All published articles of this journal are available on ScienceDirect.

The Influence of Dental Occlusion on Spectrophotometric Tooth Color Determinations
Authors Info & Affiliations
Abstract
Background:
Shade matching is a significant treatment step and a challenge for the clinical team with potentially high costs for color correction. Currently, in the United States, the majority of private dental practitioners use visual color matching, but a recent study has reported a high rate of mistakes of subjective color determination among graduate dentists.
Objective:
The aim of this retrospective study is to analyze whether a change in the oral background due to dental occlusion can influence tooth color determination.
Methods:
Volunteer dental students underwent spectrophotometric color assessment using the SpectroShade device. Two measurements were carried out (with the individuals’ occlusion closed and with the occlusion open) on 43 upper central and 58 lateral incisors. Association between colorimetric variables L*, a*, b* and ΔE00 and tooth width, length and tobacco usage were examined.
Results:
Slight changes in the CIELAB values between closed and open occlusions were found for both the gingival and the central sections as for the overall tooth area, with mean ΔL*=-1.24, Δa*=-1.77, Δb*=-1.42 and ΔE00=1,84. A larger difference was detected in the incisal area, with mean ΔL*=-2.99, Δa*=-1.76, Δb*=-2.83 and ΔE00=3.65.
Conclusion:
In conclusion, our study showed that dental occlusion does not play a significant role in tooth color matching determinations, even though attention to avoid overbite due to a maximum intercuspation should be made.
1. INTRODUCTION
Shade matching is a significant treatment step and a challenge for the clinical team with potentially high costs for color correction. Currently, in the United States the majority of private dental practitioners use visual color matching, but a recent study has reported a high rate of mistakes of subjective color determination among graduate dentists, with an average error of CIELAB ΔE = 2.92 as determined by the Vita 3D-Master shade guide [1]. Spectrophotometric methods have been developed to increase the effectiveness of esthetic restorative work and customer satisfaction and are considered by some to be the gold standard for in vivo color matching determination [2, 3].
However, guidelines to ensure their reproducibility under different intraoral conditions are insufficient. Indeed, neither the instructions for these devices nor the accompanying brochures refer to the environmental conditions required at the point of measurement [4]. Recent efforts have been made to overcome this latter limitation and to clearly understand all the variables of these procedures. A recent in vivo spectrophotometric study (42 dental students) concluded that the position of the tongue did not impact measurement accuracy, finding only slight changes in CIELABvalues between the measurements. However, ΔE assessment was not included in the evaluation [5]. The spectrophotometric methodology is based on mathematical and statistical calculations, that are evaluated by an aesthetic quantitative approach, based on human eye perception thresholds. A difference in color with a ΔE lower than 1.1 (Perceptibility Threshold) cannot be detected by the human eye, while a ΔE between 1.1 and 3.3 can be detected but is still considered clinically acceptable, and a ΔE higher than 3.3 (Acceptability Threshold) can always be detected and considered as clinically not acceptable.
Documentation that the background can influence in vivo spectrophotometric color assessment exists, but the results are still controversial [6-10]. Lack of uniformity amongst authors showed different clinical impacts of the background on spectrophotometric color assessment: does not influence [6], may influence [7], or can severely influence [8-10] tooth color measurement. Furthermore, various grey [11], white [12, 13] or black [8, 14] backgrounds have been proposed and used with the intention of simulating the natural intra-oral conditions with currently no agreement or standardization.The present study aimed at analyzing the influence of dental occlusion on tooth colordetermination in a large cohort of volunteer dental students.
2. MATERIALS AND METHODS
2.1. Study Design
All volunteer dental students who, between September and December 2019 underwent spectrophotometric color assessment using the study device (SpectroShade, MICRO, Serial N HDL1407, MHT, Arbizzano di Negrar, Verona, Italy) at the First Dental Unit of the Sapienza University Hospital (Rome, Italy), were retrospectively retrieved from our institution database. All individuals who had sound upper right permanent central and lateral incisors, shade A1, A2, A3 assessed by spectrophotometric 3D Master Vita Scale, no bleaching treatment in the 6 months before measurements, no conservative restorations, no extrinsic stains, and no evident vertical tooth wear, overjet (OVJ)= 2-4 mm, overbite (OVB)= 2-4 mm were included in the present study.
