All published articles of this journal are available on ScienceDirect.

Periodontal Surgery Intervention for Gingival Smile Correction - Case Report
Authors Info & Affiliations
Abstract
Introduction:
The success of anterior rehabilitation requires more skills than knowledge. It is necessary that the professional has updates on a new approach to obtain the best result considering the high degree of the exigency of these cases. The relationship between red and white esthetic is known and consolidated in the literature. Then, to achieve success in an esthetic smile is indispensable to apply periodontal surgery associated with restorative technique.
Methods:
In this report, a 28-year-old female patient sought care in a private clinic with a major cosmetic complaint due to disproportion of the clinical crown and gingival smile.
Result:
After planning, a clinical crown increase was performed, followed by the labial repositioning technique after the healing time of the initial surgery.
Conclusion:
It can be concluded that some of the surgical techniques, demonstrated in the literature, for gingival correction are feasible when correctly indicated. The best esthetic results will be achieved when the professional can understand the necessity to correct the disharmony of white and red esthetic.
1. INTRODUCTION
The dentogingival relationship is a key issue for smile harmony, since, under conditions of imbalance, it impairs esthetics and, therefore, it affects the individual's self-esteem [1]. Studies deal with the correlation between the excessive vertical exposure of the gingiva and its possible causes, such as hypertrophy of the upper lip lifting muscles, vertical maxillary excess, lower upper lip length, among several other factors [2]
The treatment of this alteration varies according to its etiology and diagnosis, ranging from minimally invasive therapies, such as botulinum toxin type A, to more invasive surgical procedures [3, 4]. The flap surgery techniques for gingival recontouring have been widely used to reestablish esthetics in cases of the gingival smile, but in some cases it is necessary to be associated with other procedures, aiming at patient’s satisfaction and favorable prognosis in the long term [5].
The choice of the surgical approaching type will depend on factors such as medical history and current condition, patient’s age and, obviously, the amount of exposed gingiva [1]
Among the various procedures described, the objective of this case was to report the correction of one gingival smile through the association of two techniques of gingival surgeries.
2. CASE REPORT
A female patient, 28 years old, diagnosed with leucoderma, sought care in a private clinic with a cosmetic main complaint, due to disproportion of clinical crown and gingival smile (Fig. 1).
A clinical examination was performed, wherein the anamnesis patient did not raise any other complaints, in addition to the one previously described, and denied the presence of underlying diseases. In the physical examination, a disharmony of the regular concave arch and absence of gingival zenith in elements 11 and 21 were observed, but the gingiva presented a healthy appearance with orange peel and light pink color (Fig. 2).


