All published articles of this journal are available on ScienceDirect.

Intraoral Scanners in Personal Identification of Corpses: Usefulness and Reliability of 3D Technologies in Modern Forensic Dentistry
Authors Info & Affiliations
Abstract
Aims:
This study aims to verify the applicability of modern dental technologies and their related principles of use to the forensic sciences in the field of personal identification.
Background:
Personal identification has always had a major role in many legal and administrative actions regarding both living and death beings. The techniques used are much less advanced than the technologies potentially available.
Objective:
Modern technologies, available to the daily dental clinic practice, as intraoral scanners, combined in particular to the specialist skill in orthodontics, can help redefine the methods of personal identification according to the levels of accuracy, trueness and feasibility greater than those applied in traditional forensic dentistry.
Methods:
23 corpses (12F;11M) have been selected for intraoral scanning with the Carestream 3500® digital device. The superimposition of initial and late digital models, digital models and radiographs (orthopantomography and full mouth periapical films) has been evaluated to verify the stability of some structures as palatal rugae after death and to assess intraoral scanning as a successful comparative method between antemortem and post-mortem records (digital models or radiographs). Obtained results were subjected to statistical analysis by the t-student test and X-square test with Yates correction (p<0.05).
Results:
After death, palatal rugae significatively change especially in mouths with restorations/prosthesis/missing teeth. The percentages of correct matching between scans and radiographs are very higher (up 90%; p<0.05).
Conclusion:
This study has been set up to study and develop new, reliable and fast methods of personal identification that can surpass many of the issues seen with the other techniques by a modern rugoscopy, a modern radiographic-digital comparison and virtual oral autopsy.
1. INTRODUCTION
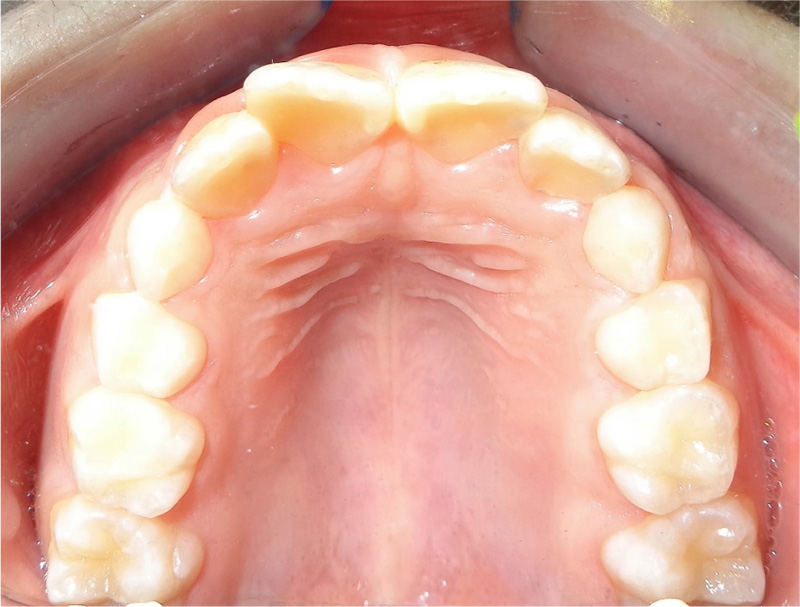
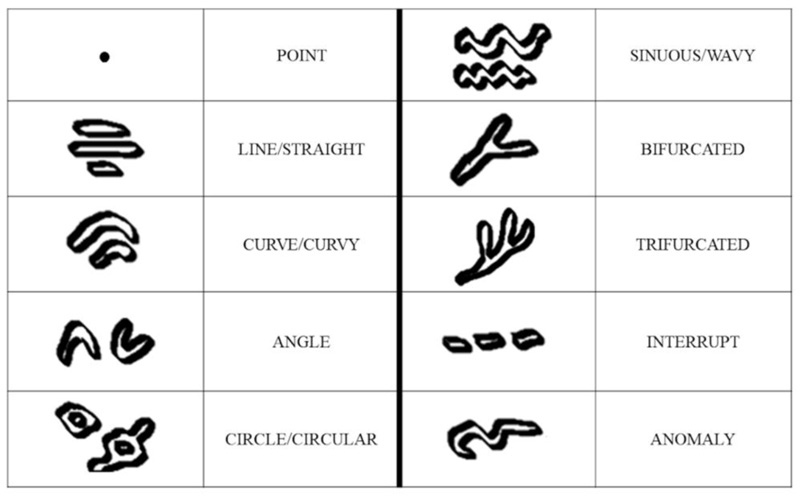
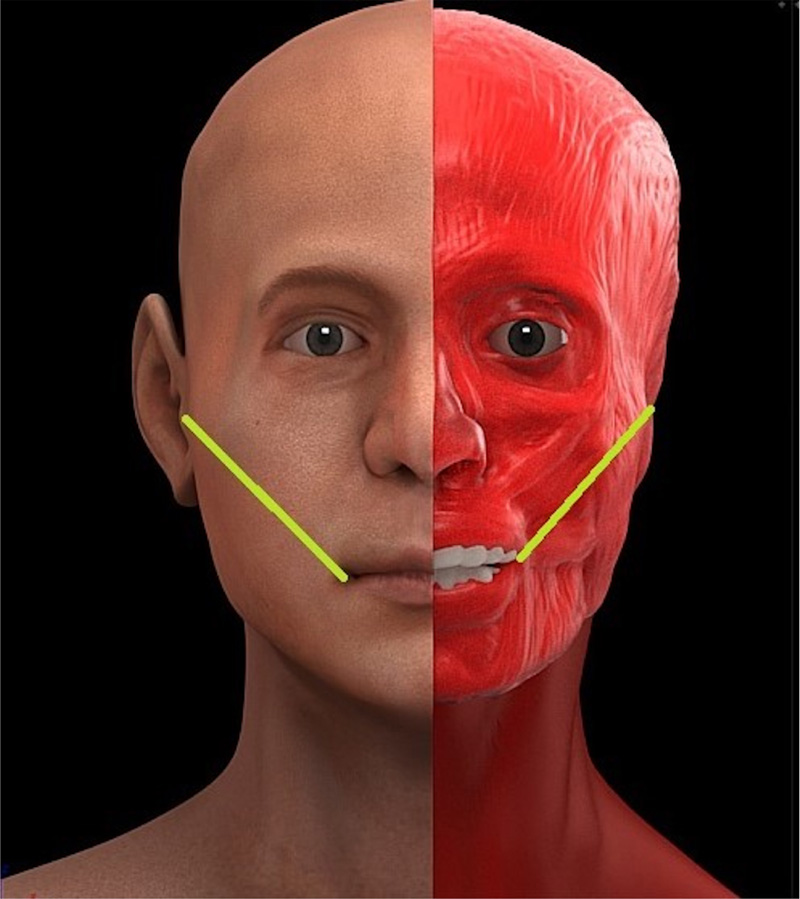
Forensic dentistry (or forensic odontology) is that branch of forensic science that exploits the skills of the dentist to determine the recognition of the person, whether living or deceased, for investigative purposes or justice processes. According to the definition of Keiser-Neilsen, forensic dentistry is the discipline that “in the interest of justice deals with the proper handling and examination of dental evidence and the proper evaluation and presentation of dental findings” [1]. From the past to today, the identification methods of odontologist competence have been enriched with new tools, also according to the most recent needs. To those of an exclusively dental nature, which mainly lead to comparative methods between ante-mortem data or between ante-mortem and post-mortem data (in an example, comparison between data collected during intraoral inspection and X-rays or plaster models of the subject of which identity is suspected), high-reliability methods such as rugoscopy and oral autopsy on cadaver have been associated. Traditional rugoscopy, also called palatoscopy, studies the characteristics of palatal rugae (the keratinized mucosa ridges placed behind the incisive papilla) (Fig. 1) through simple methods of pattern definition. Usually, on plaster patterns through