All published articles of this journal are available on ScienceDirect.

Assessment of Degree of Conversion and Knoop Microhardness of Different Resin Cementing Agents
Authors Info & Affiliations
Abstract
Background:
There are still controversies in the literature as to which is the best resinous cementing agent. Due to this fact and the immense availability of types and brands of cementing agents, further studies are needed to evaluate the properties of these important dental materials.
Objective:
To assess the degree of monomer conversion (DC) and Knoop microhardness (KHN) of four resin cements: two conventional dual-cured resin cements (EnForce and RelyXARC); one self-etching cement (RelyXU100); and one chemically-activated cement (Cement-Post).
Methods:
20 Pieces were made to assess KHN, and 20 to assess DC (n = 5). The DC was analyzed using a Fourier-transform infrared spectrometer, and KHN of the base and the top of the pieces were assessed using the Future-Tech microhardness tester. The data of KHN were statistically analyzed by two-factor ANOVA, and data related to DC were analyzed by the Kruskal-Wallis non-parametric test. The analysis of the correlation between KHN and DC of the cementing agents was performed by linear regression.
Results:
Dual-cured cements exhibited lower average KHN values at the base than at the top of the pieces (p <0.05). The self-etching cement had a significantly higher average KHN value than the other assessed cements (p <0.05). The DC of the dual-cured cement did not differ (p >0.05). The chemically-activated cement exhibited the lowest averages of KHN and DC values (p <0.05). Linear regression analysis indicated a strong correlation between DC and KNH (p = 0.043; R2 = 0.96); however, a specific hardness value could not be correlated to a specific DC value.
Conclusion:
Preferably, dual-cured resin cements (conventional or self-etching) should be used. Chemically-activated resin cements should be avoided due to their lower averages of DC and KHN values.
1. INTRODUCTION
Resin cements are polymeric materials commonly used in the cementation of indirect restorations due to their high aesthetics, low solubility, high adhesive strength, and superior mechanical properties that help reinforce restorations [1-5]. However, resin cements are sensitive to the technique. This way, problems occurring during cementation are one of the main causes of failure in indirect adhesive aesthetic restorations [6-8]. Different resin cements can be used in diverse clinical situations. It is worth mentioning that the variations between these materials occur mainly during the polymerization and bonding mechanism [2, 3].
Resin cements can be classified according to their activation modes, namely: chemically activated; photo-activated (physical activation); and dual-cured [6, 9]. In dual activation, the polymerization reaction is initiated both by the emission of visible light and by a chemical reaction (peroxide/amine) [2, 9]. This category reconciles the advantages of photo-activated cements, such as control of working time and color stability, with the possibility of achieving an adequate degree of monomer conversion (DC), regardless of the presence of light, the main advantage of chemically-activated cements [2, 5, 10].
Another classification has become mandatory since the advent of new resin cements with different bonding mechanisms [2]. This way, cements can also be classified as conventional or self-etching cements [3, 6]. Conventional cements require previous acid etching and hybridization with the adhesive system, so that the union between the resinous material and the dental structure occurs [3, 5, 6]. Self-etchers do not require previous acid conditioning with the adhesive system, reducing the sensitivity inherent to the cementation technique by simplifying the procedure and, consequently, optimizing clinical time [2, 6].
Despite the clinical advantages of self-etching resin cements, some studies have indicated that conventional resin cements exhibited higher DC and better mechanical properties [3, 4, 6]. In this sense, doubts still arise regarding the use of conventional or self-etching resin cements. Due to this fact and the immense availability of types and brands of cementing agents, the goal of the present study was to assess Knoop microhardness (KHN) and the DC of four commercial resin cements. The tested null hypothesis was that there was no significant difference in KHN and DC of the cementing agents assessed.
2. MATERIALS AND METHODS
Four A2-shade resin cements were used: two conventional dual-cured cements; one dual-cured self-etching cement; and one conventional chemically-activated cement (Table 1).
