
Are Dental Students Aware of and Knowledgeable about COVID-19? A Questionnaire-based Investigation
Authors Info & Affiliations
Abstract
Background:
Coronavirus disease 2019 (COVID-19) is a major global concern.
Objective:
This study aims to evaluate the knowledge of dental students toward COVID-19 in a context of a health emergency.
Methods:
A questionnaire-based survey was drawn up in an online form, to investigate knowledge and awareness level about COVID-19 among dental students at Magna Graecia University of Catanzaro, Italy. The questionnaire contained socio-demographic questions and 12 questions about definition, contagiousness, symptoms, incubation, source of infection, routes of transmission, treatment and infection control practices related to COVID-19.
Results:
72 dental students responded to the questionnaire-based survey. The participants had 87.6% of the essential knowledge about COVID-19 and 56.9% of the participants had also already heard about similar respiratory diseases. However, only 50% of the responders perceived a greater risk of contagion for dentists than other health professionals.
Conclusion:
Italian dental students had a good level of awareness of COVID-19. The most positive attitude of participants was toward the period of incubation, route of transmission and treatment. The COVID-19 outbreak reminded us the importance of knowledge on cross-infection control. It is essential to further sensitize future dentists to not underestimate the risk of exposure to the virus in dentistry.
1. INTRODUCTION
Coronavirus disease 2019 (COVID-19) is a major global concern. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spread began in late 2019. This virus, previously known as 2019-nCoV, was isolated in Wuhan, Hubei province, China, in December 2019. Similar to other zoonotically transferred diseases, as Middle East respiratory syndrome coronavirus (MERS-CoV) and SARS-CoV, emerged in 2003 and in 2012, respectively, SARS-CoV-2 was probably hosted by bats and its transmission from other animals to humans has been well documented [1].
1.1. Epidemiology
At the time of writing this article, 28637 952 laboratory-confirmed human cases of COVID-19, with 917417 deaths, have been notified to the World Health Organization (WHO). Italy has registered one of the highest diffusion rates in Europe with 286297 infections and 35603 deaths [2].
1.2. Route of Transmission
Based on genetic and epidemiologic findings research, it is reported that the COVID-19 outbreak started with a single animal-to-human transmission, followed by a human-to-human diffusion mainly via respiratory droplets and contact transmission [3].
Since researchers have identified SARS-CoV-2 in the stool of patients from China and the United States, the risk of fecal-oral transmission is also been reported [4]. Controlling COVID-19 infection is extremely challenging as it, although symptomatic patients represent the main source of transmission, patients in their incubation period and asymptomatic patients are also carriers of SARS-CoV-2 [2, 5].
1.3. Incubation Period
SARS-CoV-2 has an estimated incubation period of 2 to 14 days (at 5 to 6 d on average). In potentially exposed persons, it is recommended to consider this time-lapse for quarantine and potential medical observation [6].
1.4. General Clinical Features
Although SARS-CoV-2 spread can happen asymptomatically, clinical manifestations may vary from the presence of usual symptoms, as dry cough (59–82%), fever (83–98%), shortness of breath (19–55%) and muscular ache (11–44%), to atypical symptoms, such as conjunctivitis, sore throat, diarrhea, vomiting, and fatigue. In about 80% of infected patients, mild respiratory infections have been reported, though about half will have pneumonia; another 15% of patients develop severe illness; 5% need critical care treatment. A small proportion of patients presented hemoptysis. Normal or lower white blood cell counts, thrombocytopenia, or lymphopenia, with the increased C-reactive protein level can be found in COVID-19 patients [7-9].
Rarely, SARS-CoV-2 can lead to severe respiratory problems, kidney failure or death [6-11]. Computed tomography in patients with pneumonia revealed ground-glass opacity and patchy shadows [12].
Hypogeusia and hyposmia have been reported in 5.6% and 5.1% of patients, respectively [13]. Complications may include respiratory distress syndrome, arrhythmia, and shock. These events, mainly associated with older age and the existence of underlying comorbidities, i.e. hypertension, diabetes, and cardiovascular disease, were related with poorer prognosis. The mortality rate is approximately 5.4% [7, 8, 10, 14].