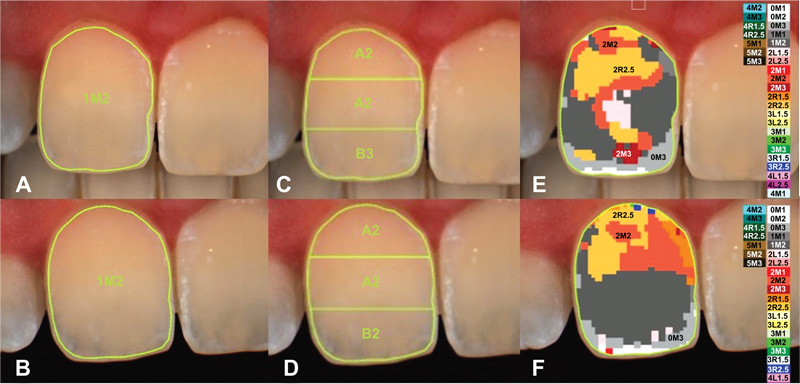
The protocol was approved by the local institutional ethics committee (approval n.4280) and informed consent was obtained from all individuals. All the procedures were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Spectrophotometric technical functioning and operative procedures were conducted as described in a previous study [15]. In the first measurement, the individuals’ dental occlusion was closed (Fig. 1). In the second measurement, the individuals’ dental occlusion was open with no contact between teeth of the opposite arches (Fig. 2). The two measurements were each performed on 103 upper central and lateral incisors (central: 45, lateral: 58). The stored data were used to retrieve CIELAB color data for the teeth [16]. Recall that CIELAB values consist of the L* value which measures the lightness ranging from 0 (black) to 100 (white), the a* value which measures redness/greenness, and the b* value which measures yellowness/blueness. Color differences (for example, ΔL = L*open – L*closed) between open and closed dentition for each tooth were defined by the CIEDE2000 color difference equation, known as ΔE00, which is perceptually uniform than the olderCIELAB system [2, 17]. The onboard MHT software divides the vestibular tooth area into three equalzones along the median axis (gingival, central and incisal area) so that the three areas of the teeth could be analyzed separately. All enrolled individuals had undertaken a clinical examination of the oral cavity carried out by a dentist to record data of the overbite, overjet and to assess tooth length and width by means of a digital calibrated caliper. Data on actual tobacco usage were also recorded.


2.2. STATISTICAL METHODS
Statistical analyses were employed to compare the study results using a software program (SPSS Version 10, SPSS Inc., Chicago, USA). First, simple descriptive statistics were obtained to determine the colorimetric variation of L*, a*, b* and ΔE00 between closed and open occlusion Only variates that were significantly correlated were chosen to be analyzed in the following steps. The association between L*, a*, b* and ΔE00OC and tooth length and width as well as tobacco usage were examined using a linear mixed effects regression analysis based on the spectrophotometric data and the clinical visit dataset. 95% confidence intervals (95% CI) were calculated and p-values < 0.05 were considered to be statistically significant (Fig. 3).
The assessments of a change in the oral background due to dental occlusion can influence tooth color determination is measured from teeth which are grouped within different patients. These data are regarded as hierarchical/multilevel, with teeth referred to as the level 1 units and patients the level 2 units. One important consequence of considering hierarchical data is that measurement on teeth within a patient is more similar than measurements on teeth in different patients. Linear mixed models account for the intra-patient correlation; failure to do so can result in misleading inferences.
3. RESULTS
3.1. Color Determination
Ninety-three consecutive volunteer dental students (36 males and 57 females; mean age of 24.47 years, ±1.96 SD years; range 20-33) fulfilled the entry criteria and were enrolled into the study.
Therefore, a total of 186 (93 teeth x 2) ΔE00, ΔL*, Δa*, Δb*, and a total of 558 (93 teeth x 3 tooth sections x 2) ΔE00, ΔL*, Δa*, Δb* accounting for overall tooth surface and for the three tooth sections, at open and closed occlusion assessments, were respectively evaluated.
