific research about this topic [4].
The purpose of this study is to investigate and compare the surface equivalent radiation dose on critical organ regions associated with ProMax 3D Classic and Planmeca ProX (Finland) using different scanning protocols to understand the advancement in the field of radiation protection. We also measured the effect of applying numerous imaging protocols of panoramic radiography and cone-beam computed tomography to understand the equivalent dose of radiation. It was also calculated that the surface equivalent dose was varied by altering KVp and exposure time in intra-oral radiography machines and CBCT machines. It was also tried to evaluate the level of dose reduction with the use of Ultra-Low Dose protocol in CBCT machine. This study will shed light on the surface equivalent dose behavior with regard to technological advancement in the software and machine hardware to provide the desired improved image quality without increasing radiation dose.
2. MATERIALS AND METHODS
In this study, a RINN trainer manikin phantom model 54/6002, serial number 6224 from DENTSPLY, was used. The instadoseTM dosimeter is a device manufactured by Microns Technologies, which is the only accredited USB-compatible dosimeter, allowing users to gain immediate feedback regarding their exposure. The advantage of Instadose is the ease of measuring the radiation dose at any given time and as many times as needed from an internet-supported computer. It has a minimal reportable dose of 0.01mSv. It employs a stable analog memory cell that is encircled by a gas-filled ion chamber. Electrons generated by the interaction of photons in the wall material will result in ionization in the airspace between the gate and chamber wall. This process will lead to an alteration in the gate charge. By evaluating the difference from one read event to the next, and in conjunction with the web-based software, the dosimeter implements the calculations of dose. The InstadoseTM software was installed on a computer from the official website after an account was created. After each exposure, interpretation was made by connecting the dosimeter to a computer in the USB port, logging in to the Instadose account, and performing device reading. The two radiographic machines that were used were given as Planmeca® ProX, Planmeca® ProX 3D Classic models. (Planmeca. Finland).