1.5. Diagnosis
Centers of Disease Control and Prevention (CDC) suggested to health care professionals to reach both the upper respiratory tract and lower respiratory tract when specimens are taken. Diagnosis of COVID-19 pneumonia can be based on a combination of epidemiologic information (i.e. residence or travel experience in affected regions in the 14 days prior to symptom onset), clinical symptoms, computed tomography imaging findings, and laboratory tests. Reverse transcriptase-polymerase chain reaction (RT-PCR) tests are the main diagnostic standard. However, a single negative RT-PCR test result in potentially infected patients does not exclude COVID-19 infection. Serology tests may also be considered when RT-PCR is not available [15].
1.6. Treatment and Prevention
The current approach to COVID-19 is to control the infection source, also through the use of personal protection precaution to reduce the risk of transmission, and to provide early diagnosis, in order to isolate affected patients [8, 15].
Since there is currently no scientific evidence to recommend specific COVID-19 therapy, the importance of supportive treatment has been emphasized. In China and Italy, Tocilizumab, a humanized antiinterleukin-6-receptor (IL-6R) monoclonal antibody, has been intravenous experimentally administered in patients with COVID-19 with encouraging results [16].
WHO has issued recommendations for all healthcare professionals caring for patients with acute respiratory tract infections [17].
The use of standard precautions, including respiratory and eye protection, was recommended when treating patients with known or suspected COVID-19 pneumonia. However, the decision to remove precautions should be based not only on laboratory, radiological, and clinical evidence but also on the professional evaluation by specialized healthcare personnel [18].
1.7. COVID-19 and Risk to Health Care Workers
Unfortunately, Italy was distressed by a disruptive and rapid spread of COVID-19, also due to the relatively easy transmissibility. Since April 7, Italy is the second European country per incidence of COVID-19 with the highest official rate of deceased subjects worldwide [19]. Current observations suggest that those who are in close contact with symptomatic and asymptomatic COVID-19 patients are the class with the highest diffusion of the contagion. Indeed, according to the Italian National Institute of Health (Istituto Superiore di Sanità), healthcare workers are at higher risk of SARS-CoV-2 infection (https://www.epicentro.iss.it/coronavirus/).
It is not surprising that dental practitioners, due to the peculiarity of dental settings, seem to be exposed to a higher risk of contagion. Dental procedures potentially expose the professionals to contact with saliva, blood, contaminated instruments or surface, and to inhalation of droplets/aerosol from infected patients. Based on the above, recommended management protocols for dental practitioners, in terms of patient triage, patients’ entrance into the practice, dental treatment, and after-treatment management have been reported [10, 20, 21].
Indeed, “have the benefit of the patient as their primary goal” it is the main indication of the ADA code for dentists [22].
Recent evidence has suggested that preventive measures, such as preprocedural mouth rinses, considerably reduce the microorganism concentration in aerosol procedures [23].
Though the overall reduction in the time spent by patients, the protection of health care workers, and the search for asymptomatic SARS-CoV-2 positive patients are the main measures to reduce the risk of cross-infection, to date, the reduction of contagion risk during dental procedures remains a challenge for dentists [24, 25].
This questionnaire-based survey aimed to evaluate the current awareness and knowledge level of COVID-19 among dental students in an Italian university scenario. This investigation was conducted according to information and guidelines provided by WHO and CDC.
2. MATERIALS AND METHODS
Since March 9, 2020 students were exempted from attending dental school and affiliated hospitals, to contain COVID-19 diffusion. In this SARS-CoV-2 outbreak context, we developed a questionnaire-based survey in the online form, to investigate knowledge and awareness level of dental students about SARS-CoV-2. Study participants were recruited from among dental students at Magna Graecia University of Catanzaro, Italy.
The emails were sent to the institutional addresses of the students by the Dean of the School of Dentistry (LF) on April 5, 2020. A reminder was sent on April 10, 2020. The inclusion criteria were willingness to participate in the study, be able to answer an online survey, and complete it by the deadline of April 15, 2020.
