All published articles of this journal are available on ScienceDirect.

Surgical Field Isolation Through Rubber Dam to Prevent COVID-19 Exposure During Tooth Extraction: Case Report
Abstract
Background:
At the beginning of 2020, a new pathogen named SARS-CoV-2 spread from China to the globe, becoming responsible for a potentially lethal acute respiratory syndrome: COVID-19. Direct contact and airborne contamination are the most frequent infection ways of SARS-CoV-2. During routine dental practice, SARS-CoV-2 transmission can occur through direct contact with mucous membranes, oral fluids, and contaminated instruments or inhalation of aerosol from infected patients.
Introduction:
Tooth extraction often involves exposure to blood and oral fluids, and the use of a rubber dam could be indicated to minimize direct contact and to decrease the amount of potentially infected droplets around the operatory field. The aim of this clinical case is to show how the use of a rubber dam could help in preventing or minimizing COVID-19 exposure during dental extraction.
Materials and Methods:
A 32-year-old patient reported severe pain and discomfort to an upper first molar due to a deep carious lesion and vertical tooth fracture. Under local anaesthesia, a rubber dam was placed, isolating the whole upper right sextant, and an atraumatic extraction was performed.
Results:
All three roots were intact, the bone septum was stable, and no oro-antral communication was present. A gauze swab was placed onto the socket and compressed slightly. After 5 minutes, the socket stopped bleeding, and both clamp and rubber dam, were removed.
Conclusion:
Within the limits of this single case report, the use rubber dam prior to tooth extraction could be a useful device to decrease aerosol spread and exposure to blood.
1. INTRODUCTION
In 2020, a new kind of virus spread from China to the entire globe, and in March 2020, the World Health Organization (WHO) officialised the pandemic status. This virus, named SARS-CoV-2, is a highly infective coronavirus responsible for a potentially lethal acute respiratory syndrome, named COVID-19 [1].
COVID-19 clinical manifestations especially include respiratory symptoms, fever and dyspnoea, and Sars-CoV-2 has a two weeks incubation period [2]. Direct and airborne contact contamination is the primary infection pathway of this coronavirus [1]. Direct infection is caused by contact of eyes, nose or oral mucosa with contaminated surfaces [3]; airborne contamination instead is due to aerosol exhaled through breath, cough or sneeze [1]. Moreover, it has been demonstrated that virus spread can also occur in patients with no clinical symptoms [4].
Health care professionals present the highest risk of contagion among professional categories [2, 3, 5]. Due to exposure to oral fluids, such as blood and saliva, and droplet production, dental practitioners, are at high risk of contagion during their usual practice [1, 6]. SARS-CoV-2 transmission during dental practice can therefore occur through inhalation of droplets from infected individuals, or direct contact of mucous membranes with oral fluids and contaminated instruments and surfaces [5, 7].
The aim of this case report is to show an expedient that could help in the prevention of COVID-19 exposure during dental extraction.
2. MATERIALS AND METHODS
A 32-year-old male patient, systemically healthy and light-smoker, was urgently referred to a private dental practice due to severe pain and discomfort to the upper right first molar.
After clinical and radiographic analysis, a deep carious lesion and a vertical fracture of the tooth were diagnosed, and tooth extraction was proposed. The patient gave written informed consent for the proposed treatment. Clinical procedures were performed in accordance with the Helsinki Declaration of 1975, as revised in 1983.
Under local anaesthesia, a rubber dam (Nic Tone, Expertech Solutions, Bucharest, Romania) was placed, isolating the whole upper right sextant and arranging the metal clamp on the second molar (Fig. 1).

