All published articles of this journal are available on ScienceDirect.

Evaluation of Knowledge, Attitude and Practice of Cross Infection Control Among Students of Dentistry, Dental Hygiene, and Dental Technology in Jordan
Authors Info & Affiliations
Abstract
Background:
Cross infection control, to reduce the incidence of disease transmission between patients and dental team personnel, is an integral part of good clinical practice.
Objective:
To assess knowledge, attitude and practice of cross infection control among dental, dental hygiene, and dental technology students.
Methods:
Data were collected by a self-administrated questionnaire assessing knowledge, attitude, and practice of infection control measures. The questionnaire was published electronically to final year dental, dental hygiene, and dental technology students through student’s official social media groups .
Results:
Statistically significant difference was found in relation to students' specialization (p-value ≤ 0.05). None of the dental hygienist students had a negative attitude about infection control, while most of participants with a negative attitude were dental technology students (84.6%). No statistically significant difference (p>0.05) was found between groups in regard to cross-infection knowledge, where the level of knowledge ranged from moderate to good.
Conclusion:
Good knowledge, attitude, and practice were reported for dental and dental hygiene students, while good knowledge with a negative attitude was found amongst dental technology students. Specialty affected the practice of infection control measures, yet gender was not a significant variable. Improvement of the university curriculum, particularly for dental technology students, to increase awareness and knowledge of cross infection control is highly recommended.
1. INTRODUCTION
Cross infection implies the transmission of infection between patients and between patients and health care professionals, which can occur during the treatment of patients if meticulous preventive procedures are not observed. [1-3]. Infection control has become such an essential part of the practice to the extent that dental health workers (DHW) no longer question its necessity [4]. The objective of cross-infection control is mainly to decrease the number of pathogenic microorganisms [5] and to reduce the risk of spreading diseases. Transmission of pathogens can occur via direct contact with blood, saliva, and other secretions [6], or indirect contact with a contaminated sharp instrument, aerosols, splatters, or clothing [7, 8].
Compliance with infection control strategies is the key in preventing the spread of infections among patients and DHWs [9]. A discrepancy between knowledge and attitude related to infection control was reported, where quite less satisfactory compliance with infection control instructions was reported, in contrast to a good level of knowledge [10, 11]. Several studies revealed poor adherence to control infection standards and emphasized the need to improve related knowledge [7, 12, 13], particularly in prosthodontic practice, 14.. Dental impression and all laboratory procedures are considered a major route to the transmission of microorganisms between dental team members [7, 11, 14, 15].
In Jordan, a previous report indicated a lack of understanding and practice of infection control basics amongst not only dental and dental hygiene students but also in graduate practicing dentists and dental hygienists [16]. Despite the routine use of gloves, the majority did not practice routine handwashing, and neither wore masks or eye googles routinely [16]. On the contrary, a study in Romania showed moderate knowledge of infection control procedures between dentists [17]. Furthermore, Saudi senior dental students were found to attain a high level of infection control knowledge, and applied all necessary precautionary measures during their undergraduate program when treating patients [18]. Dental students in India, on the other hand, stated that though they were taught about the usage of antiseptic solutions, most of them did not use it for handwashing [19].
Dental institutes and health authorities usually enforce the acquisition of a high level of clinical skills and knowledge about infection control by dental students [20, 21]. Thus, the role of teaching infection control strategies as an integral part of teaching curriculum for undergraduate students and in continuous education programs is essential to enhance awareness and increase knowledge of the acknowledged standards of infection control, 18.
Up to our knowledge, there are no previous studies in Jordan that investigated the knowledge and compliance of dental team members with infection control measures, including dental, dental technology, and dental hygiene students, and the role of the university curriculum regarding infection control teaching and assessment tools. Thus, the current investigation aims to investigate the knowledge, attitude, and practice of infection control measures among those students in Jordan and to assess the role of the university curriculum as the major tool to deliver educational material related to cross-infection control.
2. MATERIALS AND METHODS
The current cross-sectional study was conducted after ethical approval was obtained from the Institutional Review Board at Jordan University of Science and Technology (JUST), Irbid, Jordan. The questionnaire was developed and reviewed by two independent expert reviewers.
