All published articles of this journal are available on ScienceDirect.

Prevalence of Malocclusion and Associated Variables in Preschool Children of Tbilisi, Georgia
Abstract
Background:
Primary dentition is a determinant for future permanent occlusion.
Objective:
This aimed to evaluate the prevalence of malocclusion and associated variables in the primary dentition among preschoolers in the city of Tbilisi, Georgia.
Methods:
A cross-sectional survey was conducted among kindergarten children aged 3–5 years. Orthodontic characteristics were assessed by one calibrated clinician (E.G). Questionnaires were given to parents to record associated variables like general health problems, functional changes, and the presence of non-nutritive sucking habits.
Results:
A total of 396 participants aged 3-5 were included in the study. The prevalence of malocclusion was 49.8%, without significant differences among genders. The prevalence of Class II malocclusion was 21.2%(±4.091), followed by a deep overbite, i.e, 10.7% (±3.14), crossbite, i.e, 7% (±2.561), anterior open bite, i.e, 6.9%, and Class III malocclusion, i.e, 1.6% (±1.513). A total of 41.5% of children with breathing problems had Class II and 13% had crossbite. Speech disorder in 46.8% of cases was associated with anterior open bite. Pacifier users had Class II in 22.5%, deep overbite in 12.2%, and open bite in 9.2% of cases. There was a high prevalence of anterior open bite (25.2%) in children with a thumb-sucking habit (RR=4.90). These data sets are statistically reliable (p < 0.05).
Conclusion:
Almost half of the evaluated preschoolers had malocclusion. The most frequent disorder was Class II. Malocclusion is associated with non-nutritive sucking habits and mouth breathing.
1. INTRODUCTION
The perfect primary dentition is the predictor of future normal permanent occlusion. One of the main roles of primary dentition is to determine permanent occlusion and keep spaces for erupting teeth. Therefore, early diagnosis and treatment could prevent maxillofacial anomalies, deformities, and functional disorders in adulthood [1]. Also at an early age, we can manage facial growth, thus avoid physiological disturbances associated with malocclusions and maxillofacial anomalies. Environmental factors, like mouth breathing, chewing, swallowing, dietary changes, digit sucking, and prolonged pacifier use have been pointed out to be contributing to the development of malocclusions [2, 3]. Identifying and omitting these risk factors could prevent the progression of certain anomalies and are essential for the success of orthodontic treatment.
The studies conducted on primary dentition have been published since 1950, but generally of in descriptive format. The vast amount of epidemiological studies regarding the prevalence of malocclusions in primary dentition are seen mostly in the current century. The range of the prevalence varies between 21.0% to 88.1% [4-9]. There is a lack of such surveys in Georgia [10, 11]. Obtaining data about the occlusal status and possible environmental variables could help adopt oral health projects and prevent the development of dental deformities associated with early childhood malocclusions [12, 13]. Therefore, the aim of this study was to collect data about the prevalence of malocclusions and associated risk factors among preschool children of Tbilisi, Georgia. After this collected data, we will be able to raise awareness, evaluate preventive measures and practical recommendations for pediatric dentists, pediatricians, and other health care providers.
2. MATERIALS AND METHODS
The capital of Georgia, Tbilisi, was selected for the study location. The survey was conducted from March 2019 to June 2019. Multi-stage cluster sampling with preliminary stratification was applied to obtain a representative sample of preschoolers. In each stratum, kindergartens were selected using the PPS (Probability Proportional to Size) method.
Total 396 children aged 3 to 5 were evaluated in kindergartens drawn from ten districts of Tbilisi. Children were examined on-site. Occlusion was checked in maximum intercuspation, or if necessary mandible was manipulated into centric relation. Data inclusion criteria included the existence of fully erupted primary dentition, no partially or fully erupted permanent teeth, and no history of any orthodontic intervention. Data exclusion criteria were the presence of any permanent teeth, loss of any primary teeth, extensive dental caries that could affect the mesiodistal or occlusogingival dimension of a tooth and, therefore, influence the occlusal characteristics, tooth agenesis, congenital disorders (such as cleft lip/palate) or severe illness, and children unable to cooperate with the researcher.