RINN phantom was mounted on a dental chair simulating a patient. InstadoseTM dosimeter was positioned on the salivary gland region, thyroid region, and floor of the mouth regions using a double-sided adhesive tape. One critical protocol that was added to the study on CBCT Mode was the Ultra -Low Dose; when applied, it modified the exposure values by decreasing the mill amperes and shortening the X-ray pulse required for each frame. The benefit of this process is decreasing radiation dose and creating a faster rotation time, which results in fewer artefacts caused by patient movements, thus used mainly in pediatric dentistry examinations.
3. RESULTS
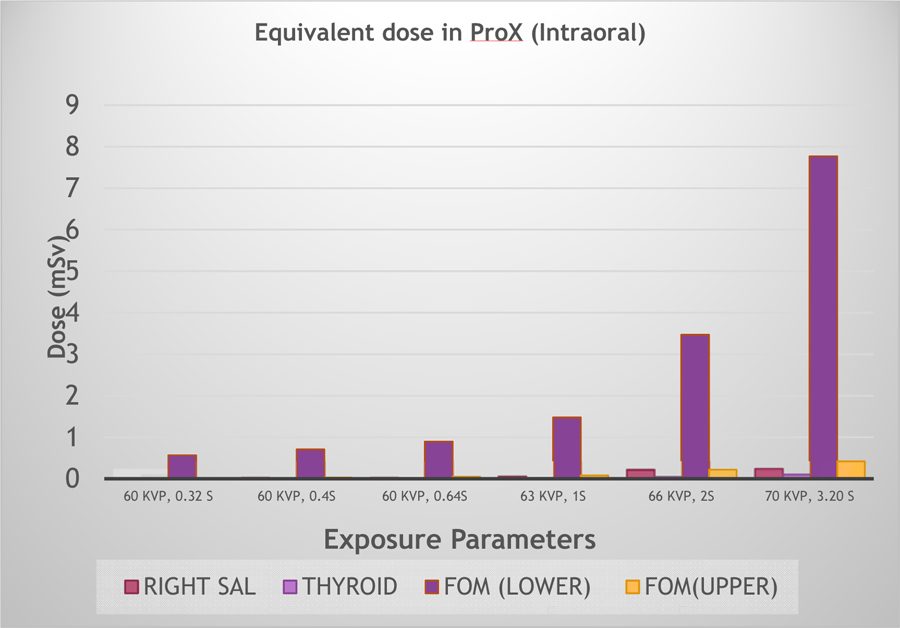
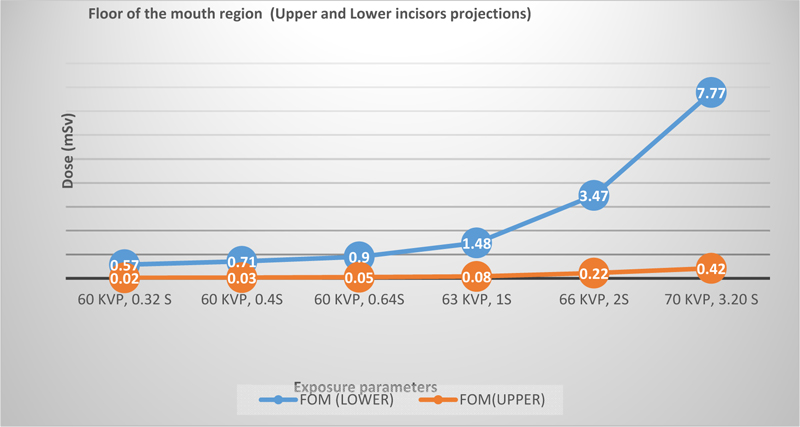
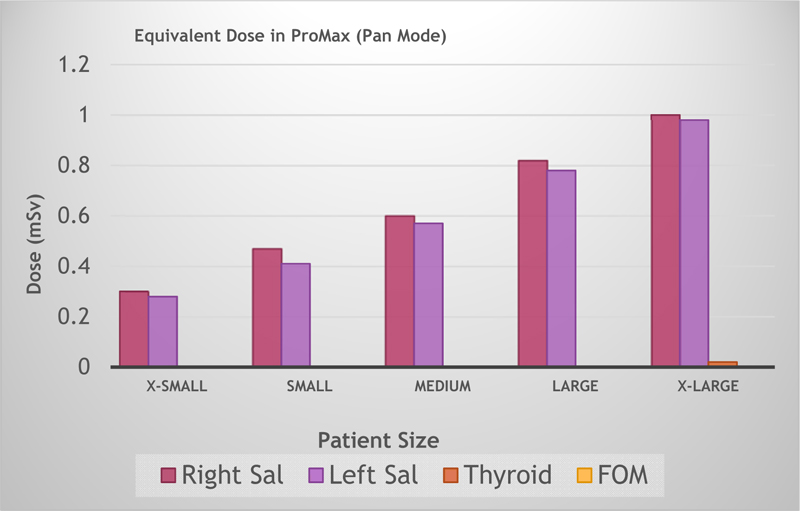
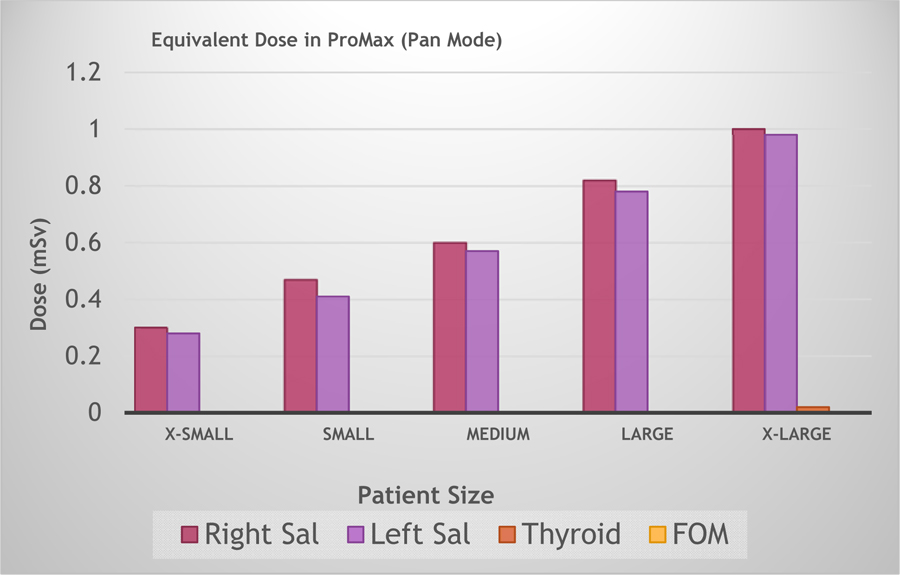
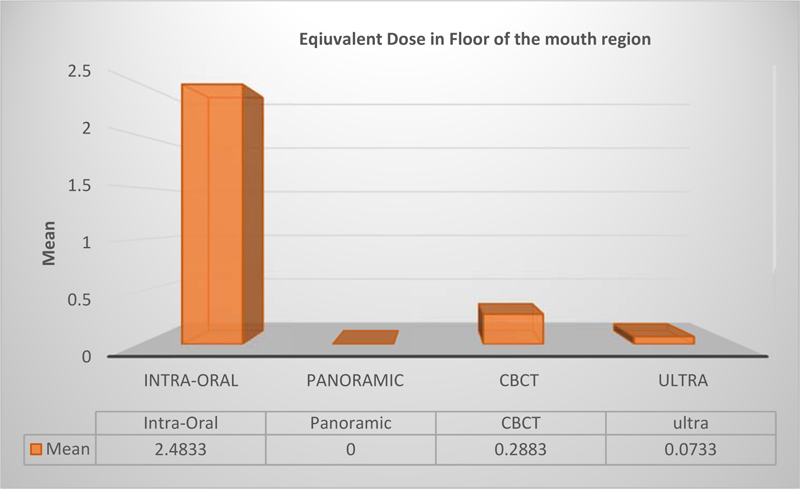
Analysis of Variance (ANOVA) was used for Statistical analysis on this study using SPSS Software. The salivary glands (parotid gland) doses were statistically significant (p= 0.006) when analyzing equivalent dose difference between intraoral ProX and CBCT Classic machines. It was shown that there is a significant statistical difference in equivalent dose when comparing between usual and ultra- low dose mode (p=0.008) (Tables 1 and 2). The floor of the mouth also showed a statistically significant difference (p=0.05) between intraoral ProX, ProMax panoramic mode, and CBCT mode (Table 2). CBCT mode showed no statistically significant difference (p-value =0.055) in comparison of surface equivalent dose with usual and the ultra-low-dose protocol in CBCT mode, which may be considered as a significant finding if the number of protocols was to be increased for follow up cases or using the CBCT exposure protocol in the pediatric population (Table 1). The right parotid salivary gland region showed a statistically significant difference in the surface equivalent doses when a