A self-administrated questionnaire was used, the questionnaire was checked for validity and reliability [22]. An initial pilot study was conducted using a convenient sample of dental, dental technology, and dental hygiene students (n = 10) to ensure that the questions were clear, understandable, practical, and valid. The pilot survey was repeated three times, at three different time intervals, one week apart, to assess reliability. Accordingly, the final draft of the questionnaire was modified based on the feedback obtained from the pilot study.
The survey was published electronically as a Google form by sending the online link to the official social media groups (Facebook) of the targeted sample, which included the final year dental, dental technology, and dental hygiene students. Recruited subjects were informed that participation is voluntary, withdrawal is permitted at any time of the study, and their responses would be anonymous and handled confidentially.
The questionnaire consisted of five main parts. The first aimed to collect demographic information, including age, gender, and discipline. The second part is designed to gather information related to knowledge. The third part assessed the participants' infection control practices that involved the usage of protective barriers (mask, eyewear, head cab, gloves, gowns) and the use of precautions against injures in addition to miscellaneous questions related to the removal of accessories during a dental procedure, short nail fingers, washing hands, and washing lab coat. The fourth part evaluated the participants’ attitudes. The last part focused on the importance of cross-infection control education and evaluation of the curriculum implemented at JUST concerning infection control measures during practice.
The data were analyzed using SPSS statistical software (Version 25). The four-degree values (never, scarcely, sometimes, always) were scored from 0 to 3. All scores were converted to percentages (sum of score/ maximum score) *100). To focus more on the knowledge, attitudes and practice, the scores of participants were categorized as follow: scores below 50 were labeled as poor, negative, or high risk; scores between 50 and 75 were labeled as moderate; scores above 75 were considered as excellent, positive or low risk [23]. Descriptive statistics, including frequencies, percentages, and univariate analysis (Chi-square), were used to find the relationship between the student's demographics (gender and discipline) and student's knowledge, attitudes and practice. All tests were performed at a significant level of P ≤ 0.05.
3. RESULTS
This study includes a total of 182 complete and valid responses. Table 1 shows the socio-demographic characteristics of the participants. The average age of the participants was 22 years old. Of the total study sample, two-thirds of the participants were female (72.4%), while 27.6% were male.
Table 2 displays the status of students related to exposure to infected patients. The majority of the students believe that dental clinics are more prone to infectious diseases than other medical fields (91.2%). More than half of the students showed a positive attitude toward treating patients with infectious diseases (61.5%).
| - | Dental Students | Dental Technology Students | Dental Hygeine Students | |
|---|---|---|---|---|
| Gender | Male | 29 (31.2) | 18 (26.1) | 3 (16.7) |
| Female | 64 (68.8) | 51 (73.9) | 15 (83.3) | |
| Age | 21 | 34 (41.0) | 38 (45.8) | 11(13.3) |
| 22 | 40 (63.5) | 20 (31.7) | 3 (4.8) | |
| ≥ 23 | 19 (54.3) | 12 (34.3) | 4 (11.4) | |
| Question |
Total n (%) |
Dental Students n (%) |
Dental Technology Students n (%) |
Dental Hygiene Students n (%) |
P-value |
|---|---|---|---|---|---|
| Are dental clinics more prone to infectious diseases than other medical fields | 0.004* | ||||
| Yes | 166 (91.2) | 91 (55.2) | 58 (35.2) | 16 (9.6) | |
| No | 16 (8.8) | 2 (12.5) | 12 (75.0) | 2 (12.5) | |
| Will you treat patients with infectious or take impression? | |||||
| Yes | 121 (61.5) | 60 (54.1) | 41 (36.9) | 10 (9.0) | 0.645 |
| No | 70 (38.5) | 33 (47.1) | 29 (41.4) | 8 (11.4) | |
| Number of infectious patients or impressions have been treated | 0.226 | ||||
| 0 | 124(68.1) | 71(56.8) | 43 (34.4) | 11 (8.8) | |
| 5 | 53(29.1) | 21(41.2) | 24 (47.1) | 6 (11.8) | |
| >5 | 5(2.7) | 1(20.0) | 3 (60.0) | 1 (20.0) | |
| Type of infectious disease have you treated | 0.189 | ||||
| Nil | 124 (68.1) | 71 (56.8) | 43 (34.4) | 11 (8.8) | |
| Hepatitis B | 24 (13.2) | 10 (43.5) | 11 (47.8) | 2 (8.7) | |
| Others | 34 (18.7) | 12 (35.3) | 17 (50.0) | 5 (14.7) | |
| Do you know how to treat patients or deal with impressions from patients with infectious diseases? | 0.065 | ||||
| Yes | 58 (31.9) | 22 (38.6) | 28 (49.1) | 7 (12.3) | |
| No | 124 (68.1) | 71 (57.3) | 42 (33.9) | 11 (8.9) | |
The majority of the students reported that the weight of cross-infection topics in the curriculum and corresponding weight of marks in the examination should be increased (80% and 71.7%, respectively) (Table 4).
