All published articles of this journal are available on ScienceDirect.

The Application of Pendulum as a Space Regainer in Orthodontic Treatment
Abstract
Background:
The process of distalization in orthodontic treatment is often very difficult. The most common method is the use of cervical headgear. However, due to poor patient compliance, it leads to poor treatment outcomes. Treatment alternatives that require minimal compliance include Jones jig, magnets, and pendulum.
Objective:
This study aimed to perform distalization of a maxillary molars on a bilateral Class II molar relationship patient with a crowded maxillary arch.
Case Report:
A 10-year-old female with a Class II molar relationship, bilateral posterior crossbite, and nonerupted upper canines was treated with a rapid palatal expander (RPE), pendulum appliance, and fixed appliance. The crowding in the maxillary arch and spacing in the mandibular arch were eliminated, and transverse discrepancies were corrected.
Conclusion:
Pendulum appliance is very effective in creating spaces for the eruption of canines and ectopic premolars. Pendulum appliances have been introduced for a long time and have proven successful for molar distalization and space regainer and require minimal patient cooperation. Like other distalization appliances, distal tipping of the molars and mesial movement of the premolars could be observed.
1. INTRODUCTION
Molar distalization is a procedure of increasing the arch length by the rear movement of the molar [1, 2]. During orthodontic treatment, the process of distalization, especially for the upper molar teeth, is challenging. Headgear is one of the most common methods to achieve distalization and has been used for a long time [3]. However, headgear depends mainly on patient compliance. Many patients are embarrassed with wearing an extraoral appliance, which led to the preference for intraoral distalizing appliances [4]. Currently, there are many different types of intraoral distalizing appliances, including Jones jig, magnets, distal jets, and pendulum. Each has its own indication and contraindication on when to use the particular appliance and also has its own mechanics. Different practitioners usually have their own personal preferences on which intraoral distalizing appliance to use.
1.1. Pendulum Orthodontic Appliance
The pendulum appliance was first created by Dr. Hilger in 1992 [5]. Many practitioners have used this appliance and achieved successful results. The pendulum appliance is usually used in a Class II case. One advantage of the pendulum appliance is to correct unilateral asymmetry molar relationships (Fig. 1) [6].
The pendulum appliance is also useful in creating spaces for the upper premolars and/or canines that do not have enough space for eruption by distalizing the upper first molar. Therefore, the best time to use a pendulum is before the eruption of the second permanent molar to maximize the efficiency of distalization. However, the pendulum could also be used in distalizing both the first and second molar. Another advantage of the pendulum appliance is controlling the molar and preventing it from tipping distally [7-10].

1.2. Design of Pendulum Appliance
The pendulum appliance is consisted of an acrylic Nance with two pairs of right and left wires for additional retention on the premolar teeth. One pair of Titanium-Molybdenum alloy (TMA) wires with coil spring are placed into the lingual sheath of the molar to be distalized. For premolar retention, a wire is usually attached using a composite to the occlusal surface of the premolar (Fig. 2). Another option is to solder an arm to a premolar band.
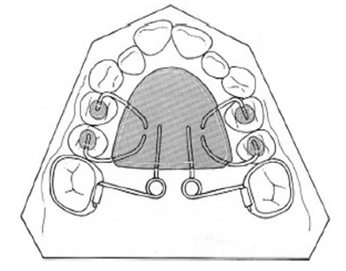
The wires of the pendulum are made parallel with the palatal midline, with a force strength of 230-250 grams [3].
2. CASE REPORT
2.1. History
A 10-year-old female patient was presented to the office with the chief complaint of fixing the bite because of spaces between teeth. The patient was not taking any medications and had no known drug allergies or acknowledge habits. She did not have temporomandibular joint symptoms, but she and her parents noticed dental crossbite.
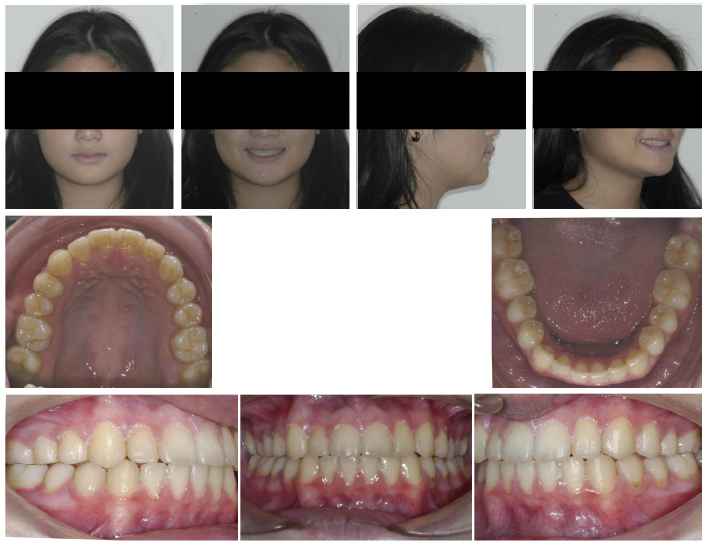
2.2. Assessment
Facial examination showed a straight, slightly concave profile of the patient (Fig. 3). The patient had a Class I skeletal relationship (Fig. 4). Intraoral examination revealed that the patient was in the late mixed dentition stage, with maxillary crowding and moderate spacing in the mandibular arch (Fig. 3). It was observed that patient had an edge-to-edge anterior bite, Class II molar relationship with a bilateral posterior crossbite, and nonerupted upper canines (Figs. 3 and 4). Furthermore, the patient had good oral hygiene and no dental cavities. The panoramic radiograph (Fig. 4) demonstrated late mixed dentition, including a lack of space for the eruption of both maxillary canines.