The questionnaire, based on the information given by WHO and CDC for SARS-CoV-2 and COVID-19, contained socio-demographic questions and 12 questions exploring the knowledge about definition, contagiousness, symptoms, incubation, source of infection, routes of transmission, treatment and infection control practices related to COVID-19. The questionnaire also included questions used to test participants’ knowledge about the similitude of SARS-CoV-2 with SARS-CoV or MERS-CoV, and to quantify the perception in the exposure risk of dentists with that of other healthcare professionals. The survey was drafted in Italian language, but the English translation is available in Table 1.
| 1) What you identify with the acronym “SARS-CoV-2” ? | A) “Severe Acute Respiratory Syndrome Coronavirus 2” virus B) An influenza virus C) A disease caused by a coronavirus D) All the previous answers seem correct to me E) I don’t know Correct answer: A |
| 2) What you identify with the acronym “COVID-19” ? | A) A coronavirus B) Disease caused by an influenza virus C) Disease caused by SARS-CoV-2 D) All the previous answers seem correct to me E) I don’t know Correct answer: C |
| 3) Is COVID-19 a contagious disease? | A) Yes B) No C) I don’t know Correct answer: A |
| 4) What can be the symptoms of COVID-19? | A) Fever and cough B) Gastrointestinal symptoms C) Respiratory failure D) All the previous answers seem correct to me E) I don’t know Correct answer: D |
| 5) What is the period of incubation COVID-19? | A) 2-14 days B) 1 month C) 2 months D) 3 months E) I don’t know Correct answer: A |
| 6) What is the possible source of COVID-19? | A) Wild mammals (bats, etc..) B) Pets (dogs, cats) C) Farm animals (poultry and livestock) D) All the previous answers seem correct to me E) I don’t know Correct answer: A |
| 7) How is it transmitted COVID-19? | A) From one person infected to others, through interpersonal contacts B) Through contact with pets C) Eating oriental food D) All the previous answers seem correct to me E) I don’t know Correct answer: A |
| 8) Which of the following indications do you find useful in order to prevent the spread of the virus? | A) Wash your hands with alcohol-based disinfectant B) Cover nose and mouth when sneezing or coughing C) Avoid social contact D) All the previous answers seem correct to me E) I don’t know Correct answer: D |
| 9) How can patients currently be treated? | A) Non-specific drugs and supportive medical treatment B) Vaccination C) No treatment D) I don’t know Correct answer: A |
| 10) Have you ever heard of “SARS” and “MERS” ? | A) Yes, both B) No C) Only about SARS D) Only about MERS |
| 11) Are there similarities between “SARS-CoV-2” the viruses responsible for “SARS” and “MERS” ? | A) Yes B) No C) I don’t know Correct answer: A |
| 12) In the context of exposure to the risk of contagion for medical doctors, dentists and other health professionals, which of the following statements do you agree with? | A) Dentists are more exposed to the risk of infection than other health professionals B) Dentists are less exposed to the risk of infection than other health professionals C) Dentists are equally exposed to the risk of infection than other health professionals D) I don’t know Correct answer: A |
Google Form (G Suite for Education, Google LLC, Mountain View, CA, USA) was used to record the participants' responses. The data were exported to Microsoft Excel format (Microsoft Office 365 Education, Microsoft Corporation, Redmond, WA, USA) for analysis.
3. RESULTS
A total of 72 dental students responded to the survey. Table 2 shows the socio-demographic variables. The population study comprised 35 male (48.6%) and 37 females (51.4%). More than half of the respondents (58.3%) were under 25 years (42) and 30 of them (41.6%) were over 25 years of age. Out of the respondents, 8 students were in their first year (11.1%), 8 in second year (11.1%), 11 in third year (15.2%), 9 in fourth year (12.5%), 12 in fifth year (16.7%) and 24 in sixth year (33.3%).