| Variables |
Total n (%) ** |
Dental Students n (%) |
Dental Technology Students n (%) |
Dental Hygiene Students n (%) |
P-value | ||
|---|---|---|---|---|---|---|---|
| Facial mask | 0.000* | ||||||
| Always | 119(65.4) | 79(66.9) | 24(20.3) | 15 (12.7) | |||
| Sometime | 48(26.4) | 7(14.6) | 39(81.3) | 2 (4.2) | |||
| Rarely | 6(3.3) | 3(50.0) | 3(50.0) | 0 (0.0) | |||
| never | 9(4.9) | 4(44.4) | 4(44.4) | 1 (11.1) | |||
| Gloves | 0.000* | ||||||
| Always | 134(73.6) | 87(65.4) | 31(23.3) | 15(11.3) | |||
| Sometime | 41(22.5) | 4(9.8) | 34(82.9) | 3(7.3) | |||
| Rarely | 6(3.3) | 2(33.3) | 4(66.7) | 0(0.0) | |||
| Never | 1(0.5) | 0(0.0) | 1(100.0) | 0(0.0) | |||
| Head cap | 0.011* | ||||||
| Always | 27(14.8) | 10(38.5) | 11(42.3) | 5(19.2) | |||
| Sometime | 43(23.6) | 15(34.9) | 26(60.5) | 2(4.7) | |||
| Rarely | 35(19.2) | 21(60.0) | 10(28.6) | 4(11.4) | |||
| Never | 77(42.3) | 47(61.0) | 23(29.9) | 7(9.1) | |||
| Gowns | 0.008* | ||||||
| Always | 35(19.2) | 11(32.4) | 16(47.1) | 7(20.6) | |||
| Sometime | 54(29.7) | 23(42.6) | 28(51.9) | 3(5.6) | |||
| Rarely | 37(20.3) | 22(59.5) | 12(32.4) | 3(8.1) | |||
| Never | 56(30.8) | 37(66.1) | 14(25.0) | 5(8.9) | |||
| Removing gloves/mask while walking around in the clinic | 0.030* | ||||||
| Always | 75(41.2) | 43(58.1) | 19(25.7 | 12(16.2) | |||
| Sometime | 83(45.6) | 41(49.4) | 37(44.6) | 5(6.0) | |||
| Rarely | 12(6.6) | 5(41.7) | 6(50.0) | 1(8.3) | |||
| Never | 12(6.6) | 4(33.3) | 8(66.7) | 0(0.0) | |||
| Changing gloves in each procedure | 0.322 | ||||||
| Always | 124(68.1) | 68(55.3) | 42(34.1) | 13(10.6) | |||
| Sometime | 45(24.7) | 22(48.9) | 19(42.2) | 4(8.9) | |||
| Rarely | 1(0.5) | 0(0.0) | 1(100.0) | 0(0.0) | |||
| Never | 12(6.6) | 3(25.0) | 8(66.7) | 1(8.3) | |||
| Changing gloves from one patient to another | 0.000* | ||||||
| Always | 155(85.2) | 91(59.1) | 48(31.2) | 15(9.7) | |||
| Sometime | 13(7.1) | 0(0.0) | 7(87.5) | 1(12.5) | |||
| Rarely | 6(3.3) | 1(16.7) | 5(83.3) | 0(0.0) | |||
| Never | 8(4.4) | 1(7.7) | 10(76.9) | 2(15.4) | |||
| Washing hand after every procedure | 0.784 | ||||||
| Always | 136(74.7) | 72(53.3) | 51(37.8) | 12(8.9) | |||
| Sometime | 40(22.0) | 18(45.0) | 16(40.0) | 6(15.0) | |||
| Rarely | 3(1.6) | 1(33.3) | 2(66.7) | 0(0.0) | |||
| Never | 3(1.6) | 2(66.7) | 1(33.3) | 0(0.0) | |||
| Changing gown if it is contaminated | 0.016* | ||||||
| Always | 112(61.5) | 64(57.7) | 36(32.4) | 11(9.9) | |||
| Sometime | 31(17.0) | 8(25.8) | 18(58.1) | 5(16.1) | |||
| Rarely | 19(10.4) | 7(36.8) | 10(52.6) | 2(10.5) | |||
| Never | 20(11.0) | 14(70.0) | 6(30.0) | 0(0.0) | |||
| Washing lab coat every week | 0.560 | ||||||
| Always | 135(74.2) | 75(56.0) | 47(35.1) | 12(9.0) | |||