the use of a pencil, the number of rugae, their shape (Fig. 2) and their length are highlighted following the reference classifications that over the years have been developed by different authors. Palatal rugae, such as hand fingerprints, are a unique and distinctive trait of the human being and remain unchanged after death [2]. Due to their dimensional stability, they are used as a method of personal identification during the visual inspection of mouth post-mortem comparing their features with plaster models of the dental arches (ante mortem data). Palatal rugae are structures very resistant to alterations on a chemical-physical basis and therefore are particularly useful in the case of mutilated or altered bodies where DNA examination, fingerprint analysis or observation of dental elements (for comparison with plaster models and ante-mortem x-rays) are not applicable. The oral autopsy, for the remarkable invasiveness, being a real complex surgical procedure, plays a role as important as it is critical because, with the methods currently documented, it entails a profound alteration of the face of the subject with important ethical and legal implications. Since the inspection of dental arches is crucial for identification and is still considered the main evidence in judicial investigations that require the identification of a corpse, the oral autopsy finds its main indication in the case where the inspection of the oral cavity is difficult. Simplified surgical protocols still require very large incisions (Fig. 3) to expose dental arches and allow the collection of dental records and this does not allow preservation of the facial integrity of the deceased [3]. Forensic dentistry has not followed the evolution of dental technologies. Intraoral scanners have profoundly changed the concept of dental impression and the workflow associated with it. The optical impressions detected with the scanner generate a three-dimensional model of the dental arches with a significant saving of time and less discomfort for the patient than the traditional impression. They are traditionally classified according to their technical characteristics such as the ability to capture the scan by a succession of the photo or video shots; the need to use opacizing powders, the speed of scanning capture, the accuracy of the result, the ability to get color models and the file type obtained (.ply, .stl,.obj). The use of intraoral scanners has made it possible to obtain models of dental arches often much more accurate than those detected with traditional dental impression materials [4]. This should be considered very important from a forensic point of view both for the possibility of having a detailed and reliable reproduction of both dental structures and palatal rugae and for the possibility of having a digital archive easily shareable even for judicial reasons without the risk of losing a significant antemortem data as in the traditional archives of plaster models. The main objective of this research is to demonstrate how the modern and latest technologies available to the daily dental clinic practice, combined in particular to the specialist skill in orthodontics, can help redefine the methods of personal identification according to the levels of accuracy, trueness, and feasibility greater than those applied in traditional forensic dentistry. The superimposability with 2D radiographs of digital scans obtained with intraoral scanners for forensic purposes in personal identification on living and corpses, has been evaluated.