Our results are summarized in Table 3. Overall, regarding questions exploring the knowledge about COVID-19, the participants had 87.6% of the essential awareness about the virus.
| Variables | Sub-Group | No. | % |
|---|---|---|---|
| Gender | Male | 35 | 48.6 |
| Female | 37 | 51.4 | |
| Age | < 25 | 42 | 58.33 |
| > 25 | 30 | 41,67 | |
| Academic year | 1 | 8 | 11.1 |
| 2 | 8 | 11.1 | |
| 3 | 11 | 15.2 | |
| 4 | 9 | 12.5 | |
| 5 | 12 | 16.7 | |
| 6 | 24 | 33.3 |
| Questions | Ans: A % |
Ans: B % |
Ans: C % |
Ans: D % |
Ans: E % |
Correct % |
|---|---|---|---|---|---|---|
| Q-1 | 76.4 | 0 | 1.4 | 22.2 | 0 | 76.4 |
| Q-2 | 31.9 | 0 | 56.9 | 11.1 | 0 | 56.9 |
| Q-3 | 100 | 0 | 0 | - | - | 100 |
| Q-4 | 27.6 | 0 | 5.7 | 66.7 | 0 | 66.7 |
| Q-5 | 100 | 0 | 0 | 0 | 0 | 100 |
| Q-6 | 97.2 | 0 | 1.44 | 0 | 1.44 | 97.2 |
| Q-7 | 100 | 0 | 0 | 0 | 0 | 100 |
| Q-8 | 0 | 0 | 5.6 | 94.4 | 0 | 94.4 |
| Q-9 | 97.2 | 0 | 1.4 | 1.4 | - | 97.2 |
| Overall correct (average percentage) | ||||||
| Q-10 | 56.9 | 1.4 | 41.7 | 0 | - | - |
| Q-11 | 81.9 | 0 | 18.1 | - | - | 81.9 |
| Q-12 | 50 | 5.6 | 44.4 | 0 | - | 50 |
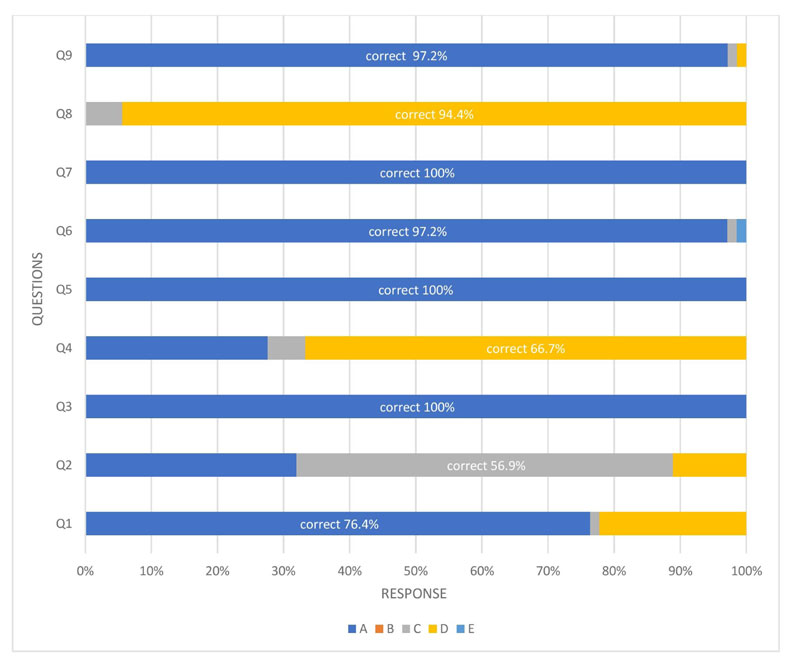
In particular, most of the total respondents (76.4%) were able to correctly define “SARS-CoV-2” acronym as a “severe acute respiratory syndrome coronavirus 2” and only 56.9% of the responders were aware that the term “COVID-19” indicate the infectious disease caused by SARS-CoV-2. About a third of the participants (31.9%) answered that the term “COVID-19” indicates a coronavirus. All respondents were aware that COVID-19 is a contagious disease.
A sizable proportion of the respondents (66.7%) knew COVID-19-related symptoms, such as fever, cough, respiratory failure, and gastrointestinal symptoms, and all the participants were aware that the period of incubation for SARS-CoV-2 is about 2–14 days.
