All published articles of this journal are available on ScienceDirect.

An Update on Root Canal Preparation Techniques and How to Avoid Procedural Errors in Endodontics
Abstract
Background:
Effective root canal treatment involves cleaning and shaping root canals using a range of instrumentation procedures and techniques. The aim of this review was to provide an update on root canal hand instrumentation techniques and how to overcome iatrogenic errors.
Methods:
A comprehensive search was carried out using multiple databases, PubMed, Medline, Google scholar, and Scopus, to identify relevant studies addressing the objective of this study and to summarize the current evidence to readers. Keywords, i.e., endodontics, root canal preparation, hand instrumentation, techniques and procedural errors, as well as, MeSH terms, i.e. “endodontics”, “instrumentation”, “root canal preparation” were used to conduct our comprehensive search.
Results:
The hybrid technique is a commonly-used approach that combines the benefits of both the crown-down and step-back techniques and was reported to be one of the best techniques to produce an optimal root canal preparation outcome. Hand-instrument manipulation using the balanced forced technique is also favoured as it rapidly and safely permits removal of canal contents allowing irrigants and medications to reach deep inside canal spaces.
Conclusion:
The use of hand files is still recommended for initial canal negotiation and preparation and is essential for the correction of procedural errors. This study provided an update on several hand instrumentation techniques commonly used in endodontics. The correct and safe application of these techniques can prevent iatrogenic procedural errors from occurring which optimizes the quality of treatment outcome.
1. INTRODUCTION
Dental students learn the required skills as depicted in their BDS program in two stages, namely, pre-clinical simulated clinical activities followed later by the clinical activities carried out on patients. Due to the high cost and demand on the resources to run these simulated activities, it is important to optimise the methods of learning and make sure that these methods have been evidenced [1-3].
The objective of root canal treatment is to thoroughly clean, disinfect, and seal the root canal system. To accomplish this goal, a biomechanical debridement of the root canal system is essential [4]. This process involves a combination of mechanical instrumentation with chemical disinfection to eliminate most of the infective microorganisms in the root canal system, as well as the inorganic contaminant debris and dentin [5]. Cleaning and shaping the root canal system is a complex procedure that involves the manipulation of endodontic hand instruments in a variable, curved multiple canal system [4]. For completing the instrumentation procedure, there is a range of hand instrument preparation and manipulation techniques to mechanically remove canal contents and infected dentine, e.g., crown-down, step-back, and hybrid techniques, using reaming, filing, watch-winding, circumferential filing, and the balanced force manipulations [6]. The inaccurate or incorrect manipulation of endodontic hand instruments during canal instrumentation can result in a number of iatrogenic procedural errors [7]. These may include straightening of the root canal, the development of ledges, apical zipping, canal transportation, perforations, and instrument separation [8].
The purpose of this review was to provide an update on root canal hand instrumentation techniques commonly used in endodontics, including how to overcome iatrogenic errors and optimize the quality of endodontic treatment outcomes.
2. METHODS
The following electronic databases were searched to identify relevant articles according to our topic: PubMed, Medline, Google scholar, and Scopus until November 2020. The task of searching the above databases was carried out by two investigators to eliminate any potential bias in selecting the relevant articles. The following keywords were used to conduct a comprehensive search so that no key studies were missed during the search: hand files, root canal preparation, techniques, hand instrumentation, procedural errors, performance, and endodontics, as well as, MeSH terms, i.e. “endodontics,” “instrumentation,” and“root canal preparation”. Inclusion criteria included all types of studies investigating root canal hand instrumentation techniques and discussing the prevention of resulting procedural errors in endodontics.
3. RESULTS
3.1. Learning Endodontic Skills
It is well established that learning endodontic theory and techniques can be challenging for undergraduate dental students [9-12]. Students are required to gain essential knowledge and develop related practical skills in a relatively short period of time. Specifically, they need to integrate their theoretical knowledge and fine motor skills and show continuous improvement in performance to achieve the competencies required to provide patient care.