2. MATERIALS AND METHODS
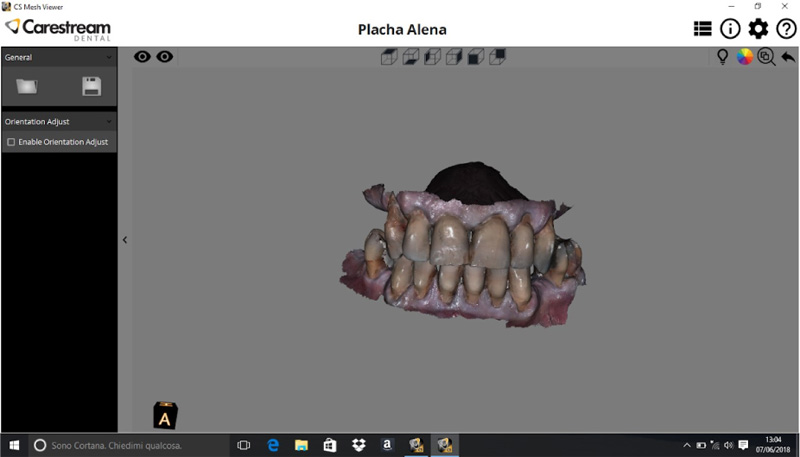
From January 2016 to February 2017, 23 corpses in permanent dentition (12 females and 11 males; aged between 45-69 years old) present in the morgue and suitable for intraoral inspection have been recruited for this study. They had the following features: full arches, partial or totally edentulous arches, fixed/removable prosthesis, different causes of death and no jaws fractures. A characteristic common to all the subjects is the belonging to the Caucasian race. Orthopantomographs and/or full mouth periapical films were taken, if available, when the subjects were still alive and released by relatives/dentists after death at the request of medico-legal operators and authorities as additional necessary identification material. The intraoral scanner has been used at the moment the corpses arrived at the morgue and, when possible, repeated after one week to obtain digital and plaster models. The intraoral Scanner Carestream 3500® used for this research is a dedicated portable laptop device and it belongs to the no powders and stitching-type category: it reprocesses the 3D image from a series of photographic shots generated by a single green-light pulse. For each scan shot, the device takes about 250 photos at the same time. It provides a high level of accuracy (30 µm) and resolution (1024x768 pixels for still images and 640x480 pixels for videos). The scanning takes 30 minutes for full arches mode. Once every file (.stl) has been created, the true colour or plaster style can be chosen for each arch and reciprocal relationship by occlusion on the CS Viewer Software can be checked (Fig. 4).
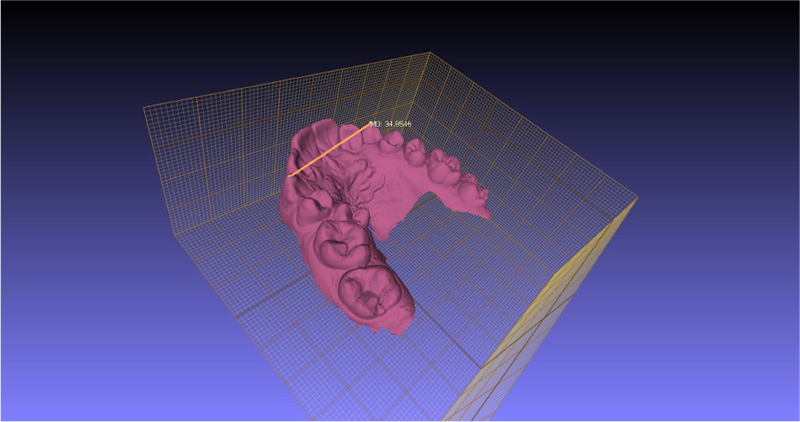
For all the corpses, the intra-oral scans have been taken by the same operator (A.P.). The identity intended as name and surname was hidden by the medico-legal operators responsible for the morgue for privacy reasons; therefore, the subjects were renamed through numbers. Age and sex were provided for each subject. The corpses have been further classified for the type of prosthetic/conservative rehabilitations and the cause of death if known. All the general data of the subjects sampled have been collected in digital sheets (Microsoft Office Excel, 2016®). The radiographic documentation was on CD-ROM, and if the CD-ROM was not available, in the presence of a traditional radiograph, it has been scanned with HP Officejet J4580 All-in-One and converted in the digital image as .jpeg file. The identity of the subjects marked on the radiographs was hidden by the medico-legal operators before making them available for user evaluations for this study. After the acquisition of all the scans, the digital archive obtained has been used to start the digital measurements on a dedicated software called MeshLab® (version 1.3.3). To calibrate the digital dimensions with the in vivo dimensions, and to have the certainty, there is a proper correspondence of both of them with each other before to start the use of an intra-oral scanner, a digital caliper (Borletti CDJB20, accuracy 0.03 mm) has been used. The inter-molar and inter-canine distance of every arch, the mesial-distal diameter of canines and the vertical height of first molars (from the median sulcus to the gingival contour) and of canines have been recorded. On the MeshLab Software, the same measurements have been taken and recorded on a dedicated digital sheet for a direct comparison between the in vivo and digital values (Fig. 5).
The part of the study dedicated to the digital superimpositions has been conducted by two independent operators: A dentist specialized in orthodontics (A.P.) and a doctor specialized in forensic science (V.B.). Three comparative methods have been followed:
(1) Superimposition of initial and late digital models to evaluate the stability of palatal rugae based on length and shape of first, second and third rugae after death. For each individual, two digital scans have been obtained, initial (t0) and, when the corpse still available in the morgue, after 1 week (t1).