2.1. Knoop Microhardness
Twenty pieces were made in a circular black Teflon matrix (diameter = 4 mm; height = 2 mm). They were randomly distributed into four groups (n = 5), according to the selected resin cementing agents. The cements were inserted with single increments in the matrix, between polyester strips and glass coverslips. Photo-activation was performed by a Light Emitting Diode (LED) (Elipar Freelight 2, 3M ESPE, USA), with irradiance of 800 mW2 for 20 seconds. Prior to making the test pieces for each experimental group, the photo-activation unit was measured by a radiometer (LED Radiometer, Kerr, USA). The groups made with chemical setting cement were not submitted to light irradiation, and were kept between the polyester strips and the glass coverslips for four minutes.
Subsequently, they were stored in a biological oven at 37 ºC ± 1 and 100% humidity for 24 hours. Prior to carrying out the microhardness tests, the pieces were polished using a polishing machine (DPU-10, Struers, Copenhagen, Denmark) with paper #1200. The hardness measurements were obtained using the Future Tech 700 microdurometer (Future-Tech Corp., Kawasaki, Japan), with a load of 50 grams-force (gf) for 30 seconds, at five equidistant points on the base and top surfaces, totaling ten measurements per piece. The average hardness values of the bases and the tops, and the general average were calculated for each piece.
2.2. Degree of Monomer Conversion
Twenty pieces were made in a Teflon bipartite circular matrix (diameter = 8mm; height = 2mm), and randomly distributed into four groups (n = 5), according to the resin cementing agents selected. The protocols for the preparation of the pieces and storage conditions were the same used for the KHN tests.
The base of each piece was eroded in order to obtain 1.5 to 2.0 mg of powder and taken to the Nicolet iS10 Fourier Transform spectrophotometer (Thermo Scientific/Waltham, MA, USA). All spectra were obtained between the 4000 and 750 cm-1 bands, with a resolution of 4 cm-1. The spectra of each sample were transferred to the Origin software (OriginLab Corp., Northampton, MA, USA). The vibrational modes between 1500 and 1700 cm-1 were selected for obtaining better visualization. The absorbance spectrum was acquired by scanning the pieces 32 times, at intervals of 1670 to 1550 cm-1. The calculation of the DC was based on the proportion between the absorbance values at 1638 cm-1, representing the absorption of the double bond of aliphatic carbon of vinyl methacrylate, and at 1608 cm-1, corresponding to the absorption of the double bond of aromatic carbon that remains constant during the polymerization reaction. These values were entered in the equation:
DC% = 100 [1- (Rpolymer/Rmonomer)]
where Rpolymer = peaks at 1638 cm-1, and Rmonomer = peaks at 1608 cm-1.
| Trade Name (Manufacturer) | Activation Mode | Method of Union | Composition | Batch |
|---|---|---|---|---|
| EnForce (Dentsply Caulk, York, EUA) |
Dual | Conventional | Base: Bis-GMA, TEGDMA, CQ, EDAB, BHT and DHEPT. Catalyst: Bis-GMA, BHT, EDAB, TEGDMA and BPO. | 103515B |
| RelyX ARC (3M ESPE, Sant. Paul, EUA) |
Dual | Conventional | Paste A: Bis-GMA, TEGDMA, dimethacrylate polymer, CQ, amine. Paste B: Bis-GMA, TEGDMA, dimethacrylate polymer, BPO. | N179452 |
| RelyX U100 (3M ESPE, Seefeld, Germany) |
Dual | Self-etching | Base: Glass Powder, methacrylated phosphoric acid esters, thriethylene glycol dimethacrylates, silane treade sílica, sodium persulfate. Catalyst: Glass Powder, substituted dimethacrylate, silane treated silica, sodium p-toluenesulfinate, calcium hydroxide. | 411674 |
| Cement-Post (Angelus, Londrina, Brazil) |
Chemistry | Conventional | Base: Bis-GMA, TEGDMA, barium glass ceramics, pyrogenic silica, tertiary amine, antioxidant, pigments. Catalyst: Bis-GMA, TEGDMA barium glass ceramics, pyrogenic silica, activator, stabilizer. | 15876 |
2.3. Statistical Analysis
Data relating to KHN and DC were submitted to the Shapiro-Wilk test and Levene’s test to determine the parametric assumptions of normality and homoscedasticity. Subsequently, the data of KHN were statistically analyzed by two-factor ANOVA and post-hoc Tukey's test. Data relating to DC were analyzed by the Kruskal-Wallis non-parametric test and post-hoc Dwass-Steel-Critchlow-Fligner test. The analysis of the correlation between KHN and DC of the cementing agents was performed by linear regression with the results of the base of the pieces. Statistical calculations were performed using the Jamovi software (version 2.22), with a significance level of 5%.
