All published articles of this journal are available on ScienceDirect.

Assessment of Parents’ Knowledge and Attitudes on Emergency Management of Permanent Avulsed Teeth in Western Saudi Arabia
Authors Info & Affiliations
Abstract
Objective:
One of the most common dental injuries is dental avulsion. This study, conducted in the western region of Saudi Arabia, aimed to evaluate parent’s knowledge and attitudes regarding the emergency management of avulsed permanent and deciduous teeth in children.
Methods:
A cross-sectional study was conducted among 393 parents recruited from six dental clinics and hospitals in Makkah and Jeddah, Saudi Arabia. The data were collected with a self-administered questionnaire that assesses the level of knowledge for managing deciduous and permanent avulsed teeth.
Results:
The total score for correct answers about managing permanent avulsed teeth had a mean of 4.77 and a standard deviation of 2.14 (out of 10 questions). With a permanent avulsed tooth, 35.37% were aware of dental reimplanting, 27.7% identified milk as an appropriate medium, and 57.5% would seek professional help immediately after dental trauma. Females and participants with a bachelor’s or higher degree had significantly higher levels of knowledge than males and participants with a high school or lower education. There were 28.5% of respondents who had a previous history of dental trauma for a child. A total of 62.1% knew that there is a difference in managing deciduous versus permanent teeth, but only 40.7% knew the proper management for deciduous avulsed teeth. Previous history of child dental avulsion was not found to be associated with more knowledge on managing avulsed deciduous or permanent teeth.
Conclusion:
Parents in the western region of Saudi Arabia have inadequate levels of knowledge to manage deciduous and permanent tooth avulsion. More efforts should be applied for conducting promotional health campaigns aimed at improving parents’ knowledge.
1. INTRODUCTION
Traumatic dentoalveolar injuries are one of the most important problems encountered by today’s dentists [1]. Injuries range from minor enamel fractures to more complex fractures of jaws and avulsion of teeth [1, 2]. Dental avulsion is defined as the complete displacement of a tooth out of its socket, associated with severe periodontal ligament with or without the involvement of the fractured alveolar bone [3]. Some studies reported that the maxillary central incisors in both deciduous and permanent dentition are the most commonly involved site [4], and 8–12 years old is the most common age range experiencing dental avulsion [5]. Boys are more likely to be affected than girls [6].
There are different treatment modalities for managing an avulsed permanent tooth, including functional appliances, minor orthodontic movement, prosthetic replacement, and immediate reimplantation followed by endodontic treatment [3]. Immediate reimplantation in its socket of the avulsed permanent tooth is considered the treatment of choice to avoid further damage to the periodontal membrane [5]. The viability of the periodontal membrane is one of the most important factors determining the prognosis of the replanted tooth [7]. Therefore, using a transport medium such as saline or milk to prevent dehydration of the root surface is a critical factor [8, 9]. It should be noted that deciduous teeth must be treated differently [10]. In fact, reimplanting deciduous teeth is contraindicated [11, 12]; rather, radiographic images and observation, along with some consideration after an avulsion, are needed, according to the level of injury [11].
Parental knowledge of first aid measures for an avulsed tooth is essential for proper management as they are usually the first people to attend and make decisions [13]. Delayed reimplantation and unphysiological storage result in loss of the replanted tooth over time [14]. For this reason, parents, teachers, and caretakers should all have adequate knowledge about the important steps in managing avulsed permanent teeth [15].
Several studies on the management of avulsion have highlighted the role of parental knowledge in the emergency management of avulsed permanent teeth [16-19]. In Turkey, 90.7% of participants would not reimplant the avulsed tooth, and 68.2% had knowledge about the critical time frame for reimplanting; however, most of the respondents lacked knowledge regarding cleaning and a good medium for storing the avulsed tooth [20]. This is different from a study conducted in Lagos, Nigeria, where 90% of guardians lacked appropriate knowledge regarding the urgent management of an avulsed tooth [21]. Another study among Kuwaiti parents found that 35.9% of participants were aware of the possibility of reimplantation, 70.6% of parents would seek professional help, and 32.9% were informed about appropriate cleansing media [22].