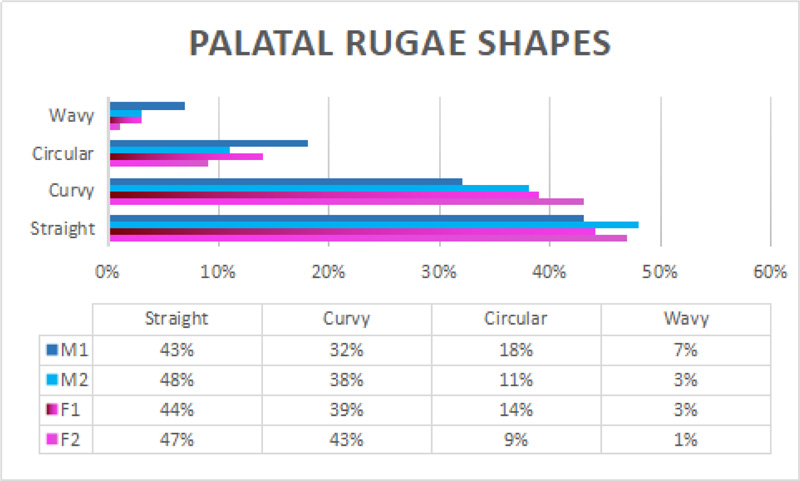
To compare the rugae length, the Lysell and Thomas and Kotze classification was followed (primary, secondary, fragmentary) for the first, second and third rugae. The rugae shapes have been compared too following the four major types (straight, curvy, circular and wavy). In the superimposition procedure, the initial and last digital scans have been differentiated, attributing two different colours (i.e., light grey and red; fuchsia and red; fuchsia and blue, etc.). Length and shape data have been recorded on both the right and left sides of the initial and final digital scan. Obtained results were subjected to statistical analysis.
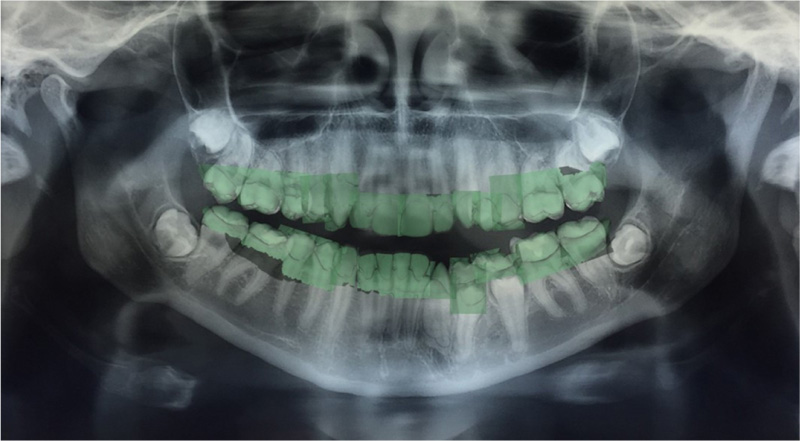
(2) Superimposition of digital models obtained by intraoral scanning and ortopantomographs (Fig. 6) as possible comparative method between ante-mortem and post-mortem records by the randomly distribution among the two observers for matching between initial or final random scan and radiograph.
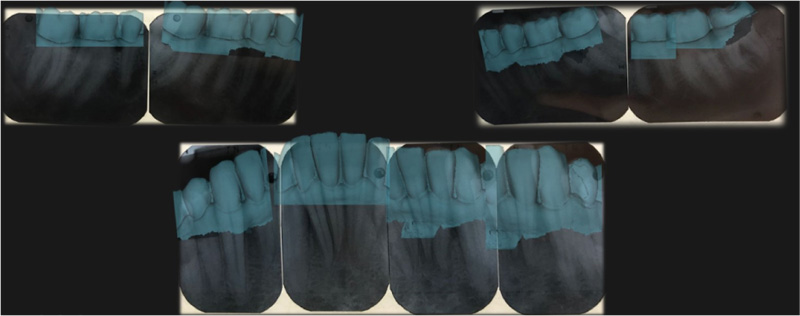
(3) Superimposition of digital models obtained by intraoral scanning and full mouth periapical films (Fig. 7) as possible comparative method between ante-mortem and post-mortem records ever by the randomly distribution among the two observers for matching between initial or final random scan and radiograph.
The last two superimpositions have been possible slicing digital models with a software called Slicer 3D® (Version 4.8), and the digital-radiographic superimposition has been obtained with the Geomagic® Control X Software (Version 2017.0.2).
The data obtained have been analysed statistically using the R Software (Version 3.5.1) and Excel Software (Microsoft Office 2016). The palatal rugae stability has been assessed by mean and deviation standard comparison with the t-Student test. The correctness of the match for each examiner was calculated as a percentage, the Χ-Square Test and the Χ-Square Test with Yates correction have been furtherly used to assess if the differences in the matching results were statistically significant or less. Both statistical methods have been chosen on the basis of previous researches in literature. To evaluate the accuracy of all the examinators’ observations, the Kappa test was performed and the score was ever 100, which indicates an agreement between observers. It has been considered a measurement error around 0.35-0.41 mm in the digital-radiographic comparison. The procedures followed in this study were in accordance with the Helsinki Declaration of 1975, as revised in 1983. Contrary to what is generally expected for human studies, this study did not, however, need to have the authorization of the Ethics Committee as the Italian law, in force at the time when this study was performed, allows the use of anonymous data collected on corpses subjected to necroscopy or judicial autopsies as long as they are limited to procedures that do not alter the body structure of the corpse itself (D.P.R. 285/190, artt.42-43; decr.leg.n.211). In the same way, consent for publication by subjects, living or deceased, according to the laws on the protection of privacy, is not necessary as the data were anonymized by the competent authorities before their collection (art.106 of Legislative Decree 196/2003).
