All published articles of this journal are available on ScienceDirect.

Comparative Analysis of Fracture Strength of Remaining Tooth Structure after Endodontic Treatment with Various Access Cavity Preparation Techniques
Authors Info & Affiliations
Abstract
Background:
A perfect balance needs to be maintained between various types of endodontic access cavity preparation designs like - Traditional and conservative designed preparation to have access to the root canal system for proper cleaning and shaping of root canals without compromising the fracture resistance of the tooth structure.
Aims and Objectives:
We aimed to assess as well as draw comparisons of resistance against fracture of remaining tooth structure post the endodontic treatment after preparing access cavity through a variety of techniques so that we can estimate which type of cavity design technique will help endodontically treated teeth to withstand excessive load without fracture.
Methods:
Forty-two intact teeth (mandibular molars) were randomly selected and then were assigned to 07 different groups, inclusive of control and test groups. Various designs of access cavity preparation were done on sample teeth. The groups were divided based on different access cavity preparation designs as well as residual walls. The samples were then mounted on a composite cylinder, which was loaded under a mechanical testing machine at 0.5mm/min speed till the tooth structure fractured. This measurement of force was denoted in newton. The later analysis was carried out with the help of two-way Analysis of Variance (ANOVA) as well as Tukey’s post-hoc statistical tests.
Results:
There was negligible statistically relevant variance in strength towards fracture between traditional and conservative designs in teeth having three remaining walls. However, teeth with only two remaining walls fractured easily.
Conclusion:
Fracture resistance of teeth with remaining 03 residual walls did not show any significant difference among Traditional (TEC) and Conservative Cavity (CEC) design groups, but increased fracture strength was reported in CEC with 02 residual walls.
1. INTRODUCTION
Vital teeth are much stronger in terms of fracture resistance, especially when bearing occlusal forces compared to root canal treated teeth [1]. A lot of factors cause the breakage of tooth structure and, in turn, weakening of the same [2]. Endodontic teeth generally dehydrate over time with changes in the crosslinking of collagen in the dentinal structure [3]. Consequently, it shows that teeth that are endodontically treated are far more brittle as compared to teeth that have not undergone endodontic treatment [4]. Endodontic teeth are fracture prone sue to caries, any traumatic event, or a combination of both, which leads to breakage of tooth structure [5]. Periodontal structure is also important to maintain the steadiness of the tooth as a whole, so if there is associated periodontitis, it is important to treat them as well so that tooth, as well as surrounding structures, are also in a sound anatomical environment.
Long-term survival is also jeopardized in the case of teeth that have been treated by root canal therapy; as they are more predisposed to breakage of the tooth substance [6].59.6% of root canal treated teeth are extracted due to fracture of the tooth walls, which results in a dramatic reduction of tooth structure as well as its functionality. Only 8.6% of cases are related to endodontic procedure failure of the affected teeth [7].
A major factor that influences fracture resistance of a tooth that has been endodontically treated is the type of access cavity preparation i.e. Traditional Endodontic Access Cavity preparation (TEC), which involves removal of excess of dentinal structure so that there is a much wider pathway for proper biomechanical preparation of canal. Nowadays, endodontically conservative access cavity preparation is preferred so that more amount of natural tooth structure is preserved and in turn increases the fracture resistance as well. This Conservative Endodontic Access Cavity (CEC) preparation comes under the minimally invasive dentistry concept which is extremely popular with various dental professionals [8].
CEC preparation consists of two types of access cavity preparation techniques endodontically; Ninja Endodontic Access Cavity (NEC) as well as Truss Endodontic Access Cavity preparation technique (TREC). In the Ninja technique, direct access to the root canal can be obtained with a prepared small occlusal orifice, but due to limited line of vision, incomplete removal of infected pulpal tissue is the main limitation leading to failure of endodontic treatment many times [9]. However, TREC usually consists of the removal of only pulpal tissue from the root canal rather than removing the entire pulp chamber roof. In this technique, endodontic access is gained through the occlusal aspect of the tooth by direct entry to the origin of the canal orifice. This technique conserves a lot of dentin structure but fails to comply with adequate canal shaping and preparation [10].
CEC has been a controversial technique, as many authors state that this type of conservative approach augments the fracture resistance of the tooth compared to the traditional method. But on the flip side, this technique also causes a lack of access for the instruments to effectively cleanse the root canals, especially distal ones in molars [11]. Caries usually causes loss of tooth structure, especially in case of residual caries in endodontically treated teeth. The case becomes trickier when there is a loss of more than one wall of the tooth structure, which has to undergo Root Canal Treatment (RCT) [12]. Very few studies have evaluated the resistance to fracture of teeth that have been subjected to endodontic treatment when using either NEC or TREC techniques. Hence, the purpose of our study was to assess the effect of damage to the residual wall of teeth which have undergone endodontic treatment, when TEC or CEC techniques are used which is important to understand further the concept of Minimally Invasive Dentistry (MID) in terms of endodontically treated teeth.