Learning endodontic skills often begins with the simulated practice of the different stages of root canal treatment on extracted human teeth. Biomechanical cleaning and shaping of the root canal space is an essential step [6, 13, 14], aimed at eliminating or minimising the number of microorganisms causing infection in the root canal system. This includes removing debris and microorganisms from the root canal system and shaping root canal spaces to facilitate cleaning and subsequent filling of the canal space (Fig. 1). When using extracted human teeth, variable external and internal anatomy, as well as the condition of the root, make the biomechanical preparation of root canal systems a challenging and sometimes discouraging task. Therefore, a recent recommendation for the simulation stage of learning endodontic procedures is to use simulated plastic models of canals and teeth prior to the use of extracted human teeth [15].
The simulated root canals permits the standardisation of the root canal hardness, length, width (diameter), location and degree of canal curvature. This standardisation allows the reproducibility of the outcomes [16]. Consistent with the recommendations of learning using simulated root canals, simulated plastic blocks and teeth have been found to be a valuable adjunct for learning how to determine root canal working lengths [17] and how to carry out preparation techniques [18, 19]. Studies have used simulated root canals (e.g., resin blocks, plastic teeth, and artificial dentine) to investigate and compare the shaping ability of instruments, to compare different root canal instrumentation techniques, and to identify possible procedural errors during root canal preparation [7, 16, 20, 21]. However, how realistically simulated canals in resin teeth or blocks mimic canals in natural teeth is unclear. For example, differences in properties between resin and dentine may be an issue. Microhardness of root canal dentine has been reported to be 35-40 kg/mm2 compared to 20-22 kg/ mm2 for clear resin endodontic blocks, and 25-26 kg/ mm2 for artificial resin teeth [16, 22, 23]. Moreover, it has been reported that the size of shavings resulting from resin and dentine is different, leading to more canal blockages in resin-simulated root canals [22]. Despite these concerns, simulated root canal models have been reported to be a suitable alternative for natural teeth in learning root canal preparation procedures [19, 24].
The blinded nature of endodontic procedures adds further complications for novice students. They do not have visual cues to support their linking and transferring their theoretical knowledge of root canal morphology and root canal preparation techniques to produce appropriately shaped and cleaned root canal spaces that are ready to be filled. In response, recommendations from the Australian Society of Endodontology and guidelines from the European Society of Endodontology support the use of visual demonstrations (observation) of simulated root canal procedures and techniques during learning [15, 25].
The success of root canal treatment relies mainly on effective cleaning and shaping of the root canal. This involves using a range of instrumentation procedures. The correct and safe application of these procedures and techniques can also prevent iatrogenic procedural errors from occurring.
3.2. Root Canal Preparation Instruments
Root canal preparation includes mechanical (i.e., debridement and shaping of root canal space) and chemical procedures (i.e., cleaning root canals using irrigants and medications to minimise bacterial presence). Learning to mechanically prepare root canals requires the use of instruments, such as hand files and engine-driven rotary files. While nickel-titanium (NiTi) rotary files may be considered the gold standard for root canal preparation [26-28], the use of traditional hand files remains of critical importance [6]. Hand files are recommended for initial canal negotiation and preparation prior to the use of rotary files to further enlarge the canal [29, 30]. If rotary instrumentation techniques are used, it is also recommended that hand files should be used in between rotary file applications to help prevent any blockage of the canal system with debris created by a rotary file system [6, 31, 32].
In addition, hand files are essential for the correction of procedural errors (e.g., by-passing ledges or blockages), preparation of large canals (e.g., maxillary central incisors, canines), and in cases where the use of rotary files may be limited (e.g., in cases of apical resistance and anatomical variations in the canal system) [31, 33]. Therefore, learning the fundamental skills of hand file manipulation is a crucial step prior to learning the use of other advanced armamentariums (i.e., rotary files) for root canal instrumentation procedures [29].