| Resin Cementing Agents | Average Top (SD) | Average Base (SD) |
|---|---|---|
| EnForce | 55.5 (3.88)ad | 40,6 (2.72)b |
| RelyX ARC | 49.3 (4.42)a | 42,4 (0.67)b |
| RelyX U100 | 61.8 (4.78)c | 49,1 (2.90)d |
| Cement-Post | 26.8 (1.75)e | 23,9 (1.76)e |
3. RESULTS
3.1. Knoop Microhardness
The two-way ANOVA test indicated that the average KHN values were influenced by the different types of resin cements assessed and by the measures taken from the top or base of the pieces (p <0.001). The cements obtained significantly lower average KHN values at the base than at the top of the pieces (p <0.05), except for Cement-Post (p = 0.83). RelyX U100 had the highest KHN average values (p <0.05), followed by EnForce and RelyX ARC, which did not differ statistically from each other. Cement-Post had the lowest average KHN value (p <0.001) (Table 2).
3.2. Degree of Monomer Conversion
The Kruskal-Wallis test indicated a statistical difference between the DC of the resin cements assessed (p = 0.014) (Table 3). The post-hoc test revealed that EnForce, RelyX ARC, and RelyX U100 did not differ statistically from each other (p >0.05). However, only RelyX ARC and RelyX U100 exhibited a statistically significant difference from Cement-Post, the cement with the lowest DC values.
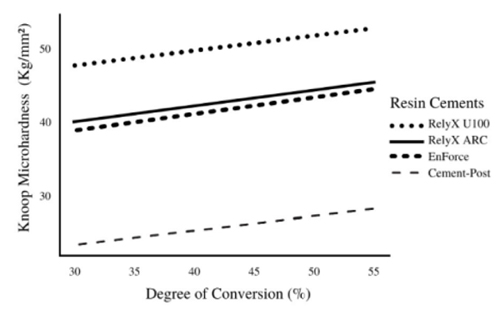
3.3. Correlation Between Degree of Monomer Conversion and Knoop Microhardness
The linear regression analysis indicated a strong positive correlation between DC and KNH (p = 0.043). The higher the DC, the greater the KNH of resin cements (Fig. 1). The DC of the assessed cements (R2 = 0.96) can explain 96% of microhardness variability. This correlation was different between the cementing agents, i.e., a specific value of DC was not able to predict KNH if the resin cements being assessed were not specified.
| Resin Cementing Agents | Median (IQR) |
|---|---|
| EnForce | 35.5 (4.14)ab |
| RelyX ARC | 42.7 (3.13)a |
| RelyX U100 | 38.2 (2.83)a |
| Cement-Post | 34.3 (1.74)b |
4. DISCUSSION
The DC of resin cementing agents is directly proportional to the magnitude of adhesion between the resin material and the dental structure, influencing the physical properties and satisfactory clinical performance of resin cements in indirect procedures [3, 4, 8]. In addition to decreasing bond strength, low DC can lead to pulp sensitivity, decrease in mechanical characteristics, and compromise the clinical success and longevity of the restoration due to detachment, fracture, or secondary caries [2-7]. There are several factors that can interfere with the DC of resin cements, for example, the composition of the materials, possible interactions between the adhesive system and the cements, characteristics of the restorations to be cemented, and characteristics of the photo-activation stage [4-9].