Few studies have evaluated the awareness among parents in Saudi Arabia regarding the management of avulsed teeth. Two studies conducted in Al-Baha [13] and Abha city [4] found that 58% to 73.8% of parents were not aware of the possibility of reimplanting, less than 50% knew about proper cleansing for an avulsed tooth, 11.7% to 21% knew acceptable replanting mediums, and around 50% were unaware of the proper time frame for reimplantation [4, 13]. In fact, both studies concluded that a majority of parents were unaware of the proper emergency management of tooth avulsion.
Similarly, studies regarding this aspect are lacking in Jeddah city, one of the largest cities in Saudi Arabia. Also, most of the previous studies have assessed the level of knowledge about the avulsion of permanent teeth, but not of deciduous teeth. Thus, this study aimed to evaluate parents’ knowledge and attitudes regarding the emergency management of avulsed permanent and deciduous teeth in children in the western region of Saudi Arabia.
2. MATERIALS AND METHODS
This cross-sectional study investigated parents’ knowledge and attitudes regarding the emergency management of avulsed permanent teeth in children using convenience sampling. Participants were recruited from six different dental clinics in Makkah and Jeddah cities, including King Fahad Armed Forces Hospital, Alfarabi Private College, Umm Al-Qura Dental Hospital, Kind Faisal Hospital, Alkaakih primary healthcare center, and Al-Hayat Medical Center. Data were collected during December 2019. Inclusion criteria included parents who were over 18 years old. The exclusion criteria included parents whose children lived with others, non-Arabic speakers, and participants who did not sign the consent form. The sample size was calculated with a confidence level of 90%, an estimated prevalence of 50%, and a 5% level of precision, yielding a minimum sample size of 271. However, to overcome the expected non-response rate, 420 individuals were invited to participate in this study.
After signing the consent form, participants answered the study’s self-administered hard copy questionnaire, which took from 4 to 6 minutes. Participants were informed of their right to withdraw from the study at any time. The questionnaire was distributed face-to-face to the participants during their free time while they were waiting at the dental clinic. All data were kept anonymous, and any recognizable data were discarded.
The questionnaire was derived from those used in multiple previous studies [4, 11, 13, 22], with modifications. The modifications in the layout and repeated questions from different articles were removed. The questionnaire is shown in Appendix A. It is composed of 19 questions allocated in three parts. The first part gathered the parents’ sociodemographic characteristics, including age, gender, education level, occupation, marital status, family monthly income, nationality, number of children, and previous history of dental trauma to children. The second part consisted of 10 questions about the proper management of a case scenario of a 10-year-old boy with an avulsed permanent central incisor. Questions encompassed proper management in the case of complete avulsion, partial extrusion, holding position, possibility of reimplanting, transportation medium, cleaning method, timing, and profession of a health care provider. Each question had one correct answer, and a total score for knowledge was calculated by totaling the scores for all the correct answers. Each correct answer for a question was counted as one point. The highest possible score was 10, while the lowest possible score was zero for a participant who answered all the questions as wrong. The last part assessed the parents’ knowledge of emergency management of a deciduous avulsion with two questions. The questionnaire was administrated in Arabic after being tested by a pilot group of 10 individuals, and their data were not included in the main study results. This step was conducted for face and content validation of the questionnaire to ensure clarity of content, grammar, spelling, and organization.
Data were tabulated, and descriptive statistics were conducted, generating mean (m), standard deviation (SD), frequency, and percentage tables. Chi-square, Fisher’s exact test, ANOVA, t-test linear regression, and logistic regression were used to analyze the data. Ethical approval was received from the Institutional Review Board of Umm Al-Qura University, Faculty of Dentistry, number 150-19.