3. RESULTS
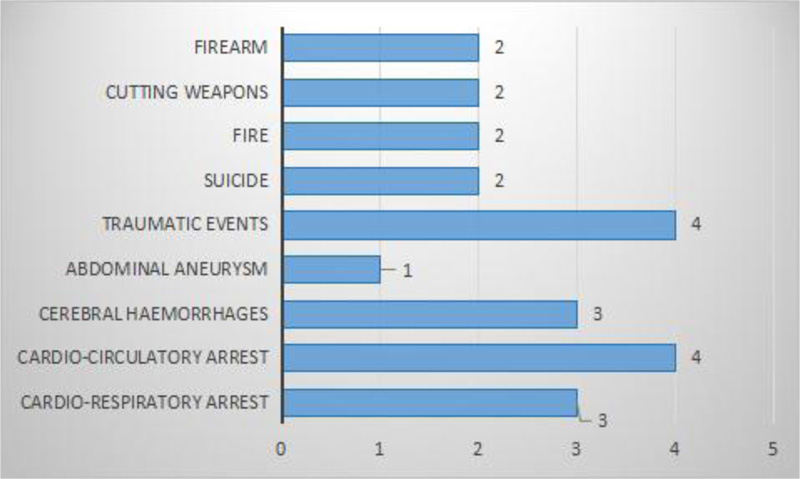
Due to the possible correlation with the presence of restorations and stability of palatal rugae analysed, the presence of conservative and prosthetic rehabilitations in the upper arch has been distinguished in anterior, lateral and posterior (from the first premolar to the second premolar). A part of the corpses had in their mouth at least one or more conservative restorations and one or more prosthetic rehabilitation at the same time. The presence of multiple prosthetic rehabilitations or the contemporary presence of prosthetic rehabilitations and conservative restorations was larger in the subjects over 45 years. The corpses delivered to the morgue had to carry out the necroscopic investigation. In many cases, the bodies had to undergo an autopsy for judicial reasons. The causes of death of the subjects indeed were a relevant matter (Fig. 8). In this study, no traditional impression materials have been used since the taking of impression was digital with the intraoral scanner and, at the morgue temperature of 16-18°C, intraoral scanner working is not influenced by that temperature. The manipulation and management of the access to the mouth of each cadaver had the support of the doctors specialized in forensic science present during the procedures (V.B., C.C., E.M.). The mean age is homogenous enough in both the genders (57.09 F; 58.46 M). It should be indicated for clarification that all the corpses observed did not need to be identified, and their age was therefore known. A large number of corpses had one or more prosthetic or conservative rehabilitation in the anterior, lateral and posterior (until second premolars) areas.
The palatal rugae analysis performed by the superimposition of digital scans led to the following results. Starting to analyse the data from the first intraoral scanner record on the first day of stay in the morgue until its last (for all the corpses, between the seventh and the eighth day) and the last digital scan, the stability of palatal rugae length has been evaluated with the t-Student test (Table 1). Since for P<0,05, a significant difference resulted between the initial length of palatal rugae and its last record, the same t-Student test has been used on the different gender and on the different subcategories of dental situation/rehabilitations to see if these two elements affected the stability. The gender does not affect the stability of palatal rugae after one week of death; they significatively change (reduction of length) in both sexes (Table 1). No differences were made between the first, second and third rugae to evaluate if one of these was more or less stable than others since the preliminary measurements of each of them showed superimposable average values.
| Sample of Cadavers | Initial Length | Last Length |
|---|---|---|
| N | 23 | 23 |
| Mean | 8,4733 | 8,2557 |
| SD | 0,1614 | 0,2768 |
| t | 3,2580 | - |
| df | 44 | - |
| P (significativity level) | 0,0022 | - |
| Female cadavers | Initial length | Last length |
| N | 12 | 12 |
| Mean | 8,4645 | 8,1975 |
| SD | 0,1263 | 0,2591 |
| t | 3,2091 | - |
| df | 22 | - |
| P (significativity level) | 0,0040 | - |
| Males cadavers | 1 | 2 |
| N | 11 | 11 |
| Mean | 8,4871 | 8,2427 |
| SD | 0,1988 | 0,2507 |
| t | 2,5334 | - |
| df | 20 | - |
| P (significativity level) | 0,0198 | - |
Further analysis for comparison with the t-Student test assessed the stability of palatal rugae after death based on the different dental situations. The absence of teeth influences the stability, such as the presence of prosthesis rehabilitations and combined conservative and prosthetic rehabilitation. The total absence of any kind of restorations and the presence of conservative restorations help to keep unaltered the palatal rugae pattern after death, but the number of corpses with the different listed dental features is extremely low to give a unique interpretation (Table 2). No significant differences based on dental situations were observed between the first, second and third rugae’s length, as already mentioned above. The last confrontation could have been based on the causes of death, but the numerosity of the many subcategories is not homogeneous and would not allow a statistically representative assessment of the relationship with the stability of the palatal rugae as it was possible for the comparison according to the belonging gender and the type of dentition (natural, absent, re-enabled prosthetically or with conservative restorations).