| Sometime | 38(20.9) | 14(36.8) | 19(50.0) | 5(13.2) | |||
| Rarely | 7(3.8) | 3(42.9) | 3(42.9) | 1(14.3) | |||
| Never | 2(1.1) | 1(50.0) | 1(50.0) | 0(0.0) | |||
| Adding disinfectant to the slurry of pumice or dental stone | 0.035* | ||||||
| Yes | 128(70.3) | 71(55.5) | 42(32.8) | 15(11.7) | |||
| No | 54(29.7) | 22(41.5) | 28(52.8) | 3(5.7) | |||
| Do you aware of infection control measures that should be taken in to practice | 0.067 | ||||||
| Yes | 161(88.5) | 85(53.1) | 62(38.8) | 13(8.1) | |||
| No | 21(11.5) | 8(38.1) | 8(38.1) | 5(23.8) | |||
| Education and Curriculum | Total n (%)* |
Dental Students n (%) |
Dental Technology Students n (%) |
Dental Hygiene Students n (%) |
p-value* | |
|---|---|---|---|---|---|---|
| Are dental schools responsible for implementation of infection control | Yes | 158(90.8) | 83(52.9) | 57(36.3) | 17(10.8) | 0.290 |
| No | 16(9.2) | 6(37.5) | 9(56.3) | 1(6.3) | ||
| Have you studied infection control within your curriculum? | Yes | 152(86.9) | 84(55.3) | 51(33.6) | 17(11.2) | 0.007* |
| No | 23(13.1) | 6(27.3) | 15(68.2) | 1(4.5) | ||
| Do you have questions about infection control among your written exams? | Yes | 127(72.6) | 69(54.8) | 40(31.7) | 17(13.5) | 0.007* |
| No | 48(27.4) | 21(43.8) | 26(54.2) | 1(2.1) | ||
| Do you have questions about infection control among your practical exams? | Yes | 126(72.0) | 73(58.4) | 36(28.8) | 16(12.8) | 0.000* |
| No | 49(28.0) | 17(34.7) | 30(61.2) | 2(4.1) | ||
| Do you have textbooks about infection control? | Yes | 93(53.1) | 51(55.4) | 27(29.3) | 14(15.2) | 0.002* |
| No | 82(46.9) | 39(47.6) | 39(47.6) | 4(4.9) | ||
| Do you think dental school teaches you enough information about infection control? | Yes | 118(67.4) | 73(62.4) | 29(24.8) | 15(12.8) | 0.000* |
| No | 57(32.6) | 17(29.8) | 37(64.9) | 3(5.3) | ||
| Do you think more weight for infection control topic in curriculum should be increased? | Yes | 140(80.0) | 66(47.5) | 59(42.4) | 14(10.1) | 0.046* |
| No | 35(20.0) | 24(68.6) | 7(20.0) | 4(11.4) | ||
| Do you think the weight of marks in examination for infection control topic should be increased? | Yes | 124 (71.7) | 53(43.1) | 55(44.7) | 15(12.2) | 0.002* |
| No | 49(28.3) | 36(73.5) | 10(20.4) | 3(6.1) | ||
However, more than two-thirds of the students that participated in the study (68.1%) had no experience of treating infected patients or handling an impression for infected patients. Moreover, the results indicated that there was a significant difference between students' opinions referred to their discipline about considering dental clinics more prone to infectious disease when compared to other medical fields.