| Variable | n | % | |
|---|---|---|---|
| Gender | Male | 138 | 35.10 |
| Female | 255 | 64.90 | |
| Level of education | No formal education | 10 | 2.50 |
| Elementary school | 40 | 10.20 | |
| High school diploma | 120 | 30.50 | |
| Bachelor’s degree or higher | 223 | 56.70 | |
| Employment | Student | 22 | 5.60 |
| Employee | 209 | 53.20 | |
| Business owner | 35 | 8.90 | |
| Unemployed or retired | 127 | 32.30 | |
| Social status | Single | 14 | 3.60 |
| Married | 331 | 84.20 | |
| Divorced | 41 | 10.40 | |
| Widowed | 7 | 1.80 | |
| Family income (Saudi Riyal) | Less than 5,000 | 138 | 35.10 |
| 5,000 to 10,000 | 146 | 37.20 | |
| More than 10,000 | 109 | 27.70 | |
| Nationality | Saudi | 294 | 74.80 |
| Non-Saudi | 99 | 25.20 | |
| Previous history of children with dental trauma | Yes | 112 | 28.50 |
| No | 281 | 71.50 |
3. RESULTS
A total of 393 participants completed the questionnaire for a response rate of 93.57%, with a mean age of 37.17 years and SD of 9.98. Participants had a mean number of children of 2.76 (SD = 1.9). Other demographic variables are provided in Table 1.
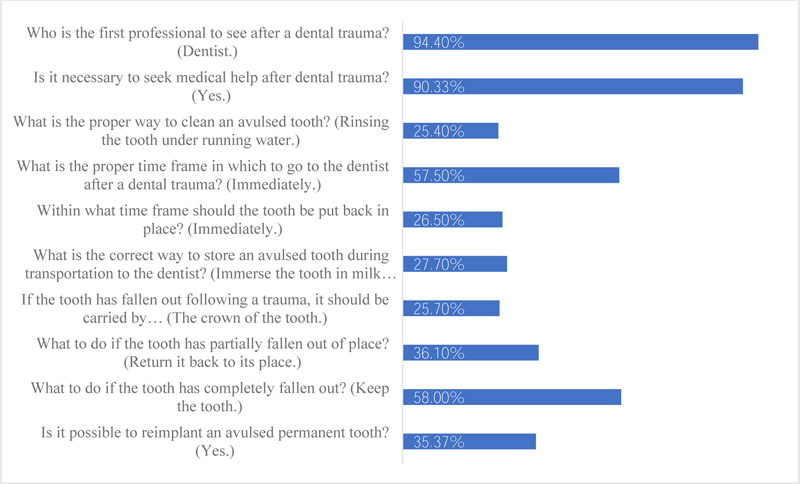
Participant answers to the items regarding dental trauma management were varied and are shown in Table 2 and Fig. (1). The mean total score for correct answers was 4.77, with an SD of 2.14. The possible score ranged from 0 to 10. Using t-test, the total correct answer score for dental avulsion management was found to be significantly higher in females (mean = 5.01, SD = 2.2) than males (mean = 4.31, SD = 1.9), t(311) = −3.23, p = 0.001. Additionally, the score was significantly higher among participants with a bachelor’s degree or higher education (mean = 5.13, SD = 2.2) than for all the other subgroups combined (mean = 4.29, SD = 1.96), t(381) = 3.98, p <0.001. Results of the t-test, ANOVA, and simple linear regression test revealed that the total correct answer score for dental avulsion management was not significantly related to age, nationality, marital status, family income, number of children, or previous history of child dental avulsion.