2. MATERIALS AND METHODS
The present study is an in-vitro study conducted in the Department of Conservative Dental Sciences, College of Dentistry, Prince Sattam bin Abdulaziz University, Al-Kharj, Saudi Arabia. This study has been independently reviewed and approved by the Institutional Review Board, College of Dentistry, Prince Sattam bin Abdulaziz University, Al-Kharj, with IRB number: PSAU2020024. Forty-two (42) intact teeth (mandibular molars) which were recently extracted for periodontal reasons were used in this study, they were randomly selected; it was ensured that the selected teeth did not have any cracks, fractures of crown and roots, even absence of carious or non-carious lesions like attrition, abrasion, and erosion. These teeth were obtained from the clinics of the oral and maxillofacial surgery department, College of Dentistry, Prince Sattam Bin Abdulaziz University, AlKharj, Saudi Arabia. They were cleaned by ultrasonic scalers and were stored in 10% neutral buffered formalin to prevent dehydration. The selected teeth were assigned to 7 different groups, inclusive of control and test groups as shown in Table 1. The selected teeth were almost comparably equal in size, shape, and anatomy and were randomly assigned to each group. In the control group, selected samples were not subjected to any sort of cavity designing having complete coronal structure intact.
| Access Cavity Design | No. of Samples (n=42) |
|---|---|
| Control specimens [Group I] | 2 |
| TEC [Group II] | 4 |
| CEC [Group III] | 4 |
| TEC + 3 [Group IV] | 8 |
| CEC + 3 [Group V] | 8 |
| TEC + 2 [Group VI] | 8 |
| CEC + 2 [Group VII] | 8 |
- Group 1= intact teeth which acted as a control
- Group 2= normal teeth where TEC design was made.
- Group 3= normal teeth where CEC design was made.
- Group 4= compromised teeth, where only three walls were remaining and then TEC design was made.
- Group 5= compromised teeth, where only three walls were remaining and then CEC design was made.
- Group 6= compromised teeth, where only two walls were remaining and then TEC design was made.
- Group 7 = compromised teeth, where only two walls were remaining and then CEC design was made.
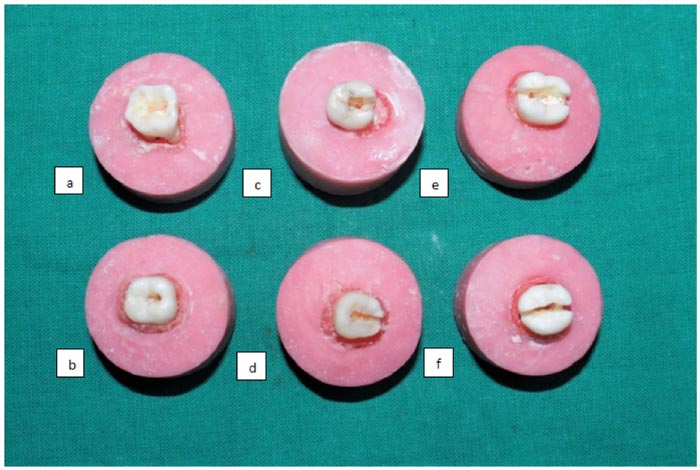
With the use of conventional round burs and high-speed tapered burs, access cavity preparation is done by de-roofing the pulp chamber in TEC. Irrigation with a 30-gauge needle was done using sodium hypochlorite 2.5% during canal preparation. Whereas conservative access cavity preparation was prepared using Clark and Khademi conservative access model as a general guide [13]. In this technique, a minimal amount of dentin is removed to locate canal orifices and preserve a tiny area of the dentinal roof of 0.5-3.0 mm around the entire pulp chamber and just wide enough to shape canals (Fig. 1).
The samples were mounted on a composite cylinder. A testing machine is then utilized where the specimen is analysed under the load (Fig. 2) At a right-angled inclination, the specimen is placed with the help of a holder inside the testing machine. At the central fossa, a standardized load is applied at an angle of 30 degrees, with a tip of 2mm of diameter at a speed of 0.5mm/min. In the load test, the values were recorded in Newton units of force.

2.1. Statistical Analysis
Shapiro-Wilk test was used to verify the normal distribution of the data. Two-way Analysis of Variance (ANOVA) test between various pairs as well as Tukey’s post-hoc test is employed for Statistical analysis in assessing the fracture resistance, where the level of significance is considered below 0.05.
3. RESULTS
The sample data in each group (mandibular molars) were evaluated for normal distribution and was found to be normally distributed or at least with few skewnesses using -Shapiro-Wilk normality test and therefore, the parametric tests (two-way ANOVA and post-hoc Tukey tests) were justified to compare data between groups and within groups.