Table 3 illustrates the compliance with the use of protective barriers to prevent direct contact with patients and prevent transmission of infections. Regardless of the students' discipline, most of the students adhered to use both facial masks and gloves (65.4% and 73.6%, respectively). On the other hand, compliance with the use of head caps or gowns was low (14.8% and 19.2%, respectively).
Regarding the importance of cross-infection education, most students agreed that dental schools are responsible for delivering infection control knowledge (90.8%). Though, 86.9% of participants reported that they had studied infection control during their study years (Table 4).
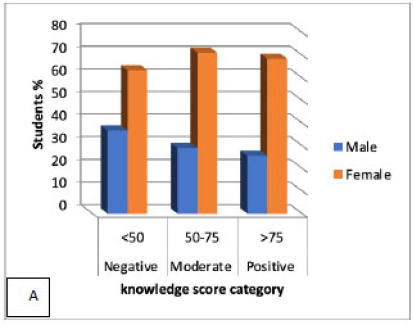
From the results obtained, it was noted that most students had either moderate (58.8%) or excellent knowledge (30.8%) regarding infection control. Less than half of the students had moderate attitudes towards implementing infection control measures (44.5%). In addition, most students had either moderate (44.5%) or low-risk practice (47.8%) regarding infection control (Table 5).
The distribution of knowledge and attitude scores according to gender and discipline were shown in Figs. (1 and 2), respectively. The Chi-Square Goodness of Fit Test indicated that the gender group and discipline group were similarly distributed among the knowledge and attitude score category (p-value > 0.05) as shown in Figs. (1 and 2).

| The categories of the participant's KAP | N | % |
|---|---|---|
| Knowledge score (76.09±19.69) * | ||
| Poor <50 | 6 | 3.3 |
| Moderate 50-75 | 98 | 53.8 |
| Excellent >75 | 78 | 42.9 |
| Attitudes and Practice score (71.79±11.63) * | ||
| Negative <50 | 12 | 6.6 |
| Moderate 50-75 | 47 | 25.8 |
| Positive >75 | 123 | 67.6 |
4. DISCUSSION
Dental team members are more exposed to cross-contamination than the general population [24]. Dental students are the future dental professionals who will be potentially exposed to contagious diseases and are responsible for employing infection control strategies taught in dental schools. Hence, they should be well educated and trained to possess the necessary level of knowledge and implement optimal adherence to infection control measures [22].
Up to our knowledge, this is the first study in Jordan conducted to assess the knowledge, attitude, and practice of infection control among dental, dental technology, and dental hygiene students, and to highlight the importance of university curriculum on the students’ attitude in this regard. A previous study in Jordan investigated the knowledge and practice of infection control, but the targeted participants were the senior dentists and dental nurses [16]. More previous studies investigated the knowledge and attitude, and awareness toward cross-infection among dental teams worldwide [7, 12]. It is worth noting that most of the research in literature was among dentists, but fewer studies focused on other dental team members like dental technicians and dental hygienists.
The majority of the students believe that a dental clinic is a high-risk place for the transmission of infectious diseases compared to other medical fields. This finding agrees with the previous studies, which found that the vast majority of dental students had similar perceptions [15, 22].
The results of the present survey regarding HBV immunization revealed that two-thirds of the participants had taken HBV vaccination. One-third of participants were found to be non-vaccinated, which may indicate inadequate enforcement and lack of strict compliance by the dental school. The immunization rate in the current study was lower than that reported by other studies in dental schools of other countries. A higher percentage ranging from 90-100% of dental students immunized against HBV was reported [13, 15, 25-27].