| Correct Answer | n | % | |
|---|---|---|---|
| Is it possible to reimplant an avulsed permanent tooth? | Yes. | 139 | 35.37 |
| What to do if the tooth has completely fallen out? | Keep the tooth. | 228 | 58.00 |
| What to do if the tooth has partially fallen out of place? | Return it back to its place. | 142 | 36.10 |
| If the tooth has fallen out following a trauma, it should be carried by… | The crown of the tooth. | 101 | 25.70 |
| What is the correct way to store an avulsed tooth during transportation to the dentist? | Immerse the tooth in milk or place it in the child’s mouth. | 109 | 27.70 |
| Within what time frame should the tooth be put back in place? | Immediately. | 104 | 26.50 |
| What is the proper time frame in which to go to the dentist after a dental trauma? | Immediately. | 226 | 57.50 |
| What is the proper way to clean an avulsed tooth? | Rinsing the tooth under running water. | 100 | 25.40 |
| Is it necessary to seek medical help after dental trauma? | Yes. | 355 | 90.33 |
| Who is the first professional to see after a dental trauma? | Dentist. | 371 | 94.40 |
In regard to questions related to deciduous teeth, 266 (62.1%) of the participants were aware that there is a difference in managing deciduous and permanent teeth. The chi-square test showed that participants with a bachelor’s degree or higher education were found to be significantly more likely to know that there is a difference between management of deciduous and permanent teeth (66.4%) than others (56.5%), X2(1) = 4.014, p = 0.045. The chi-square test, Fisher’s exact test, and logistic regression also revealed that there was no significant difference in this item correlated with age, gender, nationality, marital status, family income, number of children, or previous history of child dental avulsion.
A total of 160 (40.7%) respondents were aware of the proper management for avulsed deciduous teeth (do not reimplant and seek medical help immediately). This item was not significantly different for age, level of education, gender, nationality, marital status, family income, number of children, or previous history of child dental avulsion.
4. DISCUSSION
This study aimed to assess the knowledge of parents living in the western region of Saudi Arabia with regard to managing dental avulsion. This study showed that around one-fourth of the participants’ children had a previous history of dental trauma. The participants’ total knowledge of avulsed permanent teeth was around the midpoint, indicating a moderate level of knowledge. This score was higher among females and participants with higher education. Three out of five participants knew there is a difference in managing deciduous teeth, with higher scores among participants having higher education. In addition, two out of five knew regarding the proper management of avulsed deciduous teeth. A previous history of children with dental trauma had no impact on participant level of knowledge about dealing with permanent or deciduous teeth avulsion.
Our study and previous studies in Saudi Arabia indicate that there is a high prevalence of dental trauma among children in Jeddah (28.5%), Albaha (32%), and Abha (39%). This reflects the importance of estimating the possibility of proper management of a dental avulsion among the parents who are the first line of contact when such an event occurs.
In our study, we generated a continuous measure of this knowledge by calculating the total score (m = 4.77, SD = 2.14) for 10 questions, and the result was a little higher than in a previous study conducted in Kuwait, with a median of 3 (IQR = 2) out of eight items [22]. Other studies showed only the percentages for knowledge of each item individually. However, our study indicated that parents have low levels of knowledge about dealing with dental avulsion of permanent teeth. This was similar to studies conducted in Brazil [18], Turkey [20], Nigeria [21], Jordan [23], Kuwait [22], United Arab Emirates [24], and Saudi Arabia, in Albaha [13] and Abha [4] cities. However, there was some variation in the levels of knowledge, as detailed in the next paragraphs.
In regard to the possibility of reimplanting an avulsed permanent tooth, 35.37% were aware that this is the best course of management. This proportion was similar to previous studies in Kuwait (35.9) (sample size= 554) [22] and Albaha, Saudi Arabia (42%) (sample size= 263) [13], but better than studies in Abha, Saudi Arabia (26.2%) (sample size= 274) [4], and Turkey (9.3%) (sample size= 289) [20]. The variation might be due to differences in educational health campaigns between cities and countries, but all the results across countries showed some deficiency in this important step. According to the International Association for Dental Traumatology, implantation is contraindicated in some cases, such as with severe periodontitis, a badly decayed tooth, or severe heart disease [25].
The storage medium is important for preserving periodontal ligament (PDL) cells used in dental reimplanting, and milk is recommended as an available appropriate osmolarity balanced medium [25]. Tap water and saline are poor mediums due to osmolarity and Ph level [26]. Around 27.7% of the respondents in our study identified the correct medium for an avulsed tooth; this finding was better than in all of the other studies conducted in Turkey, Nigeria, Kuwait, and Saudi Arabia, which ranged from 1.1% to 21% [4, 13, 20-22].