Regarding the probable source of transmission, almost all respondents (97.2%) reported that the source of SARS-CoV-2 are bats, 1.4% thought that farm animals were the host of the virus and 1.4% were unable to respond.
The main mode of transmission of the virus occurs from one person infected to others, through interpersonal contacts, which were answered correctly by 100% of the responders. A majority (94.4%) of the responders were able to correctly answer questions related to COVID-19 prevention measures, while the rest believed that it was enough to avoid social contact to prevent the virus spread. Also, 97.2% of the students successfully answered that the use of non-specific drugs and supportive medical treatment are the only treatment available for patients with SARS-CoV-2 (Fig. 1). On questions regarding knowledge of similar respiratory virus, 56.9% of the participants had already heard of both “SARS” and “MERS”, 41.7% had only heard of “SARS”, while only 1.44% had never heard of either.
In the context of contagion risk perception for doctors, dentists and other health professionals, half of surveyed (50%) reported that the dentists are more exposed to the risk of infection than other health professionals; less than half (44.4%) reported that the dentists are equally exposed to the risk of infection than other health professionals; a minimum part (4.2%) answered that dentists are less exposed to the risk of infection than other health professionals.
4. DISCUSSION
Since its initial outbreak in Wuhan, China, at the end of December, the epidemic of COVID-19 has become a major challenging public health emergency, with a cascading effect worldwide [26].
Literature suggests that dental practitioners have a greater risk of transmission due to frequent aerosol-producing practices. Dental school and affiliated hospitals are also potentially contagion sites, and, in order to reduce their potential exposure, students were encouraged to take full advantage of online resources [20, 27]. Therefore, routine dental procedures have been suspended until further indications according to the real situation of disease and strict infection control [20, 21, 25, 28].
On March 20, 2020 the American Dental Association (ADA), teaming up with leading infection control experts from the Organization for Safety, Asepsis, and Prevention (OSAP), issued guidelines to provide the dental community with practical guidance and education during COVID-19 [29, 30].
The present survey attempted to evaluate future dental practitioners’ knowledge and attitude about COVID-19 in an Italian university scenario. We also assessed the perception of the risk of infection for dentists compared to the other health professionals.
To the best of our knowledge, this is the first study purely assessing the awareness of dental students about the global pandemic of COVID-19 and its impact on dentistry. Our study findings were compared with those of articles concerning the awareness of healthcare students and workers due to the limited number of publications on this topic. Consistently with our results, a prior questionnaire-based survey conducted in Mumbai Metropolitan Region among healthcare students and professionals, including a dentistry subgroup (students and faculty), demonstrated a high level of awareness [31].
Indeed, our study revealed that dental students at our University, regardless of gender, age and academic year, had a good level of awareness of the clinical aspects of COVID-19 as definition, contagiousness, symptoms, period of incubation, source of infection, transmission modes, prevention and treatment measures.
A careful analysis of the participants' responses showed that despite all participants knew that COVID-19 is a contagious disease and about 76.4% of respondents knew the definition of SARS-CoV-2, only slightly more than half of them (56.9%) knew that COVID-19 is the disease caused by SARS-CoV-2 infection. A not negligible percentage of the participants (31.9%) thought that acronym “COVID-19” indicated a coronavirus. On the other hand, a large percentage of respondents (66.7%) were aware of the symptoms of COVID-19 and all responded positively to the question about the period of incubation. This discrepancy could be due to a lack of clarity or attention when the terms “SARS-CoV-2” and “COVID-19” are used during the awareness campaigns and on the internet, which remains an important source of information. Researchers have documented that the disinformation of the COVID-19 health crisis produced by the media should be regulated by governments by developing strategies to regulate health information [32].
The major concentration toward the signs and symptoms and the incubation period of the disease is most likely related to their background, awareness campaigns and online activities that made them informed and prepared. It was also very encouraging to infer that participants were aware of the primary source of infection and the mode of transmission. These findings also revealed respondents’ awareness of the importance of following the instructions for protection and how these should be adopted to contain the human-to-human transmission of the virus. Almost all respondents (94.4%) were aware that hands washing with alcohol-based disinfectant, covering of nose and mouth during coughing or sneezing, and avoidance of social contacts represent the most important infection control measures. This response also confirmed that the dental students’ knowledge of newer infectious diseases was good, especially in the use of personal protective measures, isolation, and infection control practices. Our findings are similar to those reported in a study conducted among dentists about MERS, that showed a positive knowledge toward the use of barrier protection in healthcare infections context [33].