Most of the participants showed good compliance regarding the use of gloves and facial masks. These findings disagree with a previous study in Jordan that reported that only 43% of dental staff and 30% of dental assistants wore masks routinely; however, 100% of participants used gloves,16.. The current study findings agreed with another study that indicated that 81% of dentists wore gloves, but only 54% wore masks routinely in private clinics setting [28]. Higher compliance towards wearing gloves (99.2%) and mask (98.3%) was reported among students at Sharjah University in UAE [15].
In our study, half of the dental students remove gloves and masks when walking around the clinic. Significantly more dental students change gloves between patients compared to dental technology students. This can be explained by the fact that dental technology students are not involved directly with patients. These findings concur with a previous report in Jordan, where (96%) of practicing dentists were found compliant to change gloves compared to only (29%) of dental assistants [16]. However, a higher degree of compliance was previously reported by dental students (99.6%) [29]. The reason behind such findings could be partly related to the greater weight dedicated to infection control in the curriculum for dental students compared to the dental technology and dental hygiene curriculum at JUST. Furthermore, apparently, clinical instructors demonstrate more commitment towards enforcing compliance with personal protective measures by dental students in a clinical setting more than with other dental team members. Less emphasis seemingly had been placed on these measures’ implementation by dental assistants and dental technicians.
The significant difference between dental, dental technology, and dental hygiene students who suffered from accidental injuries may be explained by the higher risk for dental technicians due to wide exposure to sharp equipment and instruments compared to dental and dental hygiene students. 82% of accidental injuries have been previously reported among dental technology students, 28., whereas another study reported only 31% accidental injuries [13]. In the current survey, 52.6% of accidental injuries were reported. If instruments and equipment are non-sterilized, a remarkable risk of transmission of bloodborne pathogens such as HBV, HIV exists [26]. However, for the needle injuries, dental students recorded a higher percentage (66.7%) than dental technology students (15.4%) due to higher usage in the clinic.
There was a significant correlation between knowledge and practice (P=0.003), attitude, and practice (p=0.008). This partially agreed with a previous study that found a correlation between attitude and practice, but no correlation was found between the level of knowledge and practice [19]. The results reaffirmed the importance of good knowledge and a positive attitude to ensure better compliance with infection control measures.
The majority of students believed that dental school is responsible for the implementation of infection control with no significant differences between the groups, which confirmed an overall agreement on this issue. Dental school is required to focus further on infection control teaching in the curriculum, and it has the authority to enforce the recommended infection control strategies and practices. Continuous improvement can also be enhanced through periodic reviews of feedback from students and patients.
About 73% of participants believed that a proper weight of grades was assigned to cross infection control-related topics in the examinations. However, only 31.7% of dental technology students were satisfied with the weight given to cross infection control topics in the examinations. A previous report in Saudi Arabia concluded that most of the subjects responded positively to only a few lectures during the undergraduate program about cross infection control [5]. In the current study, most of the participants reported positive responses when asked if the cross-infection control is covered in the curriculum though they stated that the weight of this topic is not adequate and should be increased.
CONCLUSION
A good to moderate knowledge among dental, dental technology, and dental hygienist students about infection control principles and guidelines were found. However, moderate compliance in applying the measures to prevent cross-infection was reported. A significant difference exists among the participants, where dental and dental hygiene students demonstrated positive adherence to infection control guidelines. However, dental technology students showed less compliance and adherence to infection control guidelines. There was an obvious need to improve the university curriculum, particularly for the dental technology discipline, to increase the knowledge and awareness of infection control procedures and reduce the risk of spreading diseases.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the Jordan University of Science and Technology (JUST) Institutional Review Board, Jordan, with protocol number 2017/0032). Participation in the study was consensual.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in full accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the World Medical Association Declaration of Helsinki of 1975, as revised in 2008.
CONSENT FOR PUBLICATION
The return of completed questionnaires was taken as a proxy for consent to participate in the study.
AVAILABILITY OF DATA AND MATERIALS
The datasets generated during and analyzed during the current study are not publicly available to avoid violating the privacy of research participants. However, they would be made available from the corresponding author, SA., on reasonable request.
FUNDING
This study was funded by the Deanship of Research, Jordan University of Science and Technology, grant number (0032).
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We acknowledge the research deanship at JUST for funding the study.