Written permission from the kindergarten governing agency and written informed consent from parents or legitimate guardians of the participating children were obtained in each case. This study was approved by the Tbilisi State Medical University Biomedical Research Ethics Committee (re: 2015-0012 N1-2018/66. 17.04.2018). The study was held in the classroom provided by school authorities. Children were examined by a calibrated professional (E.G), who investigated occlusion and all its aspects under natural light in the presence of their parents/guardians, using a pair of disposable gloves and a mirror. The same professional interviewed parents using a special questionnaire, which included general information, such as gender and the age of the child. The questionnaire also included 10 questions about pregnancy, existing chronic diseases, feeding concerns, duration of breastfeeding, and oral and non-nutritive sucking habits (Questionnaire 1).
Oral and non-nutritive sucking habits were diagnosed according to intra- and extra-oral examination, with the consent from parents’ interview and filled questionnaire. Mouth breathing was reported according to the declaration of children's parents and clinical observation. Parents were asked about any history of treatment or adenoidectomy, any episodes of mouth breathing during the day and while sleeping. At the same time, children were examined extra orally in a relaxed position. Lip incompetence, muscle tension on lip closure, and nostril dilatation while breathing were considered mouth-breathing diagnostic factors. Speech problem was diagnosed at the site, by asking the child to speak specific words, at the same time observing tongue posture and articulation. Parents were asked if the child had any history of speech therapy. Generalised tooth caries and damaged crowns were considered as risk factors for chewing dysfunction. Accumulated calculus on occlusal surfaces was recorded as an indicator of chewing dysfunction.
Dental status was evaluated according to the Oral Health Assessment Form for Children (WHO, 2013) [14]. Occlusal relationships were evaluated using Foster and Hamilton criteria [15].
The following parameters were checked and recorded:
2.1. Primary Molar Relationship
The relationship of distal surfaces of primary second molars was evaluated and recorded according to the Baume classification.
a) Flush terminal plane (Class I or neutral occlusion)
b) Distal step (Class II)
c) Mesial step (Class III)
d) Asymmetric molar relationship
2.2. Primary Canine Relationship
The relationship of canines was considered to be normal or Class I if the cusp tip of the maxillary primary canine was in the same vertical plane as the distal surface of the lower canine in central occlusion. If the tip of the upper primary canine was anterior to the distal surface of the lower primary canine in central occlusion, it was considered as distal occlusion or Class II and if the tip of the upper primary canine was in posterior relationship to the distal surface of the mandibular primary canine, this was considered as mesial occlusion or Class III.
2.3. Overjet
The presence of sagittal space between upper and lower primary incisors was recorded.
2.4. Overbite
The coverage of lower primary incisors by the fully erupted primary upper incisors was measured. Cases with coverage of more than one-third were referred to as deep overbite.
2.5. Anterior Open Bite
The presence of vertical space between primary incisors.
2.6. Anterior Crossbite
Incorrect relationship between primary incisors; one or more mandibular primary occluded labially to their antagonists.
2.7. Posterior Crossbite
The transverse relationship between primary molars was considered as a posterior crossbite (unilateral, bilateral) when the buccal cusps of one or more maxillary primary molars were lingual to the buccal cusps of the mandibular primary molars and unilateral posterior crossbite when the mandible is guided into centric relation, changes into another transverse relationship, with contacts mostly on primary canines. This characterizes unilateral functional posterior crossbite.
2.8. Space Discrepancies/Spacing
No spaces between primary teeth were referred to as a risk factor for future predisposition to tooth size arch length discrepancy. The presence of spaces including primate spaces was referred to as normal.
2.9. Tooth Anomalies
They include shape anomalies, microdontia, macrodontia, supernumerary tooth, hypodontia, early eruption, late eruption, position anomalies, hard tissue lesions, etc. These types of disturbances were recorded by visual evaluation, without the involvement of any diagnostic tools.
2.10. Dental Arch Shapes
V-shaped, trapezoid, U-shaped are few of the examples. These types of disturbances were recorded by visual evaluation.
The obtained data were processed and analyzed using the SPSS v21.00 (Statistical Package for Social Sciences). The significance level was 0.05 for all statistical tests. Independent - samples T-test was used to compare the variables.