In general, our results showed an adequate knowledge toward the treatment of COVID-19 as 97.2% of the dental students answered that non-specific drugs and supportive medical treatment were the only treatment available for infected patients. These findings testified the effectiveness of educational information that students had received during COVID-19 outbreak and that had improved their knowledge, skills and attitudes.
When knowledge about similar respiratory diseases, like MERS and SARS, was investigated, participants were less knowledgeable. We found that only slightly more than half of the participants had already heard of both, but 81.9% of the respondents identified that there is a similarity of SARS-CoV-2 with these diseases. This response is in contrast with than reported by Kharma et al. among dental students from Al-Farabi Colleges, Jeddah, Saudi Arabia, during the outbreak of MERS-CoV [34].
There is a need to improve attitudes of dental students on this topic, therefore, we suggest providing more information on respiratory diseases like SARS and MERS, even in countries that have not been affected by these diseases.
When risk perception toward healthcare personnel has been quantified, we found that only 50% of attendees assumed that dentists are more exposed to the risk of infection than other health professionals. Almost half of them, 44.4%, showed a decreased awareness that, due to the peculiar characteristics of dental measures, in which aerosols and droplets could be produced, the risk of cross-infection can be higher for dental practitioners than other health professionals [20].
Despite strong evidence suggests that the dental professionals pose a greater risk for transmitting illnesses due to peculiar dental settings, these data showed that many future dentists underestimate the risk of exposure to the virus in dentistry, compared to other health professions.
The most positive attitude of the participants in this study was toward the period of incubation, route of transmission and treatment, when dealing with SARS-CoV-2 patients. So, this indicates that the information related to the way of contamination and spreading of infection is well documented.
In addition to causing significant global challenges for health systems, SARS-CoV-2 also made it necessary to seek accurate information regarding this issue. As reported by recent studies, primary sources of information about COVID-19 are news media as TV/video, magazines, newspapers, radio, and social media (Facebook, Twitter, WhatsApp, YouTube, Instagram, Snapchat) [35]. However, as there is a vast array of unverified malicious information on the internet, we find it helpful for students to carefully evaluate information related to COVID-19 and also use scientific and authentic content as sources of information.
Our results indicate that participants had good knowledge about COVID-19, but also suggest the necessity for further continuing education in dental school, as well as improving public education about COVID-19 control. The SARS-CoV-2 outbreak and the increasing number of dental practitioners affected remind us of the need to acquire the basic information of infection control, which is the main principle for protection.
The main drawback of our survey is that most participants are from urban locations in an Italian Region and do not truly represent the dental students of the entire country.
CONCLUSION
The COVID-19 pandemic has induced an unprecedented deferment of dental procedures. Students from Dental School at the Magna Graecia University of Catanzaro showed adequate knowledge and positive attitude of COVID-19 with an overall percentage of 87.6% correct answers. Still, we found an underestimation of the dentists' risk of infection compared to other healthcare professionals.
This study confirmed that realizing educational interventions could be needful to create more awareness of COVID-19 among the dentists of tomorrow.
AUTHORS' CONTRIBUTIONS
F.B.: Conception and design of the study; Acquisition of data; Analysis and interpretation of data; Drafting the article
C.B.: Conception and design of the study; Acquisition of data; Analysis and interpretation of data; Drafting the article
L.F.: Final approval of the version to be submitted; Revising the article critically for important intellectual content
A.G.: Final approval of the version to be submitted; Revising the article critically for important intellectual content
F.B. and C.B. contributed equally to this manuscript
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The ethical approval for this study was obtained by the Ethical Review Board of Central Calabria (reference for Magna Graecia University of Catanzaro), Italy with protocol number 169/2020.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Students' consent was acquired digitally at the time of participation in this survey.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author [L.F] upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