3.3. Root Canal Instrumentation Techniques
Mechanical root canal preparation using hand instruments involves the adaptation of relevant techniques to enable the instrument to properly clean and shape the root canal system to the full length of the canal. The objective of mechanical preparation is to remove infected soft and hard tissues, to facilitate the delivery of root canal irrigants and medicaments to the apical area of the root canal system, and to preserve the integrity of the root canal structure (i.e., prevent weakening of the root structure by removing too much dentine) [6].
This objective can be achieved by cleaning and shaping the root canal from a reference point (i.e., a point on the sound tooth structure) to a slightly short area (0.5-1 mm) of the canal terminus, i.e., the foramen [6]. This length is referred to as the working length of the root canal. The working length is estimated using a pre-operative radiograph of the tooth, often established with the use of an electronic apex locator and confirmed radiographically after inserting a small file in the root canal to the predicted working length [34]. The maintenance of working length can be achieved by using copious amounts of irrigation and frequent insertions of a small file to the full working length to clear and loosen accumulated debris and dentine shavings from the apical portion of the canal. Many different instrumentation techniques (e.g., standardized, circumferential filing and step-down) have been discussed in the literature [7, 35, 36]. The choice of root canal preparation technique is dictated somewhat by the design and shape of the instrument [37]. K-type hand instruments are most commonly used during root canal preparation procedures [6]. This is mainly due to their safety during the cleaning and shaping of root canals [38].
Table 1 provides a summary of the commonly used hand instrumentation techniques, which will be discussed below in detail.
Table 1.
| Instrumentation Technique | Properties | |
|---|---|---|
| 1. | Crown-down | - Preparation from coronal to apical part of the root - Flaring coronal part of the root - Reduces the risk of apical blockage - Improves access to the full length of the canal - Enhances tactile sensation to the apical portion of the canal |
| 2. | Step-back | - Preparation from apical to coronal part of the root - Stepwise reduction in the working length with progressively larger instruments - Produces flared and tapered root canal |
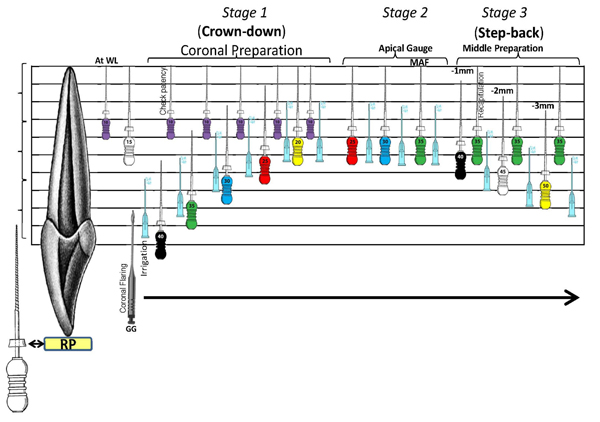
| 3. | Hybrid (modified double-flared) | - Starts with coronal preparation using crown-down method, then enlargement of the apical portion of the canal, and finishes with middle root canal preparation using the step-back technique. - Combines the benefits of crown-down and step-back techniques |
| 4. | Balanced force | - Involves a series of rotational movements - Has superior maintenance of canal curvature and prevention of procedural errors - Provides adequate apical control and good centring of the hand instrument in the root canal |
3.4. Crown-Down
The crown-down technique prepares the root canal by starting from the coronal part of the root canal system and then progressing to the apical region [39]. This technique relies on flaring the coronal part (Fig. 2) of the root canal (i.e., progressing from large to small hand instruments), which enables the removal of infected soft tissue, reduces the risk of blockage of the apical portion of the root canal, and minimises extrusion of canal contents beyond the apical area [7]. By commencing with the coronal section of the root canal, this technique improves access to the full length of the canal, enhances tactile sensation to the apical portion of the canal, and reduces the risk of fractures [40]. The crown-down technique has been reported to be superior to the step-back technique in the preparation of curved root canals ranging from 10 to 35 degrees of curvature [39].
3.5. Step-Back
The step-back technique relies on preparing the root canal, starting from the apical part and progressing to the coronal part [35]. It incorporates a stepwise reduction in the working length (i.e., 1 mm steps), but with progressively larger instruments, it produces a flared and tapered root canal. This technique is one of the traditional root canal preparation techniques and is believed to be effective in minimising procedural errors [6].
3.6. Hybrid (Modified Double-Flared)
The double-flared technique was first introduced by Fava [41]. This technique was then improved and referred to as the ‘modified double-flared’ technique [42] or ‘hybrid’ technique [6, 31]. It negotiates by reaching the end of the root canal with a hand instrument. This is followed by preparation of the coronal part of the canal using the crown-down technique, then enlarging the apical part of the root canal. Finally, the middle part of the root is prepared using a step-back technique (Fig. 1) [42]. This technique combines the benefits of both the crown-down and step-back techniques.
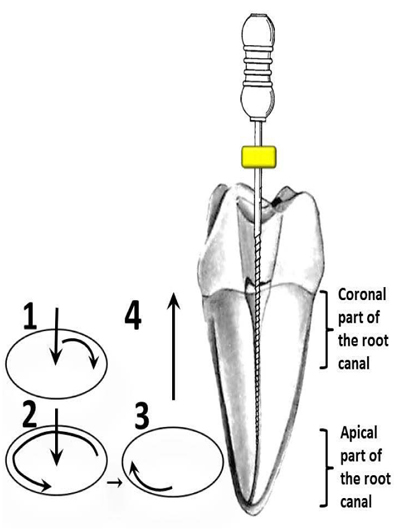
1 = Insert file and engage it in the canal wall with a quarter-clockwise rotation turn, 2 = Maintain pressure and turn the file in a three-quarters counter-clockwise direction to cut the dentine of the canal wall, 3 = Turn the file clockwise without pressure, and 4 = Remove the file from the canal;
3.7. Hand Instrument Manipulation: Balanced Force Technique
For completing the instrumentation procedure, a range of hand instrument manipulation strategies to mechanically remove canal contents and infected dentine, e.g., reaming, filing, watch-winding, circumferential root canal filing, and the balanced force technique, are performed [6]. The balanced force technique (BFT) involves a series of rotational movements (Fig. 2) that enable hand instruments to advance in the root canal [36]. BFT has been shown to be a favourable hand instrument manipulation technique compared with other instrumentation techniques due to its superior maintenance of canal curvature and prevention of iatrogenic procedural errors [6, 29, 43]. It provides adequate apical control of the tip of the hand instrument and good centring of the instrument in the root canal [7].
The balanced force technique involves introducing the instrument into the root canal with a quarter-clockwise motion with light pressure to engage the hand instrument with the canal walls. This is followed by maintaining the pressure while completing a three-quarter counter-clockwise turn, thereby cutting the dentine of the canal, resulting in enlargement of the canal. The final step involves a quarter clockwise motion, without pressure, to collect the shavings from the canal walls and removal of the hand instrument from the root canal (Fig. 2). The incorrect use of any of the previously mentioned techniques or failure to maintain working length could lead to procedural errors, such as the blockage and ledge formation in the root canal [7, 34].
3.8. Endodontic Measures of Success
The success of root canal treatment depends on accessing the apical part of the root canal during root canal preparation and maintaining this access during chemo-mechanical preparation [44]. The clinical outcome measures for root canal preparation procedures involve assessing the quality of canal instrumentation, including accuracy of the preparation and the presence or absence of procedural errors during the shaping of the root canals [7].
3.9. Quality of Root Canal Preparation
As mentioned earlier, the success of root canal preparation relies mainly on effective cleaning and shaping of the root canal system. This can be achieved through chemo-mechanical preparation of the canal from a coronal reference point (i.e., a point on the incisal or occlusal surface of the tooth) to the apical end of the root canal [45]. The assessment of the quality of the root canal preparation can be achieved clinically and radiographically [37]. Clinically, the accuracy of canal preparation can be determined via tactile digital sense by inserting the hand instrument in the root canal, ensuring that the instrument can smoothly reach the full working length of the canal [45]. This then can be confirmed radiographically by measuring the distance from the tip of the instrument to 0.5 to 1 mm short of the radiographic end of the root canal [6].
Instrumentation to a shorter length can result in the accumulation of debris, leading to procedural errors. These errors include canal blockage, ledge formation, canal transportation, and fracture of the hand instrument.
3.10. Root Canal Preparation Errors
As mentioned previously, procedural errors can occur during root canal instrumentation using hand instruments.
3.11. Blockage of the Root Canal
This involves an obstruction in a previously patent canal, resulting from the accumulation and retention of dentine chips or residual tissues at the apical part of the canal [8]. Canal blockage can be identified by an inability to advance an instrument to the full working length of the canal. A blockage can be associated with the instrumentation technique used. In a study that compared eight preparation techniques, it was found that canal blockage occurred least when the balanced force technique was used [46].
3.12. Ledge Formation
This has been shown to be associated with the degree of canal curvature and the design of the selected hand instrument [47]. For example, ledging of a root canal can result from preparing the canal using inflexible instruments (e.g., large files that have reduced flexibility). A ledge usually occurs on the outer side of the canal curvature as a step (platform) that can then be challenging to bypass and can ultimately lead to an inability to negotiate past the root canal ledge [7]. Ledges can be differentiated from canal blockage by the characteristics of tactile sensation and radiographically [8]. Specifically, advancing an instrument in the canal will feel like the file is hitting a solid wall, while radiographically, the image would show the tip of the instrument directed away from the true canal path.
3.13. Canal Transportation
This results from a tendency of the instrument to straighten a curved canal; as a result, the main path of the canal is deviated from its original canal pathway [7]. Canal transportation can be detected radiographically due to the straightening of a curved canal as compared with the original path of the root canal [20]. It has been reported that using NiTi files results in less canal transportation compared with stainless steel files [48].
3.14. Fracture of Hand Instruments
Fracture of hand instruments can result from torsion stress (i.e., an overload of force during twisting) or fatigue through flexure and repeated use of the instrument [49]. Hand-instrument fracture can be associated with the radius and angle of the canal curvature, instrumentation technique, rotational forces applied on the instrument, and experience of the operator [49]. Fracture of hand instruments can also be related to the type of hand instrument used. For example, H-type hand instruments are more likely to fracture compared with K-type instruments due to the manufacturing process and reduced cross-sectional area [6]. The use of NiTi instruments during root canal preparation can result in reduced procedural errors compared with stainless-steel hand instruments [13]. This can be explained by the flexible nature of NiTi files and their ability to conform within curved root canals, therefore being less susceptible to the fracture [50].
3.15. Fracture of a Tooth
This usually occurs in the crown and/or root. Cracked or fractured root canals are frequently difficult to diagnose and treat. In relation to root canal preparation, root canal fracture can occur when the forces used during canal preparation are beyond the elastic limit of the root canal wall [51]. However, there is limited evidence that root fractures are associated with forces generated during root canal preparation procedures [52, 53].
CONCLUSION
The hybrid technique is a commonly-used approach that combines the benefits of both the crown-down and step-back techniques and was reported to be one of the best techniques to produce an optimal root canal preparation outcome. Hand-instrument manipulation using the balanced forced technique is also favoured as it rapidly and safely permits removal of canal contents allowing irrigants and medications to reach deep inside canal spaces. The correct and safe application of these techniques can prevent iatrogenic procedural errors from occurring.
This study provided an update on several techniques commonly used in endodontics, including how to overcome iatrogenic errors and optimize the quality of endodontic treatment outcomes.
CONSENT FOR PUBLICATION
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors report no conflict of interest in the preparation of this manuscript.
ACKNOWLEDGEMENTS
Declared none.