2.1. Proposed Treatment
After a clinical and complimentary examination, surgical treatment was proposed by initially increasing the clinical crown of elements 13 to 23, recommending the use of internal bevel flap surgery (Figs. 3-5). After 90 days of healing, the measurements were taken to perform the technique of lip repositioning, in order to re-establish the esthetics of the smile completely.
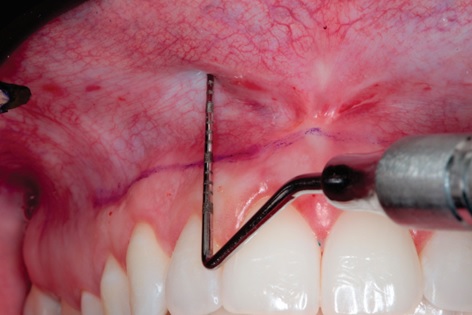
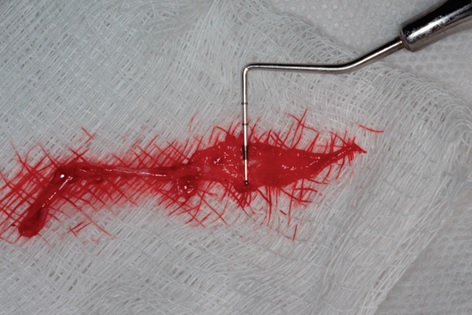
The distance between the cervical region of the tooth and the total exposure of the gingiva was measured using forced-smile, resulting in 5mm value (Fig. 6). The mucogingival junction was drawn with a sterile copy pencil, which was the lower limit, and the upper extremity double the measurement obtained initially, in other words, 10 mm in order to preserve the keratinized gingiva (Fig. 7). The procedure was followed by the completion of submucous infiltrative terminal anesthesia, tissue seizure and incision with a blade, which was first performed in the lower border and then in the upper border until complete excision of the delimited area (Fig. 8, 9). With the assistance of the Metzenbaum scissors, the tissue was divulged to reach the periosteum and incised in order to preserve its integrity, since the next step was the repositioning of the tissue (Fig. 10). The muscle attachment and later the mucosa were first sutured, both with polyglactin suture thread (Fig. 11).
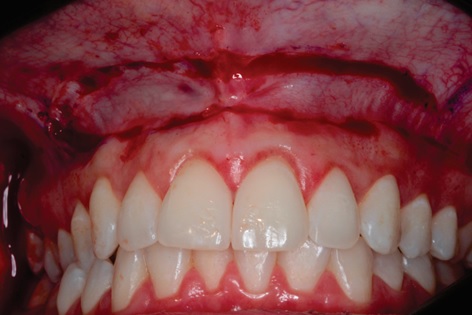
In the seven-day postoperative period, the patient presented a normal healing appearance; there was an absence of secondary infections and no complaints related to the surgical procedure (Fig. 12).
3. FOLLOW UP
In both, three months (Fig. 13) and then one year and a half follow-up (Fig. 14-16), the patient demonstrated satisfaction, improvement in self-esteem, harmonic smile without excess gingival exposure and presence of satisfactory gingival architecture with only 1 mm of gingival exposure.
4. DISCUSSION
In this report, the patient presented a major cosmetic complaint due to esthetic alteration in her smile. After clinical examination, surgical treatment was proposed, since it demonstrates a favorable prognosis in the long term. The first healing intention was observed, which denotes the use of internal bevel since the external bevel technique generates healing by second intention. However, the botulinum toxin type A is a possible minimally invasive treatment, but there is no guarantee of longevity since the toxin is absorbed by the organism in a period of 3 to 4 months, when the neuromuscular connections are re-established [3, 4].
Therefore, two surgical procedures were performed, the first being the conventional internal beveling method in order to regularize the gingival zenith, thus providing a regular gingival concave arch. Then, the first healing intention was observed. However, it was necessary to associate it with the technique of lip repositioning, because the exposed gingiva band was extremely wide, and it was not possible to correct only with the crown increasing technique. Literature has shown favorable results when surgical techniques are associated with these cases, which demonstrate the relevance of this report for contribution with the scientific area [6, 7].
Regarding the cosmetics features, the patient had a visible band of 5mm gingiva, which is out of standards considered esthetic. In the literature, the smile is considered pleasant in which the upper lip touches the cervical of the superior incisors, thus, the amount of exposed gingiva is a direct influence on the esthetics of the smile [8, 9]. In agreement with these data, it is noticed that the main complaint of the patient during anamnesis was concerning the gingival smile, which considered the same disharmony.











The proposed treatment plan re-established the harmony of white and red esthetic showing favorable results during the follow-up of the patient, without any kind of operative complications, which indicates the viability of the association of the techniques used when correctly indicated.
CONCLUSION
It can be concluded that some of the surgical techniques, demonstrated in the literature, for gingival correction are feasible when correctly indicated. The best esthetic results will be achieved when the professional can understand the necessity to correct the disharmony of white and red esthetic.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
The participants provided written informed consent involved in this study.
STANDARD FOR REPORTING
Care guidelines and methodology were followed to conduct the study.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
For the contribution of translation and revision of the Portuguese language into the English language, we thank the language teacher Bruno Oliver and the native Michael Zeigler.