patient is subjected to CBCT evaluation (Table 2). Thyroid surface equivalent doses were found to be statistically insignificant (p>0.05) when compared with all the machines and the ultra-low dose mode. (Table 3) The equivalent dose in intra-oral radiography showed significantly high results only due to extremely high exposure parameters used in intraoral machines to prove that even an intraoral machine can deliver very high doses on the floor of the mouth. When KVp and exposure time in intraoral machines were changed, the surface equivalent doses delivered at the site of the thyroid gland area increased significantly, which is important clinically to support the use of a thyroid collar for all intraoral examinations (Fig. 1). When comparing the equivalent dose in the floor of the mouth, the lower incisors projection showed a substantially higher dose in relation to the upper incisors projection as expected (Fig. 2). Equivalent doses estimation by a different protocol based on the skull size has shown varied surface equivalent doses based on the selection and is clinically important to deliver optimum safe dose with skull volume (Fig. 3). Equivalent Dose in Pro Max CBCT, with and without using Ultra-Low Dose protocol, showed an increase in the right salivary parotid gland region due to projection geometry and the location of the radiation source in the gantry. It also showed that the Ultra Low dose program considerably reduced the surface equivalent dose delivered in the right parotid gland region (Figs. 4 and 5). It also showed that pan mode and ultra-low dose CBCT mode delivered almost similar surface equivalent doses in the right parotid gland region. This is important clinically as the diagnostic data obtained from Ultra low dose CBCT is of high importance and acceptable with regard to diagnosis and treatment planning compared to 2D pan mode (Fig. 5). It also showed variation in the mean equivalent doses for the thyroid region, emphasizing the role of thyroid collar in intraoral radiology and rejecting the need of thyroid collar in Panoramic and CBCT mode as it may cast a radiopaque shadow in the region of interest (Fig. 6).