3. RESULTS
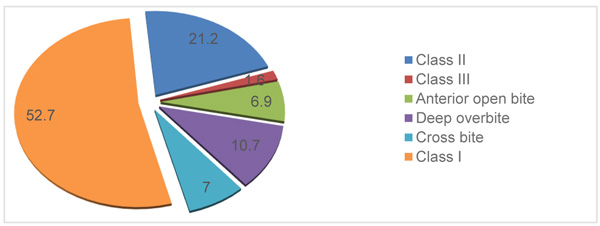
A total of 396 children aged 3 to 5 years, with an equal number of male and female subjects, were examined. The prevalence of malocclusion was 49.8%. Out of the malocclusions, Class II, deep overbite, crossbite, anterior open bite, and Class III were 21.2%, 10.7%, 7.0%, 6.9%, and 1.6% respectively with no significant differences in genders (Fig. 1).
Breathing problems were seen in 28.2% and speech problems in 11% of examined children (Table 1). Children with breathing problems had a high prevalence of Class II malocclusion and crossbite (41.5% and 13%, respectively) (Table 2). Specifically, mouth breathers had a higher incidence of Class II than children with normal breathing patterns (RR=2.93). The impact of mouth breathing was also observed on the upper dental arch (Table 3). In 51.2% of mouth breathers, a narrow upper arch was discovered. Speech disorder in 46.8% of cases was associated with anterior open bite.
| - | - | - | - | 95% Confidence Interval for Mean | |
| Dysfunction | N | Mean | Std. Deviation | Lower Bound | Upper Bound |
| Breathing | 112 | 0.282 | 0.450 | 0.237 | 0.326 |
| Chewing | 3 | 0.008 | 0.089 | -0.001 | 0.017 |
| Speech | 44 | 0.110 | 0.313 | 0.079 | 0.141 |
| Normal | 238 | 0.600 | 0.490 | 0.552 | 0.649 |
| - | Mouth Breathing | Mean | Std. Deviation | Lower Bound | Upper Bound | ± % | Sig. (2-tailed) |
| Class II | yes | 0.415 | 0.495 | 0.323 | 0.508 | 9.3% | 0.000 |
| no | 0.142 | 0.350 | 0.101 | 0.183 | 4.1% | - | |
| Class III | Yes | 0.028 | 0.167 | -0.003 | 0.060 | 3.1% | 0.725 |
| no | 0.022 | 0.148 | 0.005 | 0.040 | 1.7% | - | |
| Open bite | yes | 0.073 | 0.261 | 0.024 | 0.121 | 4.9% | 0.954 |
| no | 0.074 | 0.263 | 0.044 | 0.105 | 3.1% | - | |
| Deep bite | yes | 0.057 | 0.233 | 0.013 | 0.101 | 4.4% | 0.009 |
| no | 0.136 | 0.343 | 0.096 | 0.176 | 4.0% | - | |
| Cross bite | yes | 0.130 | 0.338 | 0.067 | 0.193 | 6.3% | 0.021 |
| no | 0.050 | 0.218 | 0.024 | 0.075 | 2.5% | - | |
| Normal | yes | 0.398 | 0.492 | 0.306 | 0.490 | 9.2% | 0.000 |
| no | 0.609 | 0.489 | 0.552 | 0.666 | 5.7% | - |
| - | - | - | - | 95% Confidence Interval for Mean | Error | t-test for Equality of Means | |
|---|---|---|---|---|---|---|---|
| Upper Dental Arch Form | Mouth Breathing | Mean | Std. Deviation | Lower Bound | Upper Bound | ± % | Sig. (2-tailed) |
| Narrow | yes | 0.512 | 0.502 | 0.418 | 0.606 | 9.4% | 0.000 |
| No | 0.144 | 0.351 | 0.103 | 0.184 | 4.1% | ||
| Elongated | yes | 0.126 | 0.333 | 0.063 | 0.189 | 6.3% | 0.539 |
| no | 0.150 | 0.358 | 0.108 | 0.192 | 4.2% | ||
| Shortened | yes | 0.097 | 0.297 | 0.041 | 0.152 | 5.6% | 0.945 |
| no | 0.094 | 0.293 | 0.060 | 0.128 | 3.4% | ||
| Widened | yes | - | - | - | - | - | - |
| no | - | - | - | - | - | - | |
| Extrusion | yes | 0.046 | 0.210 | 0.006 | 0.085 | 3.9% | 0.439 |
| no | 0.066 | 0.249 | 0.037 | 0.095 | 2.9% | - | |
| Intrusion | yes | 0.009 | 0.097 | -0.009 | 0.028 | 1.8% | 0.000 |
| no | 0.086 | 0.282 | 0.054 | 0.119 | 3.3% | - | |
| Normal | yes | 0.318 | 0.468 | 0.230 | 0.406 | 8.8% | 0.000 |
| no | 0.570 | 0.496 | 0.512 | 0.628 | 5.8% | - | |
Primary tooth caries was recorded in 41.4% of cases and generalised primary tooth caries in 8.3% of cases, and they were mostly associated with chewing dysfunction. On the other hand, children with generalised primary tooth caries had been breastfed for more than 3 years (1.5%).
