All published articles of this journal are available on ScienceDirect.

Evaluation of the Effect of Various Powers of the Diode Laser in Microcrack Formation in the Wall of the Dental Root Canal by Scanning Electron Microscope (SEM)
Abstract
Background:
The laser is utilized for the removal of the smear layer, cleaning and disinfecting the dental canal. Recently, diode laser has been offered with a wavelength of (635-980nm) for cleaning and disinfecting the dental root canal.
Objective:
There is not adequate evidence for microcrack formation when using diode lasers with different powers. Therefore, the present study was conducted in order to analyze various powers of a diode laser in microcrack formation in dental root canals.
Methods:
In this experimental study, 100 mandibular incisor teeth that were extracted because of periodontal disease were selected. Using stereo-microscope, the presence of crack and fracture of the root was evaluated before and after canal instrumentation. Then, samples were randomly divided into 10 groups (10 samples in any group) based on different powers of laser and canal to be humid or dry under laser radiation. The laser was utilized for 10s puls within three iterated times. The samples were cross-sectioned after disinfection with a diode laser at 3 and 6mm length from the dental apex. Sections were observed under a scanning electron microscope and images were taken.
Results:
The frequency of microcracks is increased at the distance of (3-6mm) from the dental apex by an increase in laser power level from 2 to 4w (P<0.05). Similarly, results showed that the probability of microcrack formation under dry condition than the humid condition at the distance of 3mm from the dental apex might increase to 6.606 times and at the distance of 6mm from the dental apex increase to 4.978 times more.
Conclusion:
The optimal power of diode laser in the wavelength of (980nm) for cleaning and disinfecting of the root canal with the minimum damage on hard periodontium tissue is 1.5w.
1. INTRODUCTION
In recent years, various lasers have been introduced for applications in dentistry, such as in accelerating orthodontic tooth movement and for the Treatment of Lateral Periodontal Cysts [1, 2]. One of these applications is the use of laser in the dental root canal. The main objective of dental root canal preparation is the removal of microorganisms, smear layer, and canal enlargement that enables canal filling material to reach to the end of the root [3]. The laser is utilized for the removal of the smear layer, cleaning and disinfecting the dental canal [4-6]. Recently, diode laser has been offered with a wavelength of (635-980nm) for cleaning and disinfecting the dental root canal [7]. The application of diode laser in root canal treatment is an increase because of its disinfection property [8].
A vertical root fracture is one of the complications in dental root canal treatment that has a poor prognosis and leads to tooth extraction or cutting dental root [9, 10]. Findings of a study done by Yamazaki et al. have shown that using Er-Cr: YSGG laser for disinfection in dry root canal causes microcrack [11]. Nevertheless, there is no adequate evidence for microcrack formation during using diode lasers with different powers. Similarly, the findings of another study indicated that any diode laser might create small thermal changes at the external root surface, although water temperature might rise up to 30°C during the utilization of laser, the temperature of the external root surface would finally rise 4°C higher. Thus, using this laser will not lead to an adverse thermal effect on dentin [12]. Likewise, the results of a study by Ribeiro et al. showed that an increase in temperature caused by diode laser did not exceed the safety limit and did not damage periodontium. SEM analysis indicated melting in Groups 2 and 3 compared to the control group in the dental apical region. Generally, diode laser may be used for root canal treatment according to the measurement parameters [13].
Given the mentioned issues, there is not adequate evidence for microcrack formation when using diode lasers with different powers. Therefore, the present study was conducted in order to analyze various powers of a diode laser in microcrack formation in dental root canals for cleaning and disinfection of root canal with the minimum damage in hard tissue surrounding the root. The null hypothesis stated the inability of laser in disinfecting the root canal.
2. MATERIALS AND METHODS
This study was an in vitro experimental research. In this study, the samples were selected and were divided randomized into 10 sampled groups. The inclusion criteria were mandibular incisor teeth that extracted because of periodontal disease and the presence of at least 10 samples in each group, therefore the total sample size was 100 teeth. Teeth were kept in distilled water during the study period. To ensure from teeth to be a single root canal, mesiodistal and buccolingual angles radiographic images from teeth were taken. The exclusion criteria were open apex teeth, teeth with the curved canal, multi-canal teeth, and teeth with decayed root, teeth with the calcified canal, teeth with internal and external root resorption and teeth with cracks along the root. Decoronization of single-canal teeth was done under water cooling with a low-speed diamond disk, maintaining 16 mm from the apex.
