All published articles of this journal are available on ScienceDirect.

Different Treatment Modalities followed by Dental Practitioners for Ellis Class 2 Fracture – A Questionnaire-based Survey
Abstract
Introduction:
Dental trauma is one of the most commonly seen injuries involving teeth and surrounding structures. The frequent causes of dental trauma are usually falls, traffic accidents, fights and sports injuries. Rapid treatment can prevent long-term damage to the orofacial structures and save the teeth. Ellis class 2 fracture is classified as the involvement of enamel and dentin excluding pulp. Dental practitioners are used to treating Ellis class 2 fracture very often in their dental practice and is usually considered as a dilemma among dental practitioners for the different treatment modalities followed for treatment of Ellis class 2 fracture. A survey is done among dental practitioners to assess the different treatment modalities followed by them in the case of Ellis class 2 fracture.
Materials and Methods:
A survey was done among 380 dental practitioners in the Chennai region in which 360 dental practitioners responded. The survey was distributed through electronic media and other means of communication. The survey data was collected, analysed and interpreted.
Results:
The results suggested that about 90% of dental practitioners had adequate knowledge and attitude towards the management of dental traumatic injuries. However, the practical application of the different treatment modalities was seen to be varied among dental practitioners. Based on this survey it was clear that majority of the dental practitioners in Chennai have good knowledge, attitude but there was a lack of clinical practice regarding the different treatment modalities followed by general practitioners for Ellis class 2 fracture.
Conclusion:
The survey shows that dental practitioners have a sound knowledge, attitude, but the practical application of the various treatment modalities available was seen to vary among various dental practitioners for Ellis class 2 fracture.
1. INTRODUCTION
Dental trauma is one of the most commonly seen injuries in the general population involving teeth and other surrounding structures. It has been observed that one in ten children suffer injuries related to the mouth and teeth that later require dental intervention. Rapid treatment can prevent long term damage to the orofacial structures and save the teeth [1]. The frequent causes of dental trauma are usually falls, traffic accidents, fights and sports injuries. Dental trauma commonly involves enamel, dentin and sometimes pulp or in some cases other orofacial structures [2]. In 1970, Paediatric dentist G.E. Ellis was the first person to promote a universal classification of dental injuries which is used now most commonly for traumatic injuries [3]. After the advent of Ellis Classification, World Health Organisation (WHO) developed a classification in 1978, which is almost similar to Ellis Classification, but it avoids the use of eponyms and therapeutic considerations [4]. It was used only for descriptive purposes and used mostly by Health professionals of other fields [5].
In 1981, Anderson et al [6] observed that children are most commonly affected by dental trauma. It was seen in their study that 25% of all school children experience dental trauma and 33% of adults have experienced trauma to permanent dentition, with most injuries occurring before age nineteen [7]. Ellis Class 2 fracture is a borderline injury and is considered as a dilemma for conventional restoration or other treatments such as conventional root canal treatment among many dental practitioners. It is seen that the incidence of dental caries is much higher in a person under dental trauma than a normal individual [8]. Murchison et al. demonstrated that the presence of unfavourable fracture pattern which when restored, exhibits low resistance to labially applied forces that mimic trauma force vectors and may exhibit higher resistance to horizontal traction forces that occur with incising or tearing food [9]. Different treatment modalities are used for Ellis class 2 fracture, the most common being conventional restorations, reattachment of fractured segments and placing full veneer crowns [10]. People with Ellis Class 2 Fracture show some signs of sensitivity due to the exposure of dentinal tubules and approach the dentist, so it is of prime importance that the dentist have adequate knowledge and clinical experience on how to treat them. The aim of this study was to conduct an observational qualitative questionnaire-based survey among general dental practitioners residing in the Chennai region for different treatment modalities followed by dental practitioners for Ellis class 2 fracture.
2. MATERIALS AND METHODS
2.1. Study Design
An observational, qualitative, questionnaire-based online survey was conducted from the time period of July 2018 to September 2018.
2.2. Sample Size
Calculation was done using a survey sample size calculator with a 95% confidence interval. Sample size was calculated in which from 380 dental practitioners only 360 practitioners responded who were practicing in the region of Chennai with an estimated 15% dropout.
2.3. Participants
The database for dental practitioners in the Chennai region was collected from Indian Dental Association were only general practitioners were included excluding specialists. Participants were not selected based on experience and the participants entered the study voluntarily. The study objectives and rationale were provided in the questionnaire itself.
2.4. Questionnaire
Although most of the dentists receive a similar training obtained from dental schools, their attitude towards clinical decision making and diagnosis makes a significant difference. Questions were asked to evaluate the diagnostic aspect, about the different restorative material as well as the frequently used treatment modalities by different dental practitioners which consists of a total of 23 questions of which 8 questions were based on knowledge, 7 questions were designed to check the attitude and the remaining were designed to evaluate the clinical guidelines followed by them. The questionnaire comprised of 2 sections with the first section assessing the demography of the respondents and the second section assessing the knowledge and approach towards Ellis class 2 fracture. The questionnaire was distributed through online media via Google forms. The survey data was then analysed and interpreted.