| Cadavers with Conservative Restorations | Initial Length | Last Length |
|---|---|---|
| N | 2 | 2 |
| Mean | 8,4050 | 8,0950 |
| SD | 0,0071 | 0,4172 |
| t | 1,0507 | - |
| df | 2 | - |
| P (significativity level) | 0,4036 | - |
| Cadavers with Conservative/Prosthetic restorations | Initial length | Last length |
| N | 5 | 5 |
| Mean | 8,5000 | 8,1340 |
| SD | 0,1356 | 0,2867 |
| t | 2,5805 | - |
| df | 8 | - |
| P (significativity level) | 0,0326 | - |
| Cadavers with prosthetic restorations | Initial length | Last length |
| N | 6 | 6 |
| Mean | 8,4600 | 8,1683 |
| SD | 0,1517 | 0,2743 |
| t | 2,2797 | - |
| df | 10 | - |
| P (significativity level) | 0,0458 | - |
| Cadavers with no rehabilitations | Initial length | Last length |
| N | 6 | 6 |
| Mean | 8,3800 | 8,1550 |
| SD | 0,1131 | 0,2192 |
| t | 1,2899 | - |
| df | 10 | - |
| P (significativity level) | 0,3261 | - |
| Edentolous cadavers | Initial length | Last length |
| N | 4 | 4 |
| Mean | 8,4675 | 8,2825 |
| SD | 0,1688 | 0,1948 |
| t | 2,4861 | - |
| Df | 6 | - |
| P (significativity level) | 0,0210 | - |
The stability of palatal rugae shape has been assessed by the digital matching of the first with the second scan (teeth have been cutted away digitally in order not to facilitate recognition based on dental characteristics). The selection of scan was on a random basis, the two observers (A.P. and V.B.) were not informed whether the scan belongs to the same individual, so each initial scan was matched with multiple second scans. A progressive simplification of wavy and circular rugae after one week is observed. There is no predominant gender and ruga (first, second and third) for this trend of change. The results of this comparative part of the study on the stability of rugal shapes showed that the straight and curvy shapes are more stable than the circular and wavy type (Fig. 9).
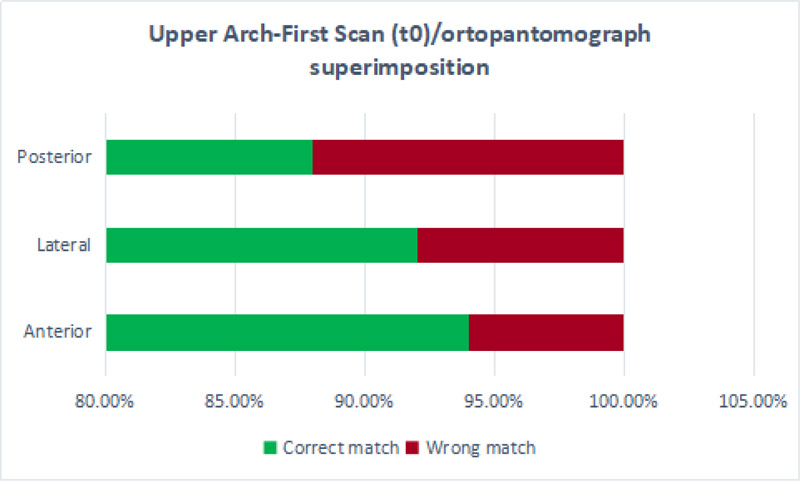
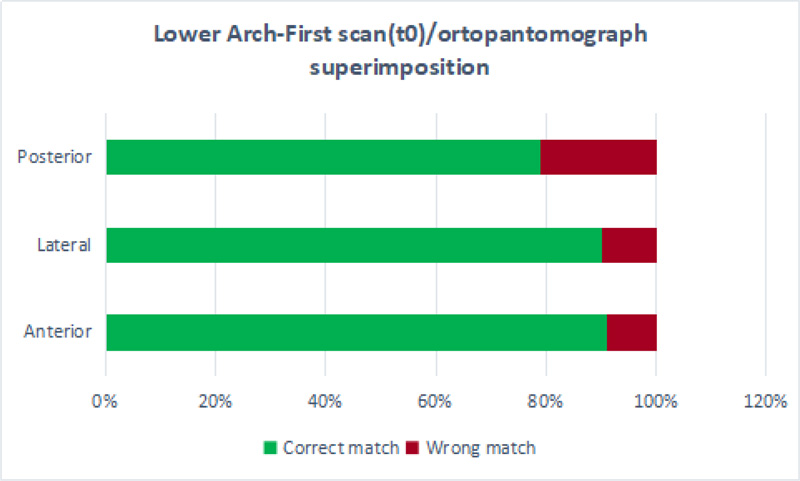
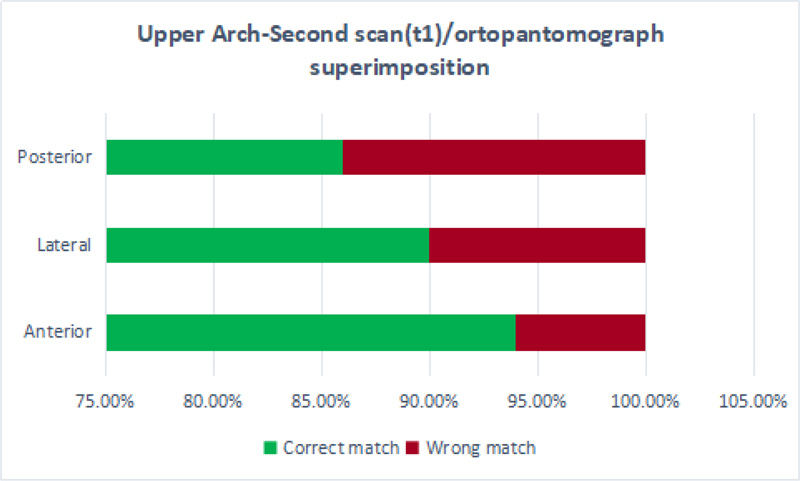
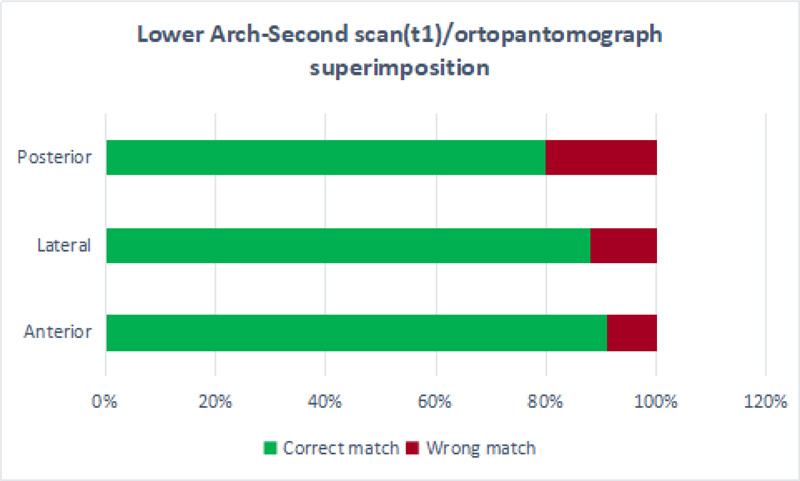
The possibility of overlapping in a useful way the scans with the radiographs available of the subject to contribute to the personal identification was carried out by matching the intra-oral scans cut with the Slicer 3D Software in three or multiple main sections corresponding to the anterior (incisors), lateral (canine and first premolar) and posterior (second premolar and teeth until the second or third molar, if present in the arch) areas of the arch and then overlapped to the radiographs with the automatic calibration tool selected by Geomagic® X control software. The overlays of the two scans, initial and final, at time t0 and t1, with the ante-mortem orthopantomographs (Figs. 10-13) have been performed. Only for two of the bodies, full-mouth periapical films have been found, so no statistical analysis has been performed even if the percentage of correct matching after the overlapping process exceeds in both the cases the 90% too and it is an encouraging result.
The results show that the overlap scan-ortopantomograph always exceeds 90% in the anterior sectors of both arches for both the detection time t0 and t1 (Figs. 10 and 11). The correctness of the overlays is lowered in particular in the posterior sectors (especially in the lower arch), at the time t1, and slightly in the lateral ones always at the time t1 probably for the quality of the scan which is sometimes more reduced in those areas where there is poor access.
To verify that the difference between the mean percentages is not due to the case but that it is a sign of a reliability of the digital-radiographic comparison, the data were analyzed by the Χ-square test (p<0,05) and the Χ-square test with Yates correction (Table 3). The non-significant differences between the t0 and t1 specific values of each sector demonstrate the potential reliability of this type of matching as a new comparative method for personal identification.
| C group t0-tl | X-Square test | p | X-Square test with Yates Correction | p | Odds Ratio | Significativity |
|---|---|---|---|---|---|---|
| Upper Anterior | 0 | 1 | 0,09 | 0,7659 | 1 | NS |
| Upper Lateral | 0,24 | 0,6212 | 0,06 | 0,8048 | 1,28 | NS |
| Upper Posterior | 0,18 | 0,6741 | 0,04 | 0,8335 | 1,l9 | NS |
| Lower Anterior | 0 | 1 | 0,06 | 0,8048 | 1 | NS |
| Lower Lateral | 0,2 | 0,6513 | 0,05 | 0,8212 | 1,23 | NS |
| Lower Posterior | 0,03 | 0,861 | 0 | 1 | 0,94 | NS |
4. DISCUSSION