Using a stereomicroscope (Olympus BX43; Olympus Co, Tokyo, Japan) at X25 magnification, the presence of crack and fracture of the root was observed for any sample. The cementum layer of the root was covered with silicon impression material as periodontal ligament space and then all roots were placed in acrylic blocks [14]. Patency and working length from the anatomic foramen of each canal was done with file NO#8 (Dentsply Maillefer, Ballaigues, Switzerland). The final working length was determined by decreasing 1mm of working length. Rubber stop, to prevent from motion, was fixed with composite resin.
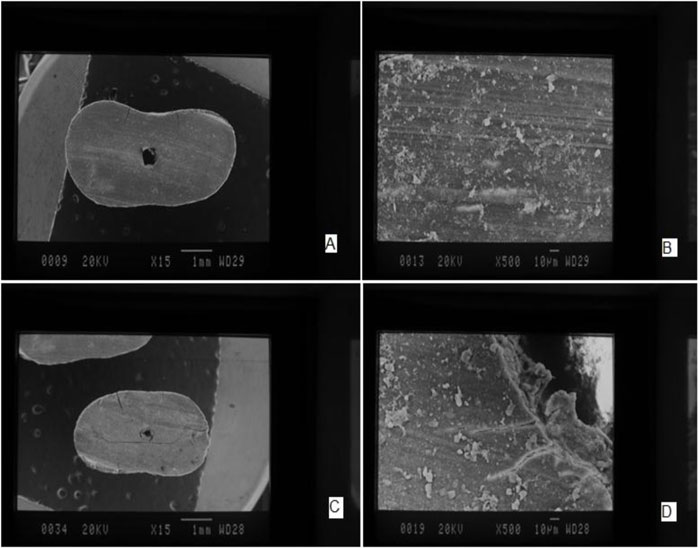
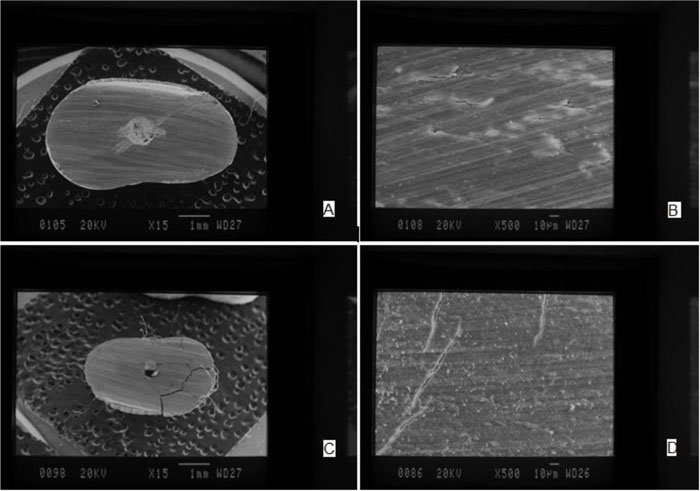
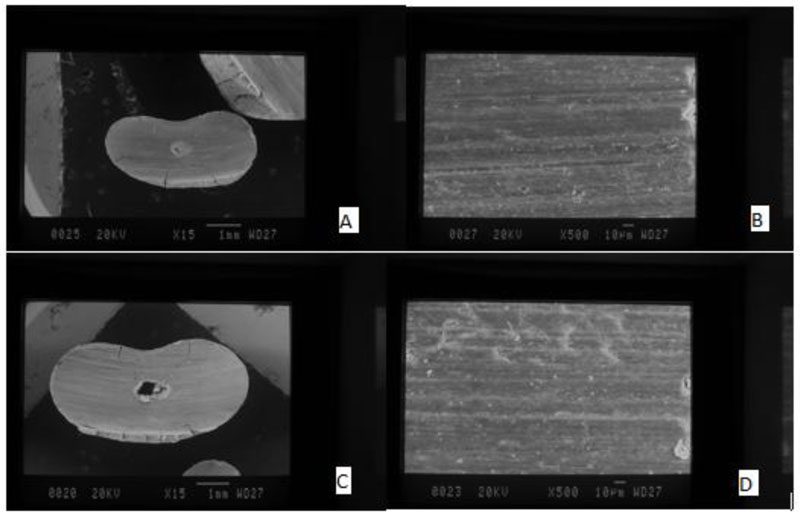
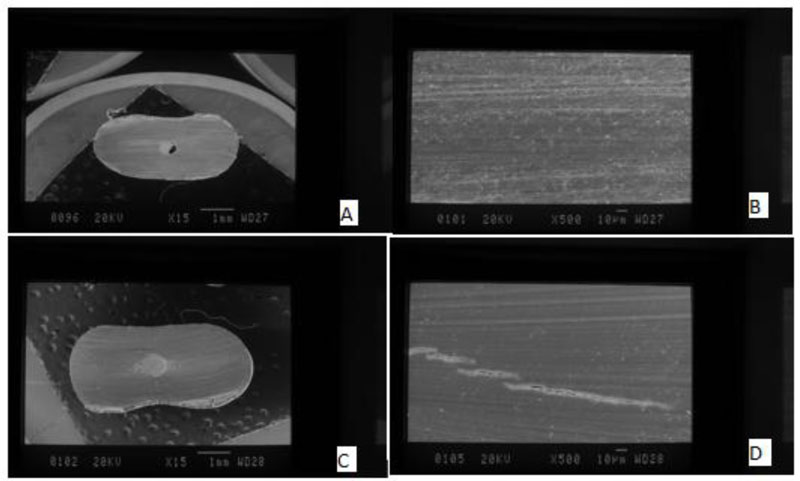
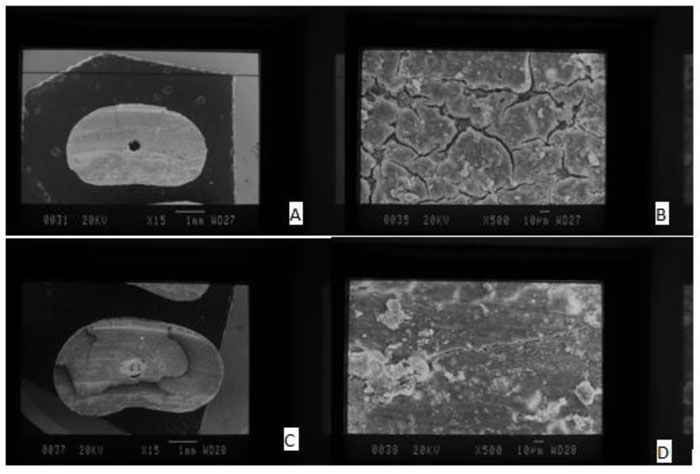
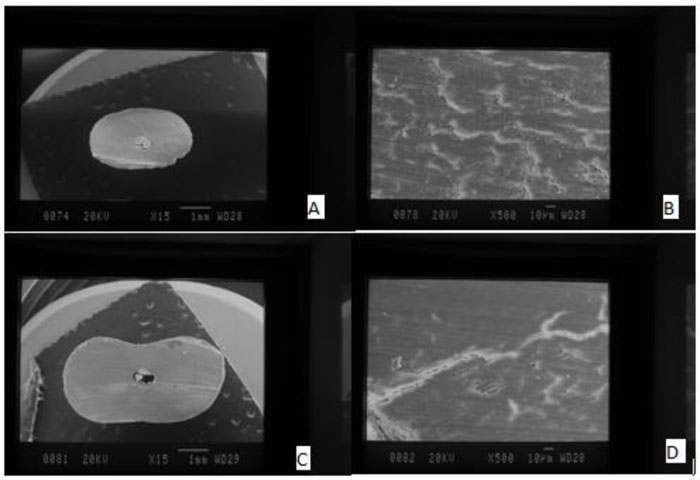
Before canal instrumentation, all canals were filing by manual file (k-file) NO#8 and 10, to create a glide path. The canal was irrigated with sodium hypochlorite (2.5%) interval of using any tool. Then the canal of teeth was prepared by the crown-down technique with M-two file rotary system Mtwo rotary files (VDW, Munich, Germany) up to No 30 with taper 4%. Using stereo-microscope at X25 magnification, the presence of crack and fracture of the root was evaluated for the second time. Then, samples were randomly divided into 10 groups based on different powers of laser and canal to be humid or dry under laser radiation (Table 1). The Diode laser (Quick lase 12W dual plus 810+980, UK) was put on the dental apex practically and pulled toward the dental crown in spiral motion. The laser was utilized for 10s puls within three iterated times. The rest time between the use of the laser was 10s. The samples were cross-sectioned after disinfection with a diode laser at 3 and 6mm length from the dental apex under water cooling with a low-speed diamond disk. Sections were observed under a scanning electron microscope (Jeol JSM 6500F, Jeol Ltd., Tokyo, Japan) at X500 magnification and images were taken.