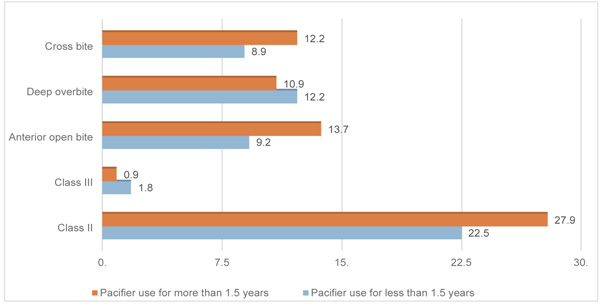
According to the questionnaire, pacifier use was confirmed in 59.1%, and in 31.9% of cases, it was used for more than 1.5 years. Children who used a pacifier for less than 1.5 years had Class II in 22.5% of cases, 12.2% had a deep overbite, and 9.2% of them had an open bite. Children with a prolonged pacifier sucking habit had a rate of malocclusion at 27.9%, 10.9%, and 13.7%, subsequently (Fig. 2). There was a high prevalence of anterior open bite (25.2%) in children with a thumb-sucking habit (RR=4.90) (Table 4). Total 67.9% of children who did not show any sign of oral dysfunctions had no signs of malocclusion. Malocclusion was not associated with gender, pregnancy, existing chronic diseases, preterm birth, and feeding concerns.
| - | NNSH | Total | RR | ||
|---|---|---|---|---|---|
| Yes | No | ||||
| Open bite | Yes | 74.8% | 94.9% | 92.6% | |
| No | 25.2% | 5.1% | 7.4% | ||
| Total | 100.0% | 100.0% | 100.0% | 4.90 | |
4. DISCUSSION
Our results, which revealed occlusal anomalies in 49.8% of cases, are in line with the global distribution of malocclusion in primary dentition between 21% and 88.1% [4-9, 12, 13]. These differences can be due to different methodologies, racial specifications, eating habits, and other characteristics.
The most frequent malocclusion, revealed in 29% of preschoolers, was Class II malocclusion, with primary second molar distal step, and increased overjet compared to Chinese and Danish children, in which the prevalence was 32.4% and 31.6%, subsequently [4]. They seem to be similar, but actually, there is a much higher incidence in British preschoolers (45%) [9].
Children with oral habits (such as pacifier, digit-sucking habits, and mouth breathing) are significantly more likely to develop anterior open bite, increased overjet, Class II canine relationship, and posterior crossbite as compared to children without a habit history [16, 17]. According to the data obtained from the questionnaire, 59.1% of children had used a pacifier that is quite close to the Portuguese study (61.7%). Our results reveal that most children who had pacifier sucking habits show a tendency to Class II malocclusion, with primary second molar distal step, and increased overjet (22.5%). Those who had a prolonged pacifier sucking habit (more than 1.5 years) had Class II with an anterior open bite at 27.9%. Different results were seen in the study of Urzal et al., where children with pacifier sucking habits had more tendency to anterior open bite and posterior crossbite [16]. Children who had a thumb-sucking habit in the past or still had it at the time of the evaluation had a high prevalence of Class II with anterior open bite (25.2%), which was in accordance with some other studies [17]. In the present study, children with no NNS (non-nutritive sucking) habits had normal molar and canine relationships, normal overjet, and overbite as in the results showed by Wagner et al. [1].