3. RESULTS
The data were collected from equal proportion from both the gender with 182 (50.8%) female and 179 (49.2%) male dental practitioners. The results of the survey are given in Table 1.
| Questions | Options | Percentage of Respondents |
|---|---|---|
| 1) Have you encountered Ellis class 2 fracture in your dental practice? | Yes | (67.5) |
| No | (15.3) | |
| Sometimes | (17.2) | |
| 2) Which is the most commonly encountered age group presenting with dental trauma in your practice? | Toddler (1-2 years) | (1.4) |
| Pre-schooler (3-5 years) | (12.2) | |
| School aged Child (6-10 years) | (43.6) | |
| Adolescence (11-17 years) | (28.6) | |
| Adults (18-40 years) | (12.5) | |
| Others – Population above the age of 40 years | (1.7) | |
| 3) Incidence of Ellis Class 2 Fracture is seen most commonly in which population? | Male | (85.8) |
| Female | (14.2) | |
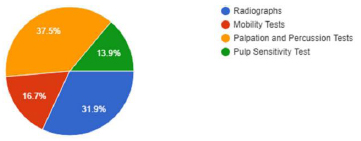
| 4) Which is the most commonly used clinical aid in the case of Ellis Class 2 Fracture? | Radiographs | (31.9) |
| Mobility Tests | (16.7) | |
| Palpation and Percussion Tests | (37.5) | |
| Pulp Sensitivity Test | (13.9) | |
| 5) Which of the following diagnostic aid do you most commonly use in the case of Ellis Class 2 Fracture? | Visual Inspection only | (12.8) |
| Visual Inspection and Tactile examination | (51.1) | |
| Pulp Sensitivity Tests | (29.4) | |
| Transillumination Tests | (6.7) | |
| 6) Which pulp sensitivity test do you think will be accurate for the diagnosis of Ellis Class 2 Fracture? | Heat Test | (23.3) |
| Cold Test | (35.3) | |
| Electric Test | (38.3) | |
| Test Cavity | (3.1) | |
| 7) According to you, do you think vitality tests show accurate results when a patient presents to immediately with Dental Trauma? | Yes | (34.2) |
| No | (31.7) | |
| Sometimes | (34.2) | |
| 8) Do you think there is a chance of pulp necrosis when a patient presents to you with Ellis Class 2 Fracture? | Yes | (38.1) |
| No | (19.7) | |
| Sometimes | (42.2) | |
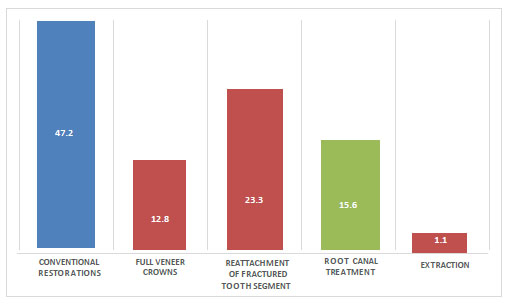
| 9) Which of the following is the most preferred treatment option to you in managing and Ellis Class 2 Fracture? | Conventional Restorations | (47.2) |
| Full Veneer Crowns | (12.8) | |
| Reattachment of fractured tooth segments | (23.3) | |
| Root Canal Treatment | (15.6) | |
| Extraction | (1.1) | |
| 10) Which type of composites do you most commonly use in your dental practice? | Conventional/Midfill Composites | (41.1) |
| Microfill Composites | (20) | |
| Hybrid Composites | (21.9) | |
| Nanofill Composites | (14.2) | |
| Others – Recent advancements such as microhybrid composites | (2.8) | |
| 11) What are the different isolation methods used in your practice for Ellis Class 2 Fracture? | Cotton Roll Isolation | (35) |
| Suction Tips and ejectors | (31.4) | |
| Rubber Dam | (31.7) | |
| None | (1.9) | |
| 12) Do you use PTFE Tape in your practice? | Yes | (18.1) |
| No | (20.3) | |
| Sometimes | (38.1) | |
| Never used | (23.6) | |
| 13) In your experience, what do you think is the longevity of composite restorations in Ellis Class 2 Fracture? | 1-2 years | (10.8) |
| 3-5 years | (42.2) | |
| 6-8 years | (33.3) | |
| 14) How often does patients present to you with a fractured tooth segment? | Above 8 years | (13.6) |
| Most of the time | (33.6) | |
| Sometimes | (57.8) | |
| Never | (8.6) | |
| 15) What is the prognosis/success rate of the reattachment of the tooth segment? | Good prognosis | (38.1) |
| Fair prognosis | (49.7) | |
| Poor prognosis | (2.2) | |
| 16) Which reattachment technique do you most commonly follow? | Enamel Beveling followed by luting the segment | (47.2) |
| Internal Enamel grooving followed by luting the segment | (20) | |
| Internal Dentin grooving followed by luting | (18.6) | |
| Over contouring the reattached segment | (6.9) | |
| Simple reattachment only | (7.2) | |
| 17) Why is bevel placement necessary for the reattachment procedure? | Improves the bonding surface | (26.9) |
| Reduces the microleakage | (10.6) | |
| Removing the unsupported Enamel | (10.8) | |
| Aesthetics | (7.8) | |
| All the above | (43.9) | |
| 18) Which material do you most commonly use for the adhesion of the fractured tooth segment? | Light Cure Composites | (60) |