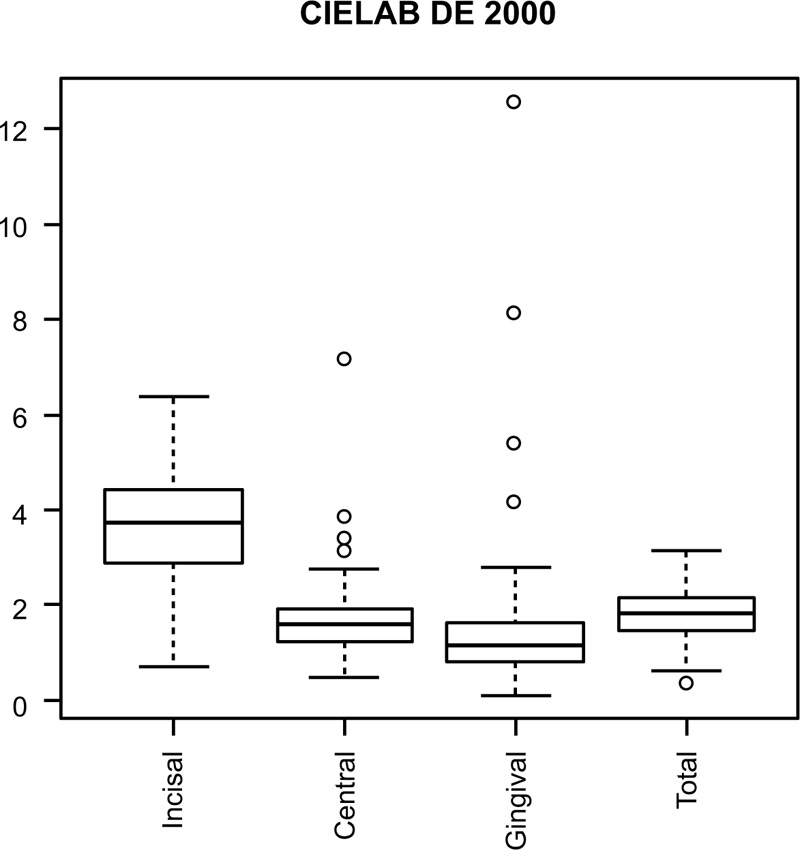
Descriptive statistics show slight changes in the CIELAB values both for the gingival and the central sections as compared to the overall area, with a mean ΔL*=-1.24, Δa*=-1.77, Δb*=-1.42 and ΔE00=1.84. The incisal area revealed larger differences between the two measurements, with mean ΔL*=-2.99, Δa*=-1.76, Δb*=-2.83 and ΔE00=3.65 (Table 1). A T-test was performed to evaluate the alternative hypothesis that the true mean is not equal to 0. The ΔL*, Δa*, Δb* and ΔE00 values were evaluated. The results show that only ΔL* and Δb* for the gingival section presented with a p value of 0.376 and 0.775, and a 95% CI of [-0.499 – 0.19] and [-0.766 – 0.572], respectively.
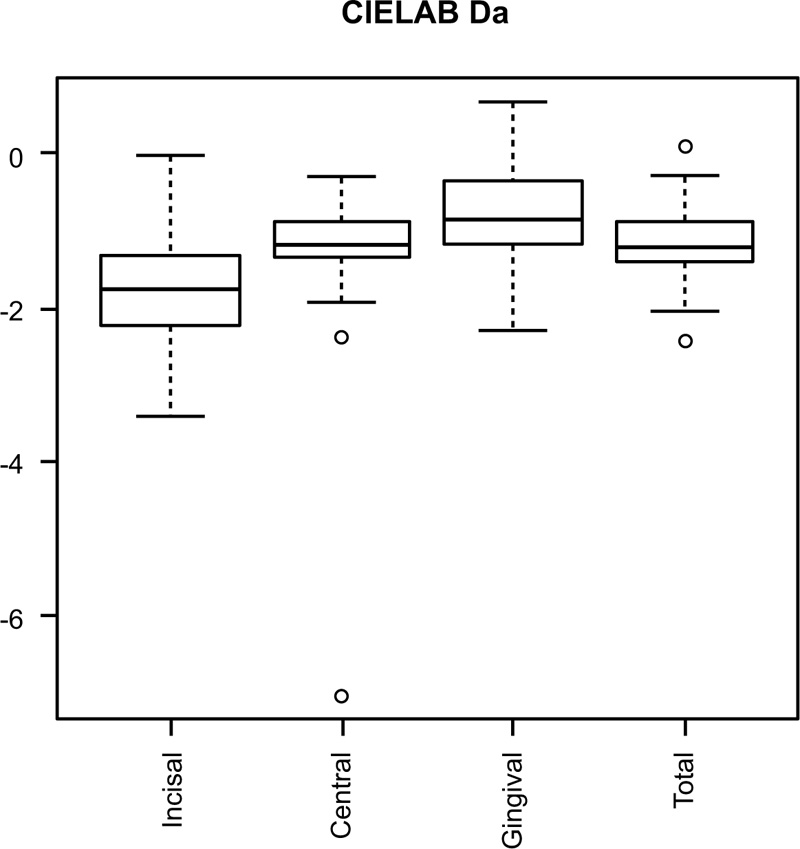
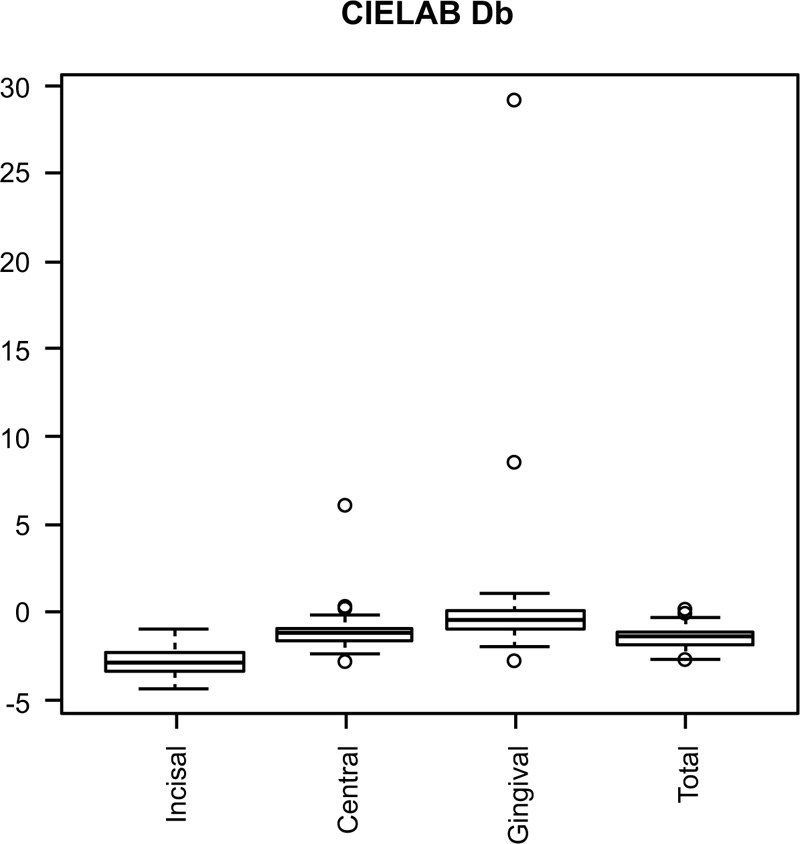
Boxplots of the ΔL*, Δa*, Δb* and ΔE00 values for incisal, central, gingival and overall tooth area are shown in (Fig. 4-7). Differences in the mean values of both groups were not great enough to reject the possibility that the difference was due to random sampling variability.
| Dimension | Mean | Median | Minimum | Maximum | p value |
| Incisal | |||||
| ΔL* | -2,98 | -3,2 | -5,45 | 8,48 | <0.001<0.001 |
| Δa* | -1,76 | -1,75 | -3,4 | -0,02 | <0.001 |
| Δb* | -2,84 | -2,9 | -4,4 | -0,94 | <0.001 |
| dE | 3,65 | 3,77 | 0,76 | 6,4 | <0.001 |
| Central | |||||
| ΔL* | -0,95 | -1,04 | -2,3 | 4,78 | <0.001 |
| Δa* | -1,19 | -1,18 | -7,03 | -0,31 | <0.001 |
| Δb* | -1,15 | -1,19 | -2,9 | 6,11 | <0.001 |
| dE | 1,74 | 1,65 | 0,51 | 7,2 | <0.001 |
| Gingival | |||||
| ΔL* | -0,15 | -0,4 | -2,34 | 10,83 | 0,376 |
| Δa* | -0,77 | -0,86 | -2,3 | 0,67 | <0.001 |
| Δb* | -0,96 | -0,47 | -2,83 | 29,13 | 0,775 |
| dE | 1,49 | 1,18 | 0,16 | 12,58 | <0.001 |
| Overall | |||||
| ΔL* | -1,01 | -1,34 | -2,63 | 4,2 | <0.001 |
| Δa* | -1,17 | -1,21 | -2,46 | 0,1 | <0.001 |
| Δb* | -1,42 | -1,42 | -2,72 | 0,21 | <0.001 |
| dE | 1,84 | 1,85 | 0,41 | 3,18 | <0.001 |

| Dependent Variables | ||||||||||||||||
| Independent Variables | Intercept | Age | Smoking | Central Incisor | Lenght | Width | Central Incisor x Lenght | Central Incisor x Width | ||||||||
| Estimate | P value | Estimate | P value | Estimate | P value | Estimate | P value | Estimate | P value | Estimate | P value | Estimate | P value | Estimate | P value | |