In the current study, the samples were visually evaluated for the presence of microcracks by scanning electron microscope and stereomicroscope (Figs. 1-8). The reliability of these steps was approved by 2 specialist observers. Data analysis was done in the present research in two parts, including the descriptive and inferential statistics. The criteria of centralization tendency and distribution criteria were reported with tables and diagrams in the descriptive statistical phase. The multiple-logistic regression was employed in inferential statistics to determine the relationship between variables of humidity and laser power with a variable of microcrack formation. SPSS software Version 18.0 (Inc. Chicago, IL, USA) was utilized for data analysis. The significance level was considered 0.05 in this study.
| Group | Description |
|---|---|
| First group | Control group, humid canal (N=10) |
| Second group | Control group, dry canal (N=10) |
| Third group | Disinfection of humid canal by diode laser with power 1.5W (N=10) |
| Fourth group | Disinfection of dry canal by diode laser with power 1.5W (N=10) |
| Fifth group | Disinfection of humid canal by diode laser with power 2W (N=10) |
| Sixth group | Disinfection of dry canal by diode laser with power 2W (N=10) |
| Seventh group | Disinfection of humid canal by diode laser with power 3W (N=10) |
| Eighth group | Disinfection of dry canal by diode laser with power 3W (N=10) |
| Ninth group | Disinfection of humid canal by diode laser with power 4W (N=10) |
| Tenth group | Disinfection of dry canal by diode laser with power 4W (N=10) |


3. RESULTS
According to Table 2, the quantity and frequency of microcracks are seen within 3mm distance from dental apex separately based on laser power and humidity. The frequency of microcrack is increased by rising laser power. Similarly, the frequency of microcrack is higher under dry condition than the humid condition. According to Table 3, there was a statistically significant relationship between the probability for microcrack formation and variable of laser power so that the probability for microcrack formation at a power level of (2W) was 5.994 greater than the probability of microcrack formation without using a laser (P=0.018). The probability for microcrack formation with the power of (3W) was 7.867 times higher than the probability for microcrack formation when laser not used (P=0.008). The probability rate for microcrack formation by laser power (4W) was 14.605 times higher than the probability for microcrack formation without the use of a laser (P=0.001) and only when laser used with the power of (1.5W), there was no statistically significant relationship between the variable of laser power and microcrack (P=0.285). As shown in Table 2, the percent of microcrack formation without laser at humid condition was the same as the percentage for microcrack formation with the laser (1.5W) at the humid condition. There was a statistically significant relationship between a variable of humidity and microcrack formation so that the probability for microcrack formation under dry condition was 6.606 times higher than the probability of microcrack formation at humid condition (P<0.001) (Table 3).
The frequency of microcrack is increased by the rise of laser power. Similarly, the frequency of microcrack is greater under dry condition than at humid condition (Table 4). There was a statistically significant relationship among probability for microcrack formation and variable of laser power so that the probability for microcrack formation in laser power of (2W) was 4.462 times higher than microcrack formation when laser not used (P=0.043). The probability of microcrack formation under laser power of (4W) was 17.098 times greater than of microcrack formation without the use of a laser (P=0.001). Only under the condition when laser power was used with power (1.5W), there was no statistically significant relationship among variable of laser and microcrack (P=0.162). As shown in Table 3, the percent of microcrack formation without using laser under humid condition was the same as the percentage of microcrack formation by means of the laser power of (1.5W) at the humid condition. There was a statistically significant relationship among the variable of humidity and microcrack formation so that the probability for microcrack formation under dry condition was 4.978 times higher than for microcrack formation at humid condition (P=0.001) (Table 5).