| Chemically cured Composites | (16.1) | |
| Resin modified GIC/Luting GIC | (18.9) | |
| Dental adhesivesonly | (5) | |
| 19) Do you use dental adhesives in combination with a luting agent for tooth reattachment technique? | Yes | (40) |
| No | (26.7) | |
| Sometimes | (33.3) | |
| 20) Which etching technique do you most commonly use? | Etch and Rinse, Total etch 2 Step technique | (67.5) |
| Self- Etch Technique | (21.1) | |
| Selective Etch Technique | (11.4) | |
| 21) How long is the etching process carried out? | 20 sec for Enamel, 1 sec for Dentin | (22.8) |
| 30 sec for Enamel, 1 sec for Dentin | (30) | |
| 20 sec for Enamel, 2 sec for Dentin | (28.1) | |
| 30 sec for Enamel, 2 sec for Dentin | (16.4) | |
| Others | (2.8) | |
| 22) In your practice, how long do you cure the bonding agent after application? | 5 secs | (10.8) |
| 10 secs | (31.9) | |
| 15 secs | (36.1) | |
| 20 secs | (21.1) | |
| 23) Does RCT show a better success rate for the management of Ellis Class 2 Fracture? | Yes | (35.6) |
| No | (21.9) | |
| Sometimes | (42.5) | |
4. DISCUSSION
These results indicate that Ellis Class 2 fracture is one of the most common types of dental traumatic injuries seen in dental practice. The most risky age groups include children below the age of 18 years with school-aged children being more common. This correlates with the literature reported by Anderson et al. [11]. Their epidemiological study reported that oral injuries are most commonly seen in children below the age of 10 years and rarely seen below the age of 30 years. In various studies done by different practitioners for dental traumatic injuries, it is seen that boys are most commonly affected by dental trauma than girls [12]. This can be due to the reason that since boys are more involved in a variety of events such as accidents, falls, they are exposed to increased risk of trauma [13].
The diagnosis of dental trauma is carried out mostly by visual examination which is used for the evaluation of the wide amount of cases of dental trauma and it goes in correlation with percussion tests for the evaluation of any dental injury [14]. The next set of diagnostic method most commonly used is pulp sensibility tests (Fig. 1). Most clinicians tend to use thermal and electrical stimuli during examination following trauma to determine the health status of the pulp. In an event of dental trauma, an injury to the nerve fibres of a vital tooth with good vascular health tend to give a nonvital reading. It is recommended that endodontic therapy should be delayed on the traumatized teeth, and the affected pulp tissue should be considered vital unless apical radiolucency or sinus tract starts to develop [15]. These tests are set to have a different time interval of six weeks to three months. The electric pulp tester during an event of dental trauma is said to show inaccurate readings or no reading at all [16]. A study done on fifty-five individuals with Ellis class 2 fracture was assessed. It reported that 95% of the traumatized teeth showed positive response during the first examination following trauma, followed by which within the initial three months the teeth gave a negative response and at the end of six months a total of six teeth showed a negative response. This determines the fact that the vitality test soon after trauma has almost negligible validity [17].
According to Fig. (2) it is observed that conventional restorations is a much more preferred treatment option compared to other treatment modalities since composite restorations are very much developed which give aesthetics and functionality in considerable detail. Different types of composites are available for the restorative procedure such as microfine composites, densified composites, Fiber-reinforced composites, etc., the most recent being nanotechnology derived composites to have a resin size of 25 nm. The use of tints and translucent composites is useful for the accurate replication of incisal edges [18]. It has been observed that microfill composites finish with a high degree of smoothness and surface becomes smoother with time whereas hybrid composites, when compared to microfill composites, are less aesthetic and are used in a wide range of cavities such as Class 1, 2, 3 or 4 restorations [19].