Some laboratory studies claim that conventional resin cementing agents have higher DC and better mechanical properties. On the other hand, other studies have indicated that self-etching cements were superior, or that there was no difference between them [3, 4, 6]. A systematic review carried out recently with laboratory studies concluded that conventional cement tended to promote greater resistance of immediate and long-term adhesion to dentin [3]. However, when considering the cementation of fiberglass posts in the root canals, self-etching resin cements performed better than conventional cements [3, 6]. In the present study, the self-etching resin cement RelyX U100 exhibited the highest KNH values, but did not differ statistically from conventional cements with respect to DC.
RelyX ARC and EnForce are conventional resin cements that have double polymerization. They did not exhibit statistical differences between them, both for the DC and KHN average values, confirming the results of previous studies that the two cements had not exhibited significant differences in their mechanical properties [10, 11]. These cements have the same polymerization mechanism and the same classification regarding the bonding mechanism. However, there are reports of studies that found DC values of RelyX ARC significantly higher than those of EnForce, probably explained by differences in the methods employed [8, 12].
The results of the present study confirmed the statement that there is a strong positive correlation between the DC and KHN, i.e., microhardness values increase as DC values increase [10, 13]. The DC was able to predict 96% of the variability of KNH in the cementing agents included in the study (p <0.05). However, KHN can be sensitive to different variables [10, 13], and a specific hardness value cannot be correlated to a specific DC when comparing different material formulations. Therefore, the two techniques should not be used interchangeably as indicative of DC of different resins since each one is sensitive to different variables. The same DC for EnForce and RelyX U100 does not mean the same KHN; however, if the DC is increased, higher KNH values will be obtained for both cements.
Cement-Post had the lowest results when compared to the other assessed cements (p <0.01). This result can be attributed to the inhibition of oxygen and the increase of the inhibitor in the formulation of chemical cure cements, used to increase the working time of this material [7, 9, 14]. Therefore, the use of dual-cure cement should always be considered for possibly increasing DC through physical and chemical activation of the monomer system [3, 5, 9]. Despite the lower results, Cement-Post was the only cement that did not show statistical differences between the KNH results at the top and base of the pieces, which can be explained by its exclusively chemical activation that occurs without depending on the irradiance of light.
The difference between the results of the top and base of the pieces indicated by KNH tests demonstrated that the chemical polymerization of the dual-cure cements was not sufficient to achieve the same results obtained in regions closer to the photo-activator unit. These results are in line with those of other studies regarding the fact that polymerization of dual-cure cements depends on photo-activation for achieving higher hardness values [7, 9, 10]. However, it has been suggested in the literature that a composite is properly polymerized when the maximum hardness of the lower surface of a sample is above 80% of that measured on the upper surface [15, 16].
RelyX ARC, RelyX U100, and EnForce achieved, respectively, 86, 79.44, and 73.15% of hardness in the base with respect to the top of the pieces. Considering the aforementioned authors' suggestion, only EnForce was far from the recommended hardness values. It is known that the intensity of light reaching the cements is drastically reduced when transmitted through a composite or ceramic restoration [2-4]. Laboratory studies have evidenced that the activation time generally recommended by the manufacturers was not enough to result in maximum DC [10, 15]. Therefore, a prolonged photo-activation time can be an option to improve the level of polymerization of dual-cure resin cements [3, 5].
The results of laboratory studies are an important factor to be considered in the prognosis of the longevity of restorations. However, other aspects should also be taken into consideration, given that the clinical success of indirect restorations is not attributed only to resin cements. Ensuring a high DC is fundamental to obtain the best chemical and physical properties of resin cements, in addition to being a critical factor of biocompatibility [5, 7]. The null hypothesis of the present study was rejected, since the cementing agents tested showed significant differences in KHN and DC.
CONCLUSION
Based on the results obtained and within the limitations of the present in vitro study, we suggest that chemically-activated resin cements should be avoided due to their lower averages of DC and KHN values. Preferably, dual-cure resin cements should be used. Although the self-etching cement assessed exhibited the highest KHN results, the dual-cure resin cements (conventional or self-etching) did not differ among them with respect to the DC. Further conclusive evidence derived from clinical observations is needed to confirm the findings of the present study.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in Zenodo Repository the at: https://zenodo.org/, reference number 10.5281/zenodo.5610313.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