Examining the currently available scientific literature up to the most recent contributions, however, emerges as compared to the advances in dentistry (and of orthodontics in particular) in the digital field [5, 6], except for a few research initiatives the forensic science, the forensic dentistry or odontology, has not put itself at the pace of the digital age and still remained branch that exploits methodologies of basic investigation. Forensic dentistry employs several identifying methods, some of which are of lesser impact and whose reliability is still being debated in the scientific community, such as cheiloscopy [7-9] and bite marks [10-12], which have a smaller scope but also the need to be supported by other elements as an instrument of evidence. Other methods, most of them, are of great interest and have a significant impact on the reality of human identification, sometimes constituting the elective method to perform identifying findings or medical-legal investigations [13-16]. The dental comparison between antemortem and possible post-mortem records for identification purposes occupies most of the forensic literature [17]. To look at most of the studies, they support the possibility of recognizing the identity of a subject through the comparison of his plaster models [18, 19] or dental radiographs [17, 20] with the data of the direct inspection on an unknown identity body. However, most of these methods do not provide for a real overlap of elements that might return a certain data, but are based on visual evidence sometimes supported by photographic documentation. Many Authors have then documented the specific potential of the study of palatal rugae, called rugoscopy or palatoscopy [21-28]. This exam is described as even more useful because the preservation of the palatine vault even in extreme environmental situations that deteriorate the body allows to perform an accurate investigation. In theory, this principle is correct, but apart from a study [28] on carbonized and non-carbonized corpses which is of a descriptive nature and is limited to the inspection of the oral cavity, all the other studies currently documented are mainly researches on plaster models of living subjects on which the observers want to determine the sex [23] or the racial characteristics [24, 29] or thanks to which is possible to verify the stability of the palatal rugae following orthodontic treatments (with the comparison of pre and post-treatment casts) to validate their use as a forensic marker [18, 19, 26, 27, 30-35]. The intrinsic limit of these studies is that the experimentation is carried out on plaster models and sometimes digital reproduction of the same and does not take into account the characteristics of the material of which they are made, which often presents superficial imperfections or defects or distortions (related to the impression from which they derive) that it is impossible to establish retrospectively with an external evaluation [18, 19, 27, 30-34]. Moreover, another element of which is not taken into account is the effect of the compression of the material by impression (alginate or silicone) on the mucous structures including palatal rugae which can therefore be altered already in the acquisition phase and therefore do not reflect the actual conformation of the palate of the subject. Obviously, the same can not be said for the dental elements that are properly reproduced but are still included in a dental cast that often in the storage stages may report injuries or fractures that disperse important details of the dental anatomy. To these aspects, one factor no less important should be added for a complete consideration. The traditional rugoscopic exam uses a pencil to highlight the palatal rugae pattern, including length and shape, and a manual calliper [19, 34-36]. These tools cannot compete with the current skills and technologies and they cannot anyhow allow a detailed and complete study of a complex and three-dimensional structure like the palate. Intra-oral scanners can no longer be considered a new technology in the dental workflow because they have been introduced in the daily practice many years ago, but their application in the forensic field, for the comparison of the dental data and for the rugoscopic examination, is extremely interesting and innovative. The use of the intraoral scanner to record a digital impression of the oral cavity of the corpse as it was done in this study, puts in front of perhaps more articulated considerations. Oral autopsy documented in the literature is described as a complex surgical method but sometimes necessary for a complete inspection of the body's mouth [3]. This practice is rather invasive and exposes elements of debate not only on the ethical level. The alteration of the integrity of the patient's face is evident, despite the accuracy of the procedure. The great limit of oral autopsy is that this alteration produces an irreversible modification of the relationships of the anatomical structures involved in the surgical dissection, as is the case for the general autopsy involving the other districts of the