Mean as well as standard deviations were measured for various groups, which were later considered for pairwise comparison with the help of ANOVA as well as post-hoc Tukey test (Table 2) For comparing various pairs in the study Tukey post hoc analysis was conducted, in which alteration was seen statistically in terms of resistance to fracture of the tooth structure between both traditional as well as conservative designs in teeth where only three walls were remaining, though conservative design still fared better before reaching their breaking point. However, having three residual walls were far better in terms of strength and ability to withstand the forces as compared to teeth where two walls remained in the coronal tooth structure. Consequently, teeth which had only two remaining walls fell drastically short on resistance to fracture, in TEC design as compared to CEC design (Table 3) This denotes that the presence of residual walls influences the amount of structure stability much more than the type of cavity preparation. Two-way ANOVA showed that the sound tooth sample (Group 1) was the strongest equated to various groups in the study where endodontic access cavity preparation was done on teeth (Table 4)
| Access Cavity Design | Mean | Standard Deviation |
|---|---|---|
| Group I | 1852.7 | 112.6 |
| Group II | 1172.6 | 262.4 |
| Group III | 1422.2 | 199.4 |
| Group IV | 1107.4 | 282.6 |
| Group V | 1314.8 | 170.5 |
| Group VI | 668.3 | 131.5 |
| Group VII | 698.5 | 121.8 |
Table 3.
| Comparison Between Various Groups | P value of Post-hoc Tukey Test |
|---|---|
| I-II | 0.011 |
| I-III | 0.04 |
| I-IV | 0.0355 |
| I-V | 0.0238 |
| I-VI | 0.047 |
| I-VII | 0.031 |
| II-III | 0.027 |
| IV-V | 0.543 |
| VI-VII | 0.021 |
4. DISCUSSION
There is a decrease in tooth structure strength when an extended design is prepared for endodontic access in root canal treatment. Hard tissue like dentin and enamel which provide walled support, provides strength to the tooth against both occlusal as well as other directional forces, removal of these will make the cusps vulnerable to fracture. This was evident in our study also, in teeth where less than three walls of the surrounding tooth structure were left, there was a phenomenal decrease in the strength of the coronal structure and thus will require increased efforts to restore the same. Consequently, it is suggested that a conservative design in comparison to a traditional design will help in strengthening the tooth structure as well as the long term prognosis of these endodontically treated teeth [14].
| Groups | P value of ANOVA |
|---|---|
| Group I | 0.03 |
| Group II | 0.0218 |
| Group III | 0.0167 |
| Group IV | 0.093 |
| Group V | 0.0867 |
| Group VI | 0.029 |
| Group VII | 0.013 |
Authors like Reeh et al. studied the effect of endodontic treatment on the occlusal loading on normal human teeth which were extracted, where it was determined that this kind of procedure leads to a reduction in stiffness of tooth structure by about 5% due to loss of occlusal strength. If there is a loss of any of the marginal ridges and a cavity is designed in the occlusal area, this might further reduce strength by around 20%. If both the mesial and distal marginal ridges are also involved along with an occlusal cavity preparation, then a 63% strength reduction is noted. So, this clearly shows that the presence of intact marginal ridges is extremely important in retaining the stability as well as strength and stiffness of the tooth structure as a whole, which was also supported by studies carried out by Oliveira et al. in endodontically treated premolar teeth [15].
In the case of endodontically treated teeth, authors had reasoned out that cuspal stability as well as flexural strength decreased when the extent of cavity preparation was increased. This, in particular, leads to more deflection of the cuspal structure leading to marginal leakage and, in turn, fracture of the tooth structure. It leads to the collapse of the load-bearing cusps [16].
Since there is a decrease in moisture content once a tooth is endodontically treated, it results in the structure of a tooth becoming susceptible to fracture. Few authors have suggested that it is because moisture content predominantly resides inside the dentinal structure which is compromised by access cavity preparation and the moisture reduction amounts to almost 9% [14]. But this view is not universal as many believe that a tooth doesn’t become brittle because of intrinsic factors, but it might be accompanied by other factors as well [17].
The dentinal structure must be maintained as much as possible, which has led to a concept i.e. MID; which provides strength and stability to tooth structure without compromising the quality of treatment. MID recently has led to the popularization of CEC which harps on the fact that a considerable amount of dentinal structure is preserved by avoiding de-roofing of the pulp chamber and only concentrating on removal of infected pulpal tissue without over-flaring of root canals, which helps to retain more dentinal structure in roots leading to the increased steadiness of tooth structure facing occlusal forces later on [18].