| - | - | MicroCrack 3mm | |||
|---|---|---|---|---|---|
| Power | Moisture | No | Yes | ||
| Count | Row N % | Count | Row N % | ||
| Without Laser | Yes | 8 | 80.0% | 2 | 20.0% |
| - | No | 6 | 60.0% | 4 | 40.0% |
| - | Total | 14 | 70.0% | 6 | 30.0% |
| 1.5w | Yes | 8 | 80.0% | 2 | 20.0% |
| - | No | 3 | 30.0% | 7 | 70.0% |
| - | Total | 11 | 55.0% | 9 | 45.0% |
| 2w | Yes | 5 | 50.0% | 5 | 50.0% |
| - | No | 2 | 20.0% | 8 | 80.0% |
| - | Total | 7 | 35.0% | 13 | 65.0% |
| 3w | Yes | 5 | 50.0% | 5 | 50.0% |
| - | No | 1 | 10.0% | 9 | 90.0% |
| - | Total | 6 | 30.0% | 14 | 70.0% |
| 4w | Yes | 4 | 40.0% | 6 | 60.0% |
| - | No | 0 | .0% | 10 | 100.0% |
| - | Total | 4 | 20.0% | 16 | 80.0% |
| - | OR | 95% C.I.for OR | P-value | |
|---|---|---|---|---|
| - | Lower | Upper | ||
| Power | - | - | - | - |
| Without Laser (reference) | 1 | - | - | - |
| 1.5w | 2.188 | .521 | 9.182 | .285 |
| 2w | 5.994 | 1.351 | 26.593 | .018 |
| 3w | 7.867 | 1.718 | 36.021 | .008 |
| 4w | 14.605 | 2.872 | 74.274 | .001 |
| Moisture | - | - | - | - |
| Yes (reference) | 1 | - | - | - |
| No | 6.606 | 2.430 | 17.955 | <0.001 |
| - | - | MicroCrack 6mm | |||
|---|---|---|---|---|---|
| Power | Moisture | No | Yes | ||
| Count | Row N % | Count | Row N % | ||
| Without Laser | Yes | 7 | 70.0% | 3 | 30.0% |
| - | No | 8 | 80.0% | 2 | 20.0% |
| - | Total | 15 | 75.0% | 5 | 25.0% |
| 1.5w | Yes | 7 | 70.0% | 3 | 30.0% |
| - | No | 4 | 40.0% | 6 | 60.0% |
| - | Total | 11 | 55.0% | 9 | 45.0% |
| 2w | Yes | 7 | 70.0% | 3 | 30.0% |
| - | No | 2 | 20.0% | 8 | 80.0% |
| - | Total | 9 | 45.0% | 11 | 55.0% |
| 3w | Yes | 6 | 60.0% | 4 | 40.0% |
| - | No | 1 | 10.0% | 9 | 90.0% |
| - | Total | 7 | 35.0% | 13 | 65.0% |
| 4w | Yes | 4 | 40.0% | 6 | 60.0% |
| - | No | 0 | .0% | 10 | 100.0% |
| - | Total | 4 | 20.0% | 16 | 80.0% |
| - | OR | 95% C.I.for OR | P-value | |
|---|---|---|---|---|
| - | Lower | Upper | ||
| Power | - | - | - | |
| Without Laser (reference) | 1 | - | - | - |
| 1.5w | 2.791 | .663 | 11.756 | .162 |
| 2w | 4.462 | 1.048 | 19.005 | .043 |
| 3w | 7.245 | 1.641 | 31.999 | .009 |
| 4w | 17.098 | 3.388 | 86.297 | .001 |
| Moisture | - | - | - | - |
| Yes (reference) | 1 | - | - | - |
| No | 4.978 | 1.935 | 12.805 | .001 |
4. DISCUSSION
The effect of various powers of diode laser (with wavelength: 980nm) was examined on microcrack formation in dental wall root canals using a scanning electron microscope in the current research, thereby to identify the optimal power of diode laser for cleaning and disinfection of root canal with the minimum damage in hard tissue surrounding the root. The results of the present research showed that the frequency of microcracks increased within 3 and 6mm distance from the dental apex by the rise of laser power. This increased rate was statistically significant so that following to the rise of laser power from 2W to 4W, the probability for microcrack formation was increased 5.994 to 14.605 times within 3mm distance and from 4.462 to 17.098 times within 6mm distance. In this regard, Mortiz et al. also indicated that the complete removal of bacteria by diode laser only occurs if higher radiation power of the laser is used that causes higher temperature on the root surface [8]. Similarly, Esteves-Oliveira et al. radiated dentin continuously under the wavelength of 808nm with a diode laser with a power of 2.5W, they observed initial signs of melting and structural changes in dentin [15]. In fact, while the cleaning and preparation process will be done more perfectly by an increase in laser power, this higher power may have hazardous effects on the periodontal tissue of the root canal and it may change the composition and structure of the tissue [16]. These variations may include evaporation and carbonization and even melting that is followed by recrystallization for the hard tissue [17]. Gutknecht et al. [18] implied a low rate of absorption of the diode laser in the hard tissue and expressed dominant interactions of radiation as transitional, dispersive and reflective types.