The participants in our study identified the correct choice for proper cleaning (running tap water), time to reimplantation and seeking help (immediately), and the correct position to hold (crown) an avulsed permanent tooth (25.4%, 26.5%, and 25.7%, respectively). This was lower than results in Kuwait and slightly lower than results in Saudi Arabia for the same items: cleaning by running tap water (29% to 47.7%), immediate reimplantation (27% to 33.9%), and holding by the crown (37% to 69%). The reason for this difference cannot be explained by our data, but it might be due to different medical educational information the participants receive, which varies from country to country. However, the percentages of the findings in Saudi studies are similar to some extent and show poor levels of knowledge about factors that are important for a good prognosis with reimplantation [27].
Despite 90% of respondents indicated the need to seek medical attention after a dental trauma, only 57.50% would do it immediately. This percentage showed to be lower than in previous studies conducted in Turkey, India, Nigeria, and Kuwait [20-22, 28], which ranged from 64.4% to 90% of respondents indicating they would need to seek medical help immediately. This might be attributed to the fact that most of the parents in our study did not understand the importance of time as a crucial factor for successful reimplantation. Nonetheless, a majority of the participants in our study would go to a dentist, which is similar to the results from Turkey, Kuwait, and Saudi Arabia [13, 20, 22].
Our results also showed that females and those with higher education had significantly more knowledge. This contradicts some previous studies’ [13, 20, 22] finding that gender and educational levels have no significant impact on the level of knowledge. This might be due to differences in culture and the typical variation in parental roles from country to country and city to city.
One of the important aspects of this study is that it included an additional section regarding deciduous teeth, which was not covered in previous studies [4, 13, 20-22]. A total of 62.1% of the parents knew that there is a difference in managing deciduous teeth versus permanent teeth, while 40.7% were aware of the proper management for avulsed deciduous teeth. This percentage is also considered to be low, and it is lower than previous studies conducted in Hong Kong (62.5% to 74.7%) [29, 30]. This might be because the studies in Hong Kong were conducted among teachers, who deal with young students on a daily basis and should be aware of such practices as a part of their duties.
As our results showed a low level of knowledge regarding the management of avulsed permanent and deciduous teeth in Jeddah, it would be beneficial to promote educational programs, especially because the prognosis for an avulsed tooth depends on appropriate immediate emergency management. Health promotional activities can be conducted using smartphone applications, which have been found to be more effective than more conventional educational interventions [31]. Using the internet alone might not be sufficient, as the public may be unable to evaluate and compare the reliability of sources of health-related information [32]. Many avulsed teeth could be saved if parents know how to manage cases, and negative consequences such as poor aesthetics and psychological and functional consequences due to a lost permanent tooth in early childhood could be avoided.
Despite the high response rate, validated questionnaire, and multiple centers used for recruitment, the results of this study have no external validity to Saudi Arabia in general, as the sample was not representative of all of Saudi Arabia. Furthermore, a self administered questionnaire was used, making the study results subject to self-reporting bias. Future studies should include a wider range of other individuals who play a big role in the emergency management of avulsed permanent teeth in children, such as teachers, coaches, and nurses.
CONCLUSION
Parents in the western region of Saudi Arabia demonstrated low levels of knowledge regarding emergency management of tooth avulsion for deciduous and permanent teeth. More efforts should be placed on improving parents’ knowledge about the management of avulsed teeth by using promotional health campaigns including the use of smartphone applications. Using the internet alone might not be sufficient, as the public may be unable to evaluate and compare the reliability of sources of health-related information.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study received the approval of the Institutional Review Board (IRB) of Umm Al-Qura University, Saudi Arabia, Faculty of Dentistry, with number 150-19.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
All participants signed the consent form before participating in the study.
AVAILABILITY OF DATA AND MATERIAL
The data that support the findings of this study are available from the corresponding author, [R.A], upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interests, financial or otherwise.
ACKNOWLEDGEMENTS
We would like to thank Dr.Sulaiman Alrezgan, Dr. Noor Farsi, and Dr. Abdualwahab Nagro, who helped us in collecting the data.