| Descriptives | ||||||||||||||||
| - | N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | |||||||||
| Lower Bound | Upper Bound | |||||||||||||||
| Right salivary gland ( Parotid ) |
PLANMECA: Kvp,ES | 6 | .0983 | .10342 | .04222 | -.0102 | .2069 | .01 | .24 | |||||||
| Protocol (PAN) | 5 | .6220 | .27905 | .12480 | .2755 | .9685 | .29 | .99 | ||||||||
| CBCT | 6 | 1.7133 | 1.19242 | .48680 | .4620 | 2.9647 | .39 | 3.21 | ||||||||
| ultra | 3 | .6967 | .31005 | .17901 | -.0735 | 1.4669 | .39 | 1.01 | ||||||||
| Total | 20 | .8035 | .91237 | .20401 | .3765 | 1.2305 | .01 | 3.21 | ||||||||
| Thyroid gland | PLANMECA: Kvp,ES | 6 | .0350 | .03987 | .01628 | -.0068 | .0768 | .01 | .11 | |||||||
| Protocol (PAN) | 5 | .0000 | .00000 | .00000 | .0000 | .0000 | .00 | .00 | ||||||||
| CBCT | 6 | .0133 | .01506 | .00615 | -.0025 | .0291 | .00 | .03 | ||||||||
| ultra | 3 | .0000 | .00000 | .00000 | .0000 | .0000 | .00 | .00 | ||||||||
| Total | 20 | .0145 | .02645 | .00591 | .0021 | .0269 | .00 | .11 | ||||||||
| Floor of the mouth |
PLANMECA: Kvp,ES | 6 | 2.4833 | 2.80148 | 1.14370 | -.4566 | 5.4233 | .57 | 7.77 | |||||||
| Protocol (PAN) | 5 | .0000 | .00000 | .00000 | .0000 | .0000 | .00 | .00 | ||||||||
| CBCT | 6 | .2883 | .29989 | .12243 | -.0264 | .6031 | .02 | .76 | ||||||||
| ultra | 3 | .0733 | .05033 | .02906 | -.0517 | .1984 | .02 | .12 | ||||||||
| Total | 20 | .8425 | 1.82117 | .40723 | -.0098 | 1.6948 | .00 | 7.77 | ||||||||
| - | Sum of Squares | df | Mean Square | F | Sig. | |||||||
| Right Salivary Gland (Parotid ) |
Between Groups | 8.149 | 3 | 2.716 | 5.669 | .008 | ||||||
| Within Groups | 7.667 | 16 | .479 | |||||||||
| Total | 15.816 | 19 | ||||||||||
| Thyroid gland | Between Groups | .004 | 3 | .001 | 2.473 | .099 | ||||||
| Within Groups | .009 | 16 | .001 | |||||||||
| Total | .013 | 19 | ||||||||||
| Floor of the Mouth | Between Groups | 23.320 | 3 | 7.773 | 3.133 | .055 | ||||||
| Within Groups | 39.696 | 16 | 2.481 | |||||||||
| Total | 63.017 | 19 | ||||||||||
| Tukey HSD | |||||||
| Dependent Variable | (I) Dev | (J) Dev | Mean Difference (I-J) | Std. Error | Sig. | 95% Confidence Interval | |
| Lower Bound | Upper Bound | ||||||
| Right salivary Gland ( Parotid ) |
PLANMECA: Kvp,ES | Protocol (PAN) | -.52367 | .41916 | .606 | -1.7229 | .6755 |
| CBCT | -1.61500* | .39965 | .005 | -2.7584 | -.4716 | ||