This conservative technique preserves pre-cervical dentine, which acts as support against fracture as well as tensional forces. Gates- Glidden burs as well as large round burs are avoided in this technique. But a major disadvantage is leaving out infected pulpal tissue as improper cleaning and shaping which leads to endodontic failure, so more studies are required to prove its effectiveness in root canal treatment. More time and experience are also required to achieve success through CEC, which also proves to be technique sensitive [19]. Our results were in line with a study conducted by Krishan R. et al., which demonstrated that conservative access cavity preparation was better in all posterior teeth, especially mandibular molars in terms of fracture load resistance. In the case of restorative composite resins, they restore the stability and fracture resistance of teeth where there is a loss of dentin around the cervical area to that of 72% of an intact tooth [19]. A trend has been popularized these days for making conservative cavity designs due to the use of advanced instruments like- Cone-beam computed tomography, Micro-Computed tomography, etc [20]. It is also imperative to mention that apart from the number of residual walls that influence the fracture resistance, other factors can also influence the long-term survival of endodontically treated teeth. One of the major factors is nearby periodontal support. In cases where existing periodontitis or endo-perio lesions are present, survival of a tooth, however meticulously restored, will not survive for long when encountering the masticatory forces. Periodontitis which is a chronic multifactorial disease [21], leads to disruption of the tooth-supporting tissues and finally causes tooth loss [22].
Many studies have indicated that around 60% of the stiffness of tooth structure is reduced when a mesial-occlusal-distal cavity is prepared which leads to damage to the marginal ridges which is essential for the toughness of the tooth itself. Recently it has also been observed that resistance to fracture is directly dependent on the amount of residual coronal dentin. It is imperative to consider the amount of marginal ridge loss when choosing a restoration for ensuring aesthetics as well as functionality for a longer period [23]. Studies by Rover G et al., and Moore B et al., have also demonstrated that in the case of maxillary molars resistance to fracture is similar in cases of traditional as well as conservative designs of access cavity [24, 25]. The whole point of access cavity design apart from the carious affected area, is to conserve dentin by leaving an area between two cavities if prepared so that the dentinal area gives the tooth, the necessary strength [26].
In the present study, loss of residual walls of the tooth structure accompanied by a different type of access cavity designs on tooth samples was evaluated. The preferred sample which was used in the study was Mandibular molars as these vertical fractures are most common if these teeth are undergoing root canal treatment. Correlating with the number of residual walls, it is imperative to note that excess dentine removal might compromise the fracture resistance of the tooth. However, a major limitation of in vitro studies is that they lack the simulation of the clinical environment as in a study setting, limited sample size is chosen and the environment is also controlled one [27].
However, CEC comes with its drawback also which is reduced access cavity preparation in conservative design, which in turn could influence the efficiency of root canal therapy [28, 29]. In particular, it could influence the possibility to detect root canals as well as the ability to complete removal of the pulp tissue, debris, and necrotic material [30]. Hence, an impeccable balance should be maintained between traditional as well as conservative design preparations, so that even in teeth where few coronal walls remain especially in endodontically treated teeth, the tooth can be restored to better strength and stability for long term survival.
CONCLUSION
The fracture strength of teeth with remaining 03 residual walls did not show any significant difference among TEC and CEC groups, but increased fracture strength was reported in CEC with 02 residual walls. Preserving some amount of coronal as well as pre-cervical dentin provides augmented fracture resistance to the tooth structure. A sense of balance should be maintained by the clinician between both the traditional as well as modern conservative designs, so that strength is maintained and should be less prone to fracture and ensure the stability of the tooth structure and ensure sterile environment inside the root canal.
LIST OF ABBREVIATIONS
| TEC | = Traditional Endodontic Access Cavity |
| CEC | = Conservative Endodontic Access Cavity |
| NEC | = Ninja endodontic access cavity |
| TREC | = Truss Endodontic Access Cavity |
| MID | = Minimally Invasive Dentistry |
AUTHORS' CONTRIBUTIONS
Mohammed Mustafa, Zaid A. Al-Jeaidi, Ali Robaian AlQahtani: Concept; Study design; Intellectual content; Manuscript drafting; Final manuscript approval including editing and reviewing.
Mohammed Ali Salem Abuelqomsan, Raneem Suleiman Alofi, Ziyad Ibrahim Alghomlas, Tameem Abdullah Alothman: Literature search; Data acquisition; Statistical analysis; Manuscript writing.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study has been independently reviewed and approved by the Institutional Review Board, College of Dentistry, Prince Sattam bin Abdulaziz University, Al-Kharj, Saudi Arabia, with IRB number: PSAU2020024.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2008 (http://www.wma.net/en/20activities/10ethics/10helsinki/).
CONSENT FOR PUBLICATION
All participants signed an informed consent regarding their participation in the study and their agreement regarding the publication of the data gained in the current study.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the finding of the present study are available from the corresponding author [M.M] upon reasonable request.
FUNDING
The present study was supported by the Deanship of Scientific Research, Prince Sattam bin Abdulaziz University, Al-Kharj, Saudi Arabia.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