| dL central | -0.153 | 0.937 | -0.012 | 0.778 | 1.089 | 0.003 | -2.880 | 0.183 | -0.013 | 0.930 | -0.094 | 0.644 | 0,205 | 0.201 | 0,122 | 0.640 |
| dL overall | -0.371 | 0.845 | -0.006 | 0.873 | 0.904 | 0.012 | -2.653 | 0.215 | -0.016 | 0.910 | -0.116 | 0.561 | 0,185 | 0.243 | 0,124 | 0.628 |
| da* incisal | -0.729 | 0.624 | -0.032 | 0.231 | 0.159 | 0.501 | -2.885 | 0.134 | 0.300 | 0.010 | -0.431 | 0.013 | -0,089 | 0.0532 | 0,473 | 0.038 |
| da* overall | -0.933 | 0.289 | -0.017 | 0.274 | 0.112 | 0.412 | -2.191 | 0.058 | 0.180 | 0.009 | -0.220 | 0.032 | -0,03 | 0.724 | 0,316 | 0.021 |
| dE incisal | 6.029 | 0.028 | -0.027 | 0.558 | -0.371 | 0.360 | 2.622 | 0.485 | -0.293 | 0.176 | 0.311 | 0.346 | -0,097 | 0.730 | -0,199 | 0.654 |
3.2. Stastistical Analysis
A linear mixed effects regression analysis was employed to estimate possible relationships between ΔL*, Δa*, Δb* and ΔE00 and tooth length and width and tobacco usage. The ΔL* for the central tooth area showed a statistically significant correlation with tobacco (p = 0.003), which means that individuals who smoked showed a bigger difference in L* value when comparing open and closed occlusion. A similar correlation was shown for ΔL* value in overall crown measurements (p = 0.012).
In addition, the Δa* showed correlation with tooth width (p = 0.013) and length (p = 0.01) for both the incisal tooth section and the overall tooth area (tooth width p = 0.032; tooth length p = 0.009).
These results indicated that tooth length in both cases is directly related to Δa*. On the other hand, tooth width for the overall area stood in direct correlation with Δa*, but when taking into account only the incisal tooth section there was an inverse proportion of the tooth width to the Δa*.
4. DISCUSSION
We performed a study to compare two intraoral methods of measurement of the frontal upper teeth with a spectrophotometer. One measurement was made at the labial surface with teeth being in maximum intercuspation occlusal contact, while the second one was made with the mouth completely open without any contact between the lingual of the incisor surfaces. Slight changes in the CIELAB values both for the gingival and central sections as well as for the overall tooth area were observed, but none of these