| ultra | -.59833 | .48947 | .622 | -1.9987 | .8020 | ||
| Protocol (PAN) | PLANMECA: Kvp,ES | .52367 | .41916 | .606 | -.6755 | 1.7229 | |
| CBCT | -1.09133 | .41916 | .081 | -2.2905 | .1079 | ||
| ultra | -.07467 | .50552 | .999 | -1.5210 | 1.3716 | ||
| CBCT | PLANMECA: Kvp,ES | 1.61500* | .39965 | .005 | .4716 | 2.7584 | |
| Protocol (PAN) | 1.09133 | .41916 | .081 | -.1079 | 2.2905 | ||
| ultra | 1.01667 | .48947 | .202 | -.3837 | 2.4170 | ||
| ultra | PLANMECA: Kvp,ES | .59833 | .48947 | .622 | -.8020 | 1.9987 | |
| Protocol (PAN) | .07467 | .50552 | .999 | -1.3716 | 1.5210 | ||
| CBCT | -1.01667 | .48947 | .202 | -2.4170 | .3837 | ||
| THYROID | ||
| Tukey HSD | ||
| Dev | N | Subset for alpha = 0.05 |
| 1 | ||
| Protocol (PAN) | 5 | .0000 |
| Ultra low dose | 3 | .0000 |
| CBCT | 6 | .0133 |
| PLANMECA: (intra oral Kvp,ES) | 6 | .0350 |
| Sig. | .157 | |
| Floor of the Mouth | ||
| Tukey HSD | ||
| Dev | N | Subset for alpha = 0.05 |
| 1 | ||
| Protocol (PAN) | 5 | .0000 |
| Ultra low dose | 3 | .0733 |
| CBCT mode | 6 | .2883 |
| PLANMECA: Kvp,ES | 6 | 2.4833 |
| Sig. | .118 | |
The surface equivalent dose absorbed by the right salivary gland is comparatively higher than that of the left salivary glands by a percentage ranging from 2% to 12.7% in the case of panoramic mode studied. The reduction in the dose when applying the Ultra-Low Dose protocol was up to 100%, 81.06%, and 89.47% in the thyroid, salivary gland, and the floor of the mouth, respectively, in comparison to the standard protocol with maximum shown in the thyroid gland region (Figs. 4 and 5). This is clinically validated in the case of CBCT examination in paediatric tumours and cysts, where the advantage of slicing the tumour in all three planes allows maxillofacial surgeons to treat the pathology surgically with high precision (Tables 4 and 5).
4. DISCUSSION
This study provides further evidence that a thyroid collar is not needed in panoramic exposures due to the negligible surface equivalent dose (below 0.01mSv) of radiation seen in the thyroid region. It was also noticed that in the comparison conducted between the regions, the 6thyroid region was the least affected by radiation in terms of surface equivalent dose in all radiographic techniques, supporting the study conducted by Reyhani. et al. [5].