Allergic rhinitis and adenotonsillar hypertrophy are the main reasons for the obstruction of airways, that force a child to breathe through the mouth [18, 19]. Evaluation of maxillofacial system functions revealed that 28.2% of examined children had breathing problems. Children with breathing problems had a high prevalence of Class II (41.5%). These results are in agreement with other studies, where the higher incidence of Class II was considered in mouth breathers, rather than Class I [20].
Interesting findings were observed in children who were breastfed for a prolonged time (3 years or more). They had destruction of almost all primary teeth, with severe caries and damage of almost all hard tissues of teeth, although these children had no pacifier and thumb-sucking habits, and almost none of them had malocclusion. Some studies highlighted the correlation between socioeconomic factors and malocclusion. Poor perinatal health and pacifier use may be risk factors for malocclusion development in primary teeth. The long duration of breastfeeding is associated with better occlusal conditions in the children of adolescent mothers [21]. However, several studies have reported prolonged and unrestricted breastfeeding as a potential risk factor for primary tooth caries (ECC) [22, 23]. Children with generalised primary tooth caries were generally associated with low hygiene, poor dental education of parents, and probably low-income families [23].
The deep overbite was present in 10.7% of cases. This condition is less than that reported in other studies like Brazilian (19.7%) and German (33.2%) [24].
The posterior cross bite was revealed in 7% of the total sample and was mostly associated with narrow upper dental arch and mouth breathing. Previous studies have reported the frequency of this disorder ranging from 7.2% to 20.8% [13, 25].
The anterior open bite was found in 6.9% of the total sample, as compared to other studies where the average prevalence is between 2.8% and 46.2% [4, 5, 9]. According to Urzal V et al., anterior open bite frequency decreases from primary to mixed dentition, ranging from 16.9% to 11.4% [16].
Children with Class III molar and canine relationships were revealed in 1.6% of cases. Other studies have revealed much higher frequency, i.e, 6.7% and 8% [4, 24]. The difference could be due to the small sample size in the present study, which may enlarge the sampling error to misunderstand the actual situation.
Bernardo Q Souki et al. have reported that the prevalence of posterior crossbite was almost 30% in the children during primary and mixed dentitions, which is twice as high as our result (13%) [25].
Epidemiological studies on primary dentition are important to understand the distribution of oral health conditions in different populations and individuals and also to evaluate orthodontic treatment need in this particular age group. The malocclusion that definitely needs orthodontic treatment during primary dentition is an anterior and posterior crossbite, while other conditions can be registered and parents should be given appropriate information about future treatment options. Occlusal discrepancies connected with NNS (non-nutritive sucking habit) usually self-correct if the habit is removed [26]. Functional disorders, including mouth breathing, should be collaborated between different practitioners (pediatricians, allergists, speech therapists, otorhinolaryngologists, etc.)
Early diagnosis, preventive measures, and treatment might prevent further development of maxillofacial anomalies, deformities, and functional disorders. Additionally, we can manage facial growth at an early age in order to avoid physiological disturbances associated with malocclusion and maxillofacial anomalies.
CONCLUSION
After the evaluation of 396 Georgian preschoolers, the following conclusions can be drawn:
• Malocclusion remains a problem in the preschoolers of Tbilisi.
• There is a strong association between malocclusions and non-nutritive sucking habits.
• There was a strong association between thumb sucking and prolonged pacifier use and Class II malocclusions with anterior open bite.
• There is higher susceptibility to develop Class II malocclusions in mouth breathers.
• There is a need for raising awareness among pediatric dentists, pediatricians, and other health care providers in detecting early dental anomalies and timely referral to orthodontists.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Tbilisi State Medical University Biomedical Research Ethics Committee (re: 2015-0012 N1-2018/66. 17.04.2018).
HUMAN AND ANIMAL RIGHTS
No Animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written permission from the kindergarten governing agency and written informed consent from parents or legitimate guardians of the participating children were obtained in each case.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors wish to acknowledge the help provided by the head of Ivane Javakhishvili Tbilisi State University dental health department, D.M.D., Ph.D., D.M.Sci Vladimer Margvelashvili. We would also like to thank the staff of the Tbilisi Kindergarten Agency for their cooperation.
We want to express special thanks and gratitude to Professor, Head of Pediatric Dentistry Department, Faculty of Medicine, Tbilisi State University, Manana Kalandadze, for being the principal supervisor of this project.