body, and may have consequences in judicial investigations. This study explored the possibility of performing a virtual autopsy of the corpse, without altering the integrity of its body and collecting as much information as possible that is not limited to a visual inspection but that allows to register the dental and mucous structures in a three-dimensional real-coloured file. Significative chromatic changes of oral mucosa can be monitored scan by scan, adding important information to the post-mortem decomposition process. The use of different tips that touch the surfaces without getting in contact with them and without compressing them allows to reach all the areas of the oral cavity even when, as happens in the living, the opening of the mouth can be rather limited. Among other things, the possibility to record also the occlusion allows to make a comparative examination also of this aspect.
In literature, there are not even studies that have investigated the possibility of using intraoral scans of living subjects or corpses for comparative radiographic studies. The possibility to “slice” the scans and to superimpose them with panoramic radiographs of the dental arches and full mouth periapical films has several advantages. First of all, it returns to two-dimensional examinations such as orthopantomography and full mouth periapical films the importance of being necessary examinations for identifying purposes that do not have, from this point of view, less validity of three-dimensional examinations such as CT Cone beam. The possibility to make a matching, with excellent results, of a three-dimensional file with a two-dimensional examination lead to understanding how it is not necessary to have a three-dimensional x-ray exam to reason in three-dimensional terms. So besides the advantage of knowing that the recovery of radiographs belonging to a subject can be of aid or real proof of identification, there is the advantage of knowing that the full mouth periapical film of a subject can be superimposed to an intraoral scan with the same purpose. In addition, the full mouth periapical film executed on corpse (element not of little importance considering that it is an examination that can be played without affecting the position of the body) or on human remains, can be used as a post-mortem record to be compared to antemortem records such as radiographs of the subject in life or intraoral scans.
CONCLUSION
Personal identification has always had a major role in many legal and administrative actions regarding both living and death beings. Nowadays, it has been invested in a new social and political interest. In forensic medicine, personal identification is attained through a process that evaluates different pieces of information. There is not a gold standard, and every approach to the issue has its advantages and flaws. The most common and easy approach is to compare recorded features with the ones noted during the identification process, but retrieving this type of information is often difficult and slow. On the one hand, the most reliable approach, DNA analysis is too expensive to be used in large scale, needs high-specialized personal and has an important privacy issue. On the other hand, one oral autopsy is an invasive method altering facial conservation, which could complicate visual recognition of remains by family members and other interested persons. This study has been set up to study and develop new, reliable, and fast methods of personal identification that can surpass many of the issues seen with the other techniques by a modern rugoscopy, a modern radiographic-digital comparison and virtual oral autopsy.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was conducted in compliance with applicable Italian laws on scientific research on cadavers. The use of corpses for the purpose of study and research is regulated by the Mortuary Police Regulations (D.P.R. 285/190, artt.42-43). The inspection of the corpse for scientific purposes, without its alteration and violation of its integrity (otherwise punishable by the Italian Penal Code according to article 143), could prejudice the necessary judicial investigations, does not need to be authorized by the Ethics Committee provided that data have been previously anonymized by the medico-legal operators responsible for the morgue or by the competent authorities. This is in accordance with the current Regulation of the Ethics Committee of the Higher Institute of Health (Istituto Superiore di Sanità, Rome 12th May 2015).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article are available on a reasoned request to be assessed on a case-by-case basis since this is material that can be partially reserved for judicial activities.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