Reattachment of the fractured tooth segment is quite often used for the treatment of Ellis Class 2 Fracture. Various studies [20-23] show that reattachment of the fractured tooth segment is said to provide adequate, long-lasting aesthetics as well as conservative, cost-effective treatment option [20]. A clinical case report showing the conservative and aesthetic reattachment of Ellis class 2 fracture showed a high prognosis [24]. These tooth fragments are usually attached with the total etch technique in which a protocol of 30 seconds etching is done for enamel and 15 secs for dentin while 37% orthophosphoric acid being the most commonly used etching agent [21]. Saliva is one of the factors to be considered in the process of reattachment. It is seen in cases of complicated tooth fractures saliva contaminates the fracture line and hinders the bond to form with each other [25]. Different process is used for the attachment process some of the examples being enamel bevelling, internal dentin groove, over contouring and simple reattachment.
The enamel bevelling is done to improve the retention and acid etching process. The internal dentin groove is also used but having a disadvantage in which it modifies the shade of the tooth. The next type of tooth segment reattachment is by over contouring in which the tooth segment is bonded to the fractured structure and prepared superficially of 0.5mm and cured with a thin layer of composite which removes the marginal lines from the restoration causing it to be highly aesthetic [26].
Due to the recent improvements in the adhesive system, the current treatment modality is to reattach the tooth structure to the fractured part without any preparation though it has a disadvantage that the aesthetics is not optimal compared to other type of methods. It can be used in combination with other techniques as well such as with internal dentin grooving [25]. Another newly used reattachment technique is the use of Er:YAG and Nd:YAG lasers in fragments reattachment of the fractured anterior tooth with pulp exposure. It was seen that the use of laser technology is used for the treatment of traumatic anterior teeth injury with the increase in the aesthetic result, patient comfort, and the quality of restoration [27, 28].
Enamel Bevelling followed by luting of the segment is done possibly due to the fact of limited knowledge in this field. Bevelling of margins is said to appear to reduce the marginal microleakage of fissure sealants [29]. Bevelling the enamel margins is an interesting alternative because this procedure makes the enamel prisms more reactive to conditioning, and consequently increases the bonding performance of the self-etch adhesive [30]. The adjuvant use of Polytetrafluoroethylene (PTFE) Tape which found its way into dentistry has a wide variety of applications some of it being as a barrier material for healing site to promote bone tissue formation, for adhesive dentistry which is seen for the restoration of anterior teeth by using composites restorations, another being protection of implant abutment screws during sealing, as a barrier between the assess cavity and root canal system [31].
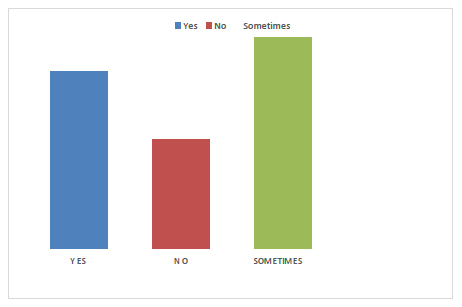
Endodontic Therapy is another preferred treatment option among the general practitioners Fig. (3) which is done possibly due to consideration of the formation of pulpal necrosis [32]. Ravn [33] conducted a follow-up study in which he observed that pulp necrosis occurred in 250 teeth in which 3.2% of the study subjects had enamel-dentin fracture as the only damage. Pulpal necrosis acts as a harbour for various types of microorganisms such as Bacteroides, Corynebacterium, Peptostreptococcus and Fusobacterium species [34]. In accordance with the study conducted, general dental practitioners in Chennai have sound knowledge on the overall diagnosis and management of Ellis Class 2 Fracture. The reason could be the knowledge gained during their undergraduate program and the awareness and information available through various sources. However, the application of the acquired knowledge and the protocols to be followed such as other treatment modalities than conventional restorations using tooth coloured remains quite satisfactory. This may be possibly due to the lack of knowledge on the different treatment modalities and lack of guidance and practice in this aspect. Creating awareness by means of CDE programs, demos and workshops on practical management of Ellis Class 2 Fracture could be considered beneficial.
5. LIMITATIONS
In accordance with the study conducted it can be seen that the study was focused on general dental practitioners practicing in the Chennai region. A comparative evaluation between the general practitioners and specialists would have shown a higher significance between the two groups
CONCLUSION
Based on this survey it can be concluded that many of the general dental practitioners in Chennai region have good knowledge, attitude and practice management of the different cases of Ellis Class 2 Fracture. There are variety of treatment modalities available for the treatment of Ellis Class 2 Fracture but according to the survey data acquired, many of the dental practitioners adhere to the conventional option rather than exploring the newer treatment possibly due to fact that they are unaware of the other treatment modalities or the lack of exploration of other methods of treatment.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Saveetha Research Committee, India with the clearance number of SDC/MDS/18-19/0012.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
All the participants of the study signed a general consent form.
AVAILABILITY OF DATA AND MATERIALS
The data analysed during the current study are available from the corresponding author upon request.
FUNDING
None
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