According to the wavelength (980nm) of this narrow laser beam and lower power of the laser, the results of their studies are justifiable. The findings of the current study also indicated that the optimal power of 1.5W for a diode laser with a wavelength of (980nm) for cleaning and disinfection of root canal has minimum damage so that there was no statistically significant relationship between the variable of laser power and microcrack formation within three and six millimeter distances and the percentage of microcrack formation under humid condition was the same as the percent of microcrack formation at the laser power level of (1.5W). In line with this finding, Asnaashari et al. showed that the power of 1.2W for a diode laser with a wavelength of 810nm significantly reduced all cultured species [19]. In addition, a study by Da Costa Ribeiro et al. on 24 extracted mandibular incisors concluded that despite the creation of melting in the dental apical area, a diode laser with wavelength (810nm) and power (1.25W) was suitable for root treatment preparation and it was not unsafe for periodontium tissue [11]. In another investigation, Wang et al. (2005) indicated that it could reduce the smear layer, which caused reducing micro-leakage of apical by using suitable power (980nm) of diode laser [20].
On the other hand, water-spray on radiation site is one of the complementary activities that could be very practical along with simplicity. It may increase the disinfection effects of laser and reduce the related side-effects on hard periodontal tissue. The water presence leads to better interaction between laser and tooth, as a result, reduces thermal damage in nervous tissue and also affects the rising efficiency of the laser on dental hard tissue [21]. The studies have also shown that the diode lasers had good penetration, high interaction with water and hydroxyapatite of dental hard tissue [20, 22]. Faria et al. (2013) showed that removal of the smear layer was done well in samples that had been under radiation by a diode laser at the wavelength (980nm) and power (1.5W) with water spray coolant and damages in dentin were limited and no fracture occurred in it [23]. The findings of the current study also indicated that dryness of the canal during laser radiation might be an influential factor for microcrack formation so that the probability for microcrack formation was increased up to 6.606 times within three millimeters distance from the dental apex and 4.978 times in six millimeters distance from the dental apex under humid condition. This shows well the impact of humidity presence on reducing the frequency of microcrack formation. The effect of water spray on reducing the frequency of microcracks in using a diode laser with wavelength (980nm) may be for this reason that the wavelength in these types of lasers is adjusted to the range of water absorption in the infer-red area so that dispersion and absorption of laser radiation can be ignored in other tissue elements compared to absorption of laser radiation in existing water in the given tissue. Thus, as dental enamel or dentin is radiated by a laser pulse with adequate energy, the existing water on the surface of the tissue is heated and quickly rises to the higher temperature. As a result, it destroys microorganisms on this surface to a great extent and it reduces the hazardous effects of radiation in the depth of the hard tissue [7]. Likewise, it is noteworthy that the rest time has been considered 10s between any radiation interval in the present research. According to the study by Hmud et al. [12], this period was selected because of a lack of significant difference between rest times (5-15s) in operation with a diode laser at the wavelength (980nm).
CONCLUSION
The optimal power of a diode laser is 1.5W at the wavelength (980nm) for cleaning and disinfection of the root canal at the minimum damage in the periodontal hard tissue. Likewise, the findings prove that the existing humidity may highly reduce microcrack formation within three and six millimeters distances from the dental apex and it can decrease thermal side-effects of diode lasers on dental hard tissue.
SUGGESTIONS
According to the findings of current research, it is recommended to avoid from using the higher power of 1.5W in diode laser with wavelength (980nm) for cleaning and disinfection of the root canal and to use certain water spray in radiation site during operational processes with a diode laser at a power level (1.5W). It is also generally suggested for conducting other studies with other parameters of laser radiation as well in order to identify variables involved in laser properties further. Likewise, with respect to the rising efficiency of the laser in using along with chemical cleaning solutions in many studies, it is recommended to conduct complementary studies for further use of clinical supplementary methods. It is also suggested for the execution of future investigations about the distribution of thermal energy in the periodontal tissue of the root canal as well in order to identify the hazardous effects and controlling them better.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The protocol of the clinical trial, was approved by the Ethics Committee of Kermanshah University of Medical Sciences, Iran.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from each participant prior to the study.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the “jumpshare.com” at “https://jmp.sh/HyimzdQ.
FUNDING
This work was performed with funds from the Kermanshah University of Medical Sciences, Kermanshah, Iran (Grant No. 96662).
CONFLICT OF INTEREST
The authors declare no conflicts of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the Kermanshah University of Medical Sciences to support this work.