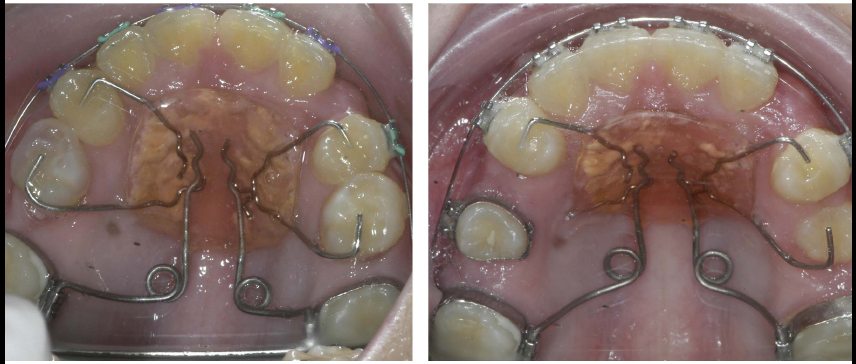
2.3. Treatment Objectives and Treatment Progress
The treatment objectives were to expand the maxillary arch, coordinate arches, eliminate the posterior crossbite, and establish a Class I molar and canine relationship. Treatment was started by bonding metal 0.022-in slot pre-adjusted edgewise appliances with a rapid palatal expander (RPE) to correct the posterior crossbite. Instruction was given to the patient and parents to do one turn per day of the expansion screw for 14 days. The RPE was removed after a five-month retention phase. A pendulum appliance was then delivered to start the distalization process. After eight months, enough space was created for both maxillary canines, and a Class I molar relationship was achieved (Figs. 5 and 6). Detailing was performed using 0.017 x 0.025 titanium molybdenum alloy (TMA) archwire. Upon completion of treatment, maxillary and mandibular Hawley retainers were delivered, and the patient was instructed to wear the retainer for 24 hours per day (Figs. 7 and 8).

3. RESULTS
The patient’s chief complaint was addressed. Acceptable esthetic and functional results were achieved. The crowding in the maxillary arch and spacing in the mandibular arch were eliminated, and transverse discrepancies were corrected.
4. DISCUSSION
In cases of Class II malocclusions, bilateral or unilateral Class II molar relationships, and ectopic eruption of canines and/or premolars, treatment options include headgear, distal jet, Jones jig, magnetic repelling, and pendulum. However, noncompliance tends to be one of the most common reasons due to which treatment options, such as headgear, tend to fail [11]. Hence, many practitioners tend to go with an intraoral appliance, such as a pendulum, distal jet, or Jones jig [9]. Out of these options, the pendulum appliance is very effective for distalization of maxillary molars and the establishment of a Class I molar relationship in a relatively short period of time [12].
In comparison to the distal jet appliance and Jones jig appliance, the pendulum provides more distalization or space. The pendulum also has better control of the molar by minimizing tipping [7-10]. Furthermore, the distal jet and the Jones jig tend to create more mesial movement, greater mesial tipping, and extrusion of the maxillary premolars [13]. Many clinicians have mentioned that the pendulum appliance produces less second premolar anchorage loss and is more satisfactory for distalizing purposes [14, 15]. Other benefits of a pendulum include high patient tolerance and lower cost compare to other distalizing appliances.

The average time spent on molar distalization is between six to seven months. The monthly rate of maxillary molar distalization between the pendulum and other appliances, such as the Jones jig, are similar [11]. The pendulum achieves approximately about 1.2 mm of space per month [9]. Some studies have also reported that higher distalization is achieved prior to the eruption of maxillary second molars [12, 16].
After achieving sufficient space, a replacement of the pendulum appliance with a Nance holding appliance is recommended to reduce or prevent relapse. Additionally, it is recommended that premolar teeth distalization should be performed immediately. A stop in front of the molar tube could also help anchorage.
CONCLUSION
Based on the result of the treated case and findings from the previous study, it is possible to use the pendulum appliance as an alternative appliance for molar distalization on uncooperative patients with Class II malocclusion and unilateral or bilateral Class II molar relationships. The pendulum is also very effective in creating spaces for the eruption of canines and ectopic premolars. Pendulum appliances have been introduced for a long time and have proven successful for molar distalization and space regainer.
AUTHORS’ CONTRIBUTION
Himawan Halim contributed to treating the case and providing the treatment photos and radiographs. The author initiated the case report and gave the final approval of the manuscript.
Ivan A. Halim contributed to the literature review. The author completed the manuscript, critically reviewed, revised, and finalized it for the pre-publication stage.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
The patient gave consent for the publication.
STANDARDS FOR REPORTING
CARE guidelines and methodology were followed.
FUNDING
Not applicable.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