were statistically significant. Spectrophotometry is the gold standard for color measurement and communication. The usage of electronic devices on routine basis in dental practice enhances the communication of color to the dental technician. Although in dental practice the subjective evaluation is a frequently used method, it does also present a very high rate of mistakes. In fact, in vivo color matching is highly dependent upon the environmental lighting conditions and the subjective operator’s perception and experience. On the other hand, intraoral factors such as saliva, tooth dehydration, tongue position, surrounding colors, the chameleon effect of surrounding restorations, surface condition of the tooth being assessed, are all to be considered when performing color matching [4]. It has been reported that upper incisors show no color homogeneity and, in moving along the median axis from the incisal area toward the cervical one, the different optical characteristics of enamel and dentin cause a not uniform shade of the tooth [18]. It is also well known that different and not standardized backgrounds, such as grey, black, green and white affect color matching both in vivo and in vitro [9, 10]. Tooth color matching is one of the most important step in aesthetic rehabilitation not only for the professionals who want to select the correct tooth shade for aesthetic restorations, but especially for patients who wish to enhance their smiles [19]. Failure in tooth color matching is the most important reason for the patient’s dissatisfaction. Indeed, it has been reported that17.9 to 21.3% of UK adults and 34% of USA adults are dissatisfied with their tooth color after treatment [20, 21].The use of intraoral devices can minimize errors and the influences by the operator or the external factors, thus maximizing the reproducibility of color measurement. A recent in vivo study suggested that when using a spectrophotometer neither the users nor the intraoral environmental conditions influence the accuracy of the measurements [4].
No previous data are reported in Literature on in vivo studies aiming to test the influence of occlusion on tooth color determinants. A recent study by Ardu et al. evaluated the influence of different backgrounds on spectrophotometric color