All published articles of this journal are available on ScienceDirect.

Multimodal Protocol for the Treatment of Odontogenic Keratocysts
Authors Info & Affiliations
Abstract
Purpose:
The aim of this study is to evaluate longitudinally the effectiveness of a multimodal protocol based on decompression followed by enucleation combined with the use of liquid nitrogen under local anesthesia for the treatment of odontogenic keratocysts.
Methods:
Seven patients with a diagnosis of odontogenic keratocyst were evaluated longitudinally to clinical and histological features, and pre- and postoperative radiographs were analyzed. Data were collected on the epidemiological profile of patients and on cysts, including the presence of recurrence, duration of drainage device use, lesion site, and presence of postoperative complications.
Results:
No recurrence was observed during follow-up. Mean follow-up was 59.57 months (range, 18-96 months). No pathological fracture was observed. None of the patients had persistent paresthesia of the inferior alveolar nerve. Substantial reduction in cyst size and epithelial differentiation were observed in all patients after multimodal treatment.
Conclusion:
Based on these results, the multimodal protocol proposed here was effective in the treatment of odontogenic keratocysts by reducing lesion size, avoiding possible damage to adjacent anatomical structures, and allowing a surgical procedure with less morbidity. The longitudinal follow-up of patients showed that this treatment modality is associated with a low recurrence rate compared with alternative therapies.
1. INTRODUCTION
The Odontogenic Keratocyst (OKC) is a cystic lesion of odontogenic origin classified as a developmental cyst derived from the dental lamina [1]. OKC accounts for approximately 10% of all odontogenic cysts [2, 3]. It is known for the locally aggressive behavior and a high likelihood of recurrence, with rates ranging from 2.5 to 62.5% during the first 5 years after treatment [2, 4, 5]. For this reason, OKC has been extensively investigated in recent decades [1]. The lesions are more prevalent in the second and third decades of life, with a slight predilection for males [6, 7]. OKC often presents as a single lesion, unless it is associated with basal cell nevus syndrome [8]. It may occur anywhere in the jaws, but there is a preference for the mandible, most commonly in the posterior region - body and ascending ramus (65-83%) [3].
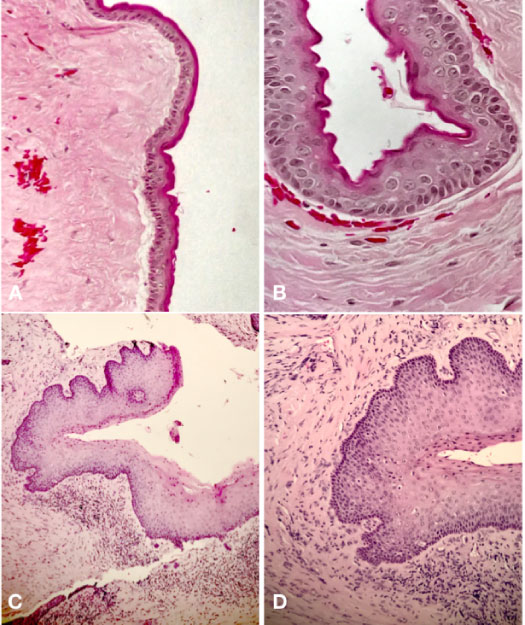
Radiographically, OKC presents as a well-defined, multilocular or unilocular, radiolucent lesion, and 25 to 40% of cases are associated with an unerupted tooth [7]. Histologically, there is a thin lining of corrugated parakeratinized stratified squamous epithelium, with a prominent basal layer composed of 6-8 cuboidal or columnar cells and a basal layer of palisade cells, associated with an inflammation-free connective tissue wall [3, 7].
The treatment of OKC remains controversial. Over the years, several surgical techniques have been proposed to treat OKC. Treatment modalities are divided into conservative (simple enucleation with or without curettage, marsupialization, decompression) and radical (peripheral osteotomy, marginal resection) [9]. Changes in treatments with the use of adjuvant therapies, such as cryotherapy, aim to eliminate the potential risk of recurrence while minimizing surgical morbidity [6].
OKC adherence to epithelial and connective tissue is poor, which often leads to lesion fragmentation during enucleation. As a result, cystic epithelial cells are left in the surgical site, with high recurrence potential [10]. Cryotherapy, as an adjuvant therapy, consists in applying liquid nitrogen directly to the cystic cavity in order to eliminate epithelial remnants and satellite cysts. Liquid nitrogen has the ability to cause cell necrosis by means of direct damage to the intracellular and extracellular surfaces owing to the formation of ice crystals that affect the osmotic and electrolyte balance, preserving inorganic bone structures to allow osteoconduction [5]. Cryotherapy is a well-tolerated treatment with few associated complications, which makes it an excellent option for the treatment of locally aggressive dental lesions [11].
Several authors have already demonstrated that the aggressive nature of OKC does not always justify radical treatment [12]. Thus, several treatment modalities have emerged aiming to balance the potential risk of recurrence and treatment morbidity. An example is decompression [8]. The decompression of odontogenic cysts has been widely used as an alternative to conservative treatment. Tucker was the first to describe, in 1972, the technique of decompression followed by enucleation as a treatment modality for OKC [1]. The benefit of this protocol over other conventional approaches [enucleation and en bloc resection] lies in the minimal surgical morbidity. In addition, associated bone structures, such as the inferior alveolar nerve and developing teeth, are less vulnerable to damage [8].
Considering that we aim and benefit from the use of a protocol with minimal surgical morbidity, many strategies have been developed to reduce clinical signs and symptoms following procedures with local anesthesia, including the use of pharmacological therapy to inhibit the release of the inflammatory mediators responsible for this acute response [9-11].
The purpose of this study was to evaluate longitudinally the effectiveness of a multimodal protocol based on decompression followed by enucleation combined with the use of liquid nitrogen under local anesthesia for the treatment of odontogenic keratocysts.
2. MATERIALS AND METHODS
A longitudinal study was conducted at the Pontifícia UniversidadeCatólica do Rio Grande do Sul [PUC-RS]’s Department of Oral and Maxillofacial Surgery from March 2010 to April 2020. This study followed the Declaration of Helsinki on medical protocol and ethics and the Ethical Review Board approved the study (CAAE: 30409320.1.0000.5336).
2.1. Sample
The sample consisted of consecutive patients treated with the multimodal protocol described in the study. All lesions were evaluated on routine radiographs. The preoperative diagnosis was made by incisional biopsy and then confirmed histopathologically by the presence of a corrugated paraceratinized thin layer, stratified squamous epithelium with a prominent basal layer composed of 6 to 8 cuboidal columnar cells and a palisade basal layer.
2.2. Inclusion and Exclusion Criteria
Eligible participants were all patients with a histopathological diagnosis of OKC who had any anatomical structure involved in the lesion or risk of pathological fracture after enucleation and cryotherapy without signs or symptoms of local infection. Patients with incomplete medical records, history of previous treatment, no written informed consent, and diagnosis of basal cell nevus syndrome were excluded.
2.3. Data Collection
Data were collected on the epidemiological profile of patients, including age, sex, and medical history, on OKCs regarding recurrence during the follow-up period, and on pre- and post-treatment panoramic radiographs. The following data were also collected regarding the clinical characteristics of lesions: location, the presence of impacted teeth and root resorption, duration of decompression device use, the presence of complications resulting from decompression device use and postoperative surgical complications.
2.4. Multimodal Protocol
The multimodal protocol was designed based on the methodology that Pogrel [20] and Tonietto [5] used in their studies, involving decompression and irrigation as the first step, followed by enucleation and treatment of the cystic cavity with liquid nitrogen as the second step. Both steps were performed under local anesthesia (4% articaine with 1:100,000 epinephrine).
2.5. Decompression and Irrigation
Cystic decompression was performed by removing the mucosal lining and bone tissue, inserting the irrigation cannula into the cystic cavity, which was stabilized with a suture of the oral mucosa. A sample of the cystic capsule was sent to PUC-RS School of Dentistry’s Oral Pathology Laboratory for histopathological diagnosis.
Patients were instructed to irrigate the cystic cavity twice daily with a 20-mL syringe containing saline solution. Regular return visits were arranged to monitor and evaluate the decompression device. The maintenance period of the decompression device was established based on this outpatient return visits and on panoramic radiographs taken monthly, regression of lesion size was assessed as an effect of decompression and new bone formation, releasing anatomical structures that could have been involved.
2.6. Enucleation and Cryotherapy
At the time of the second intervention, enucleation was performed, followed by cryotherapy. After curettage of the lesion, the adjacent tissues were protected with dry gauze pads and liquid nitrogen was applied directly to the cystic cavity using a cryotherapy device, spray, and a No. 12 tracheal aspiration tube. Three 1-minute applications were performed, with an interval between applications to allow defrosting to occur.
2.7. Radiographic Evaluation and Follow-up
For each patient, a panoramic radiograph was taken before treatment and each month after placement of the decompression device. Only when the anatomical structure involved by the lesion was diagnosed radiographically as outside the cystic lumen and with adjacent new bone formation, the patient was referred for surgical enucleation and cryotherapy.
Post-resection radiographic follow-up was performed every 6 months for the first year, and every 12 months thereafter.
2.8. Histopathological Examination
At the time of decompression, a sample of the cystic capsule was removed and examined histologically at PUC-RS School of Dentistry’s Oral Pathology Laboratory. After enucleation and cryotherapy, additional samples of the cases were examined histologically to assess epithelial changes and confirm the diagnosis. A comparative descriptive analysis between the 2 biopsies of each patient was performed by the same operator.
3. RESULTS
This longitudinal study evaluated 7 patients, 3 women and 4 men, with a mean age of 32.57 years [range, 19-60 years]. Six cysts were located in the posterior mandible [body and/or mandibular ramus], and 1 cyst was located in the anterior maxilla. None of the patients had previous clinical signs and symptoms, and all of them were diagnosed by radiographic findings. No patient had received previous treatment. The demographic characteristics of patients and the characteristics of lesions are shown in Tables 1 and 2, respectively.
| Patient | Age | Sex |
|---|---|---|
| 1 | 20 | F |
| 2 | 20 | M |
| 3 | 19 | M |
| 4 | 20 | F |
| 5 | 47 | F |
| 6 | 42 | M |
| 7 | 60 | M |
| Mean | 32.57 | M: 57.14% F: 42.85% |
Perforation of the bone cortex was not observed [clinically or radiographically] in any patient. Four patients [57.14%] had an impacted tooth associated with the lesion. In 3 cases, the tooth was removed, and 1 case was opted for tooth retention and later orthodontic traction -the decision not to extract the tooth was based on the fact that it was an impacted third molar with the possibility of replacing the second molar with resorption.
The mean duration of decompression device use was 7.14 months (range, 3-12 months). In 2 patients, it was lost, and another device had to be placed. The positioning of the decompression device in the oral cavity is shown in Fig. (1).
| 7 | 6 | 5 | 4 | 3 | 2 | 1 | P |
|---|---|---|---|---|---|---|---|
| Maxilla (anterior region) | Mandible (body and ramus) |
Mandible (body and ramus) |
Mandible (ramus) |
Mandible (body) |
Mandible (body) | Mandible (body and ramus) |
Location |
| No | Yes | No | Yes | Yes | No | Yes | Impacted tooth |
| No | No | No | No | No | No | No | Root resorption |
| 3 | 11 | 12 | 5 | 7 | 6 | 6 | Decompression device (months) |
| 19 | 18 | 60 | 57 | 72 | 95 | 96 | Follow-up (months) |
| No | No | No | No | No | No | No | Recurrence |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Epithelial differentiation |
| Nasal cavity and maxillary sinus | Inferior alveolar nerve | Inferior alveolar nerve | Inferior alveolar nerve | Inferior alveolar nerve | Mental nerve | Inferior alveolar nerve | Anatomical structure involved |

In a histological comparison of the incisional biopsy performed at the time of decompression device placement and after enucleation and curettage [resection], all patients showed epithelial differentiation, where the cystic epithelium became hyperplastic and a subepithelial inflammatory infiltrate was observed (Fig. 2).
All lesions observed in this study involved at least one important anatomical structure. The inferior alveolar nerve was involved in 5 cases, the mental nerve in 1 case, and the maxillary sinus and nasal cavity in 1 case.
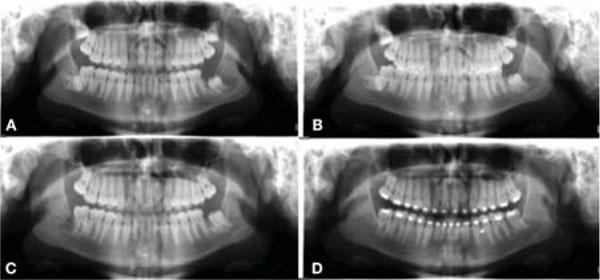
Significant regression of lesion size was observed on panoramic radiographs obtained during the decompression period. It was possible to diagnose that important anatomical structures, such as the inferior alveolar nerve, which were previously involved by the cystic lesions, were no longer involved, and adjacent new bone formation was observed between the anatomical structure and the cyst. An example of evidence of lesion size regression after decompression on panoramic radiographs is shown in Fig. (3).
Postoperative complications observed during treatment are shown in Table 3. Two patients who had paresthesia of the inferior alveolar nerve reported a return of nerve function within 6 months of the surgical procedure. There were no cases of pathological mandibular fracture or major complication. Mean follow-up was 59.57 months [range, 18-96 months]. No recurrence was observed during follow-up.
| Postoperative complications | |
|---|---|
| Loss of drainage device | 2 [28.57%] |
| Suture dehiscence | 2 [28.57%] |
| Infection | 0 |
| Paresthesia [inferior alveolar nerve] | 2 [28.57%] |
| Bleeding | 0 |
| Mandibular fracture | 0 |
| Recurrence | 0 |
4. DISCUSSION
OKC is one of the most common odontogenic cysts and requires special attention due to its locally aggressive behavior and likelihood of recurrence. There are several therapeutic modalities for the management of OKCs, ranging from conservative methods, such as enucleation and decompression, to more aggressive techniques, such as peripheral osteotomy and en bloc resection. There has been much debate about which therapeutic modality is most effective, with less morbidity and lower rates of recurrence [16]. In view of this discussion in the literature, the present study evaluated an alternative treatment based on a multimodal protocol consisting of decompression followed by enucleation and cryotherapy and showed favorable results over time, with low morbidity and no sequelae to patients.
Regarding epidemiological data, the mean patient age of 32.57 years is consistent with data from previous studies reporting that OKCs occur more frequently in the second and third decades of life [2, 5, 12], as well as with data showing a predilection for males [5, 7, 12]. The anatomical location of the lesions is also in agreement with the literature, with a preference for the posterior mandible [12].
OKC is considered one of the most aggressive odontogenic cysts due to its high risk of recurrence and tendency to invade adjacent tissue [7]. The high recurrence potential can be attributed to technical and surgical difficulties that result in incomplete removal of the lesion, since it shows poor adherence to epithelial and connective tissue, with a thin friable cyst lining [7, 12]. Incomplete removal of the capsule, growth of a new cyst from small satellite lesions or epithelial remnants left behind during surgery may explain the high rates of recurrence [5, 12]. Therefore, it is believed that complete removal of the lesion capsule reduces the chance of recurrence [5]. One of the reasons to create a multimodal protocol treatment was to avoid recurrences, because the authors believe that the association between thick capsule after decompression and cryotherapy during cyst removal are two techniques favorable to eliminate the OKC without recurrences, and the results observed in this study corroborate to that.
Considering the different surgical treatment modalities available for OKC, enucleation appears as the option with the least morbidity. However, this technique seems to result in the highest recurrence rate, especially for capsule rupture during the surgical procedure. Marginal resection, in turn, has the lowest recurrence rate but the highest treatment-related morbidity rate [3, 4, 7-16]. Because OKC is clinically silent, lesions are usually diagnosed at a large size, thus requiring more invasive surgical procedures and major reconstructions to restore form and function. Changes in treatments with the use of adjuvant therapies aim to eliminate the potential risk of recurrence while minimizing surgical morbidity [6].
Successful treatment of OKC using the technique of decompression and irrigation is based on a substantial reduction in cyst volume and a significant change in the character of the residual epithelium, which changes from a friable to a thick, robust epithelium with poor adherence to the adjacent bone, more closely resembling the oral epithelium or an inflammatory cyst [2]. This epithelial differentiation was observed in all patients included in the present study. It is believed that this change in the cystic epithelium after decompression results from the communication of the cyst with the oral cavity, thus inducing a chronic inflammatory response characterized by the presence of a lymphoplasmacytic inflammatory infiltrate and fibroplasia [2, 17, 18]. This epithelial differentiation was assumed by the authors to facilitate enucleation and curettage, which minimized the chance of incomplete removal of the cystic capsule, thereby reducing the recurrence potential.
Likewise, Pogrel and Jordan [19] reported 10 cases of OKC that completely resolved both clinically and radiographically after decompression, with a follow-up of 2.8 years; however, the recurrence rate was 12%, which is considered high. It is important to note that decompression should be used in a selected group of cooperative patients, since this type of treatment requires patient commitment during a prolonged period of time. Regular return visits are necessary to ensure cyst involution and the opportunity to provide appropriate treatment in the event of recurrence [5, 19, 20]. Therefore, this technique should be an option in cases where the initial goal is to reduce lesion size. Later, another treatment modality will be necessary for enucleation [5], because the protocol described here is multimodal.
The purpose of using enucleation combined with liquid nitrogen is to remove the visible lesion and to necrotize possible cell remnants by freezing, thus preventing possible recurrence. Liquid nitrogen has cell-necrotizing properties and preserves inorganic bone structures, unlike the Carnoy solution, which destroys osteogenic and osteoconductive properties [5, 14]. The use of liquid nitrogen has proven to be effective and well tolerated with few associated complications, which makes it an excellent option for the treatment of locally aggressive lesions, as an adjuvant therapy [4, 5, 14]. On the other hand, it was seen that the cryotherapy caused temporary paresthesia in two patients, which were spontaneous resolved. The authors are sure that the sensitive lost was caused by the liquid nitrogen because during the surgical treatment, one of the cystic cavity was in contact with the inferior alveolar nerve and the flap never was near the mental nerve in those cases.
Studies have shown that the most common postoperative complications associated with the treatment of OKC are paresthesia of the lingual nerve or inferior alveolar nerve, pathological fractures, and suture dehiscence [5, 20]. In the present study, as mentioned above, 2 patients had transient paresthesia of the inferior alveolar nerve the sensitivity returned spontaneously within 6 months of the surgical procedure and two patients had suture dehiscence, which was associated with the use of liquid nitrogen, a complication that has been previously reported in several studies as most of the common complications are associated with cryotherapy [5, 14]. Suture dehiscence was managed conservatively by mouth rinses with 0.12% chlorhexidine digluconate and the wound was closed in three weeks. Moreover, 2 patients lost the decompression device, but both of them sought care quickly, thereby not compromising the progress of the decompression process.
Pogrel [20] reported that leaving teeth associated with the cystic lesion may increase the recurrence rate due to difficulty in accomplishing enucleation and using cryotherapy during surgery in these cases. Conversely, the present study showed a case in which the tooth involved in the lesion was left in the area, with orthodontic traction during follow-up and absence of recurrence with more than 5-years of control. So, it is possible to believe that in some cases where the patient is engaged in his treatment and the surgeon is in constant contact with the orthodontist, the lesion impacting the tooth can be safe.
CONCLUSION
To date, no recurrence of OKC has been observed in any patient treated with the multimodal protocol described here. The study findings suggest that the treatment proposed for the management of OKC using the multimodal protocol based on decompression and irrigation, followed by enucleation and curettage combined with the use of cryotherapy was associated with zero rate of recurrence and low surgical morbidity, thus providing an excellent option for the treatment of these lesions. The benefit of this protocol over other conventional approaches [enucleation or en bloc resection] lies in the minimal surgical morbidity and the possibility to be performed under local anesthesia.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethical Review Board of Catholic University of Rio Grande do Sul, (CAAE: 30409320.1.0000.5336).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from each participant prior to the study.
AVAILIBILITY OF DATA AND MATERIALS
The data supporting the findings of this article is available in the Pontifícia Universidade Católica do Rio Grande do Sul (PUC-RS)’s Department of Oral and Maxillofacial Surgery.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