There is evidence that a range of 3-4 minutes of cooling time was needed between exposures when using the Instadose™ device as it showed conflicting results when used repeatedly without a cooling time. It was observed that CBCT in ULD mode could replace panoramic radiography for radiological study in pediatric patients, considering its significantly low radiation equivalent dose and the large volume of image data it provides in all three planes. It has been noted that the equivalent dose absorbed by the right salivary gland in panoramic exposures is comparatively higher than that of the left salivary glands by a percentage ranging from 2% to 12.7%. This increase can be attributed to the fact that the source of radiation was originally situated at the right side, and hence the right salivary gland was subjected to an initial dose which is thought to be higher. Another finding of significant importance is the reduction in the dose when applying the Ultra-Low Dose protocol by up to 100% in the thyroid, and 81.06% in the salivary gland, as well as 89.47% in the floor of the mouth in comparison to the standard protocol (Fig. 7). This finding is in agreement with the study where Ludlow [6] et al. found an average of 77% dose reduction using the ultra-low-dose protocol. They also observed that there was no statistical reduction in the image quality between the two protocols studied.
In a study carried out by Grunheid et al. [7], the employment of a RANDO phantom and TLDs was required to perform a comparison of the absorbed dose of vital organs in CBCT, digital panoramic, and lateral cephalometric machines. In the results documented, it was noticed that the absorbed dose of target organs in digital panoramic machines was lower than the other systems. However, the organ which absorbed the highest dose was the submandibular gland, while the one with the lowest absorbed dose was the thyroid gland. Likewise, in a study by Talaeipour et al. [8], they used two conventional and digital cephalometric radiography machines and compared the absorbed dose of target organs, which led them to the conclusion that the digital system caused a substantial reduction in the absorbed dose of target organs.
Davies et al. [9], in another study, used a RANDO® phantom and TLDs, and effective doses for each protocol were calculated using the 1990 and 2007 international commission on radiological protection (ICRP) recommended tissue weighting factors (E1990, E2007). As a result, the effective dose for E 1990 and E 2007 was calculated for full field of view (FOV) of the head, 47 mSv and 78 mSv, respectively (using 13 cm FOV scan) [10]. It was also concluded that using the new generation of CBCT scanner reduces the effective dose by a larger degree when compared to the original generation machine with the same FOV using the ICRP 2007 tissue weighting factors.
Koivisto et al. [11, 12] (2014) studied 40 TLD and 20 MOSFET dosimeters to measure the effective dose. They were placed in anthropomorphic RANDO® head phantom, which was exposed to four different CBCT maxillofacial protocols. In conclusion, it was mentioned that TLD effective doses were in the range of 7.0-158.0 mSv, while the MOSFET doses range was 6.1-175.0 mSv, also that the largest variation in organ and effective dose was recorded in the small FOV protocols.
Based on these results gathered from this study, effective doses absorbed by biological organs can be measured by the equivalent dose multiplied by a tissue weighting factor, which was used in previous studies merely for comparison of different types of radiation on body organs and tissues. The reason for its legitimacy in this particular experiment is that the equivalent dose changes in accordance to KVp, time of exposure, alignment, and position of useful beam [13]. The only issue faced and thought to be related to conflicting results with regard to reading displayed by the Instadose software, and that was solved by specifying a cooling time of 3-4 minutes for the device between exposures. Each radiological examination is designated for a specific diagnostic concern. Therefore one type of imaging modality such as CBCT cannot be used for all the radiologic examinations, and CBCT is usually regarded as an additional technique rather than a replacement of traditional 2D radiography [14-16]. In post surgical healing, morphometric analysis of maxillary sinus surgeries bone morphometry beneath a periodontal phenotype can be carefully evaluated in CBCT examinations compared to other diagnostic or treatment modalities like lasers.
CONCLUSION
In this study, a RINN phantom model 54/6002, serial number 6224 was used due to lack of availability of the RANDO® anthropomorphic phantom. Therefore, we advise future researchers to use an anthropomorphic RANDO® phantom, which is a replica of the human skeleton inserted into a material that absorbs radiation comparable to that of soft tissue. It is considered by many to be the gold standard in measuring the absorbed dose, along with TLD dosimeters in order to reach more accurate results. In further research, more light should be shed on research aimed at maintaining the optimum image quality with reduction of radiation dosage to the patient.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
None.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the finding of the article is available in the Zenodo Repository at zenodo.org, reference number: https://doi.org/10.5281/zenodo.5729282.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