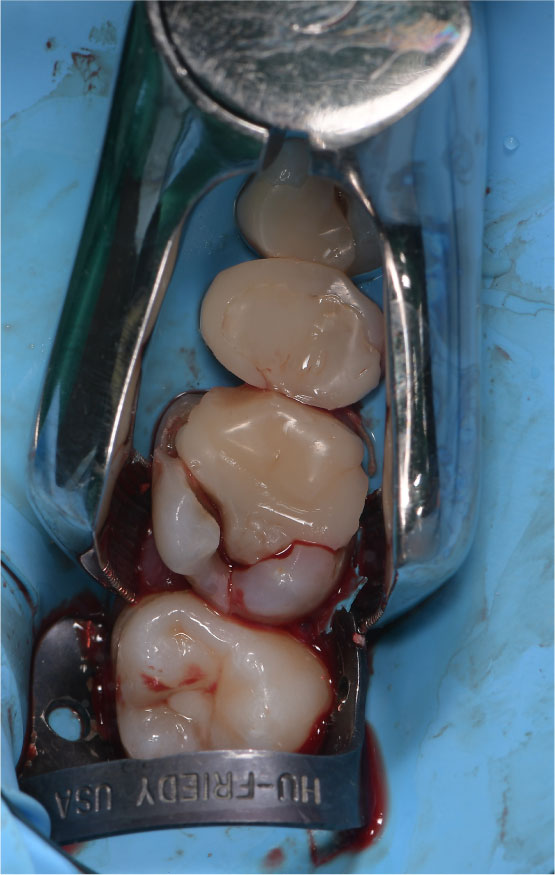
A gentle sindesmotomy with a periosteal elevator was performed, taking care not to lacerate the rubber dam. Once the tooth had been luxated and dislocated, an atraumatic extraction was performed with dental forceps, preserving the inter-radicular bone septum (Fig. 2). All three roots were intact, the bone septum was stable, and no oro-antral communication was present. The socket was finally rinsed with 0.20% chlorhexidine.
A gauze swab was placed onto the socket and compressed slightly in order to stop bleeding and wait for coagulation to occur (Fig. 3). After 5 minutes, the socket stopped bleeding and both clamp and rubber dam, were removed. Due to the complete absence of bleeding in the following 20 minutes, sutures were avoided, and the patient was dismissed.

In combination with a non-steroidal analgesic, amoxicillin with clavulanic acid was administered at a loading dose of 3 grams, followed by 3 grams daily for 4 days. Post-extraction instructions included a soft-food diet for 1 week and suitable oral hygiene, including twice-daily rinsing with a 0.2% chlorhexidine mouthwash. A follow-up visit was scheduled after 7 days.
3. RESULTS
Healing was uneventful-patient-reported no swelling, pain, nor bleeding. The use of a rubber dam could have decreased droplet spread and exposure to blood and saliva.
4. DISCUSSION
During the COVID-19 pandemic, great attention is placed on the research of devices and procedures able to reduce or eliminate potentially infected droplets spread into the environment.
To our knowledge, this is the first reported case with a rubber dam placement prior to tooth extraction. The use of rubber dam is quite common in restorative and endodontic dentistry because it permits operatory field isolation from oral fluids and permits correct disinfection and adhesive procedures [8]. A dental extraction is a common procedure that often involves intra-surgical bleeding and exposure to blood and oral fluids [9]. Moreover, in some cases, the tooth has to be sectioned with a handpiece, and this creates an aerosol spread made of air, water and contaminants. It has been shown that the use of a rubber dam is indicated to reduce significantly the amount of aerosol containing saliva and/or blood, obtaining a 70% reduction of droplets around the patient’s mouth [10]. Moreover, the isolation of the surgical field through a dental dam and the use of high-speed ejectors are able to reduce the amount of aerosol and are also able to make these droplets less contaminated. These aspects could become extremely useful in the prevention of airborne diseases, such as COVID-19.
CONCLUSION
Within the limits of this single case report, the use rubber dam prior to tooth extraction could be a useful device to decrease aerosol spread and exposure to blood. Since SARS-CoV-2 spread also happens in the absence of clinical symptoms, all patients should be treated as potentially infected, and routine use of the rubber dam during tooth extractions seems to be an ideal aid for the prevention of COVID-19 exposure.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Clinical procedures were performed in accordance with the Helsinki Declaration of 1975, as revised in 1983.
CONSENT FOR PUBLICATION
The patient gave written informed consent for the proposed treatment.
STANDARDS OF REPORTING
CARE guidelines and methodology were followed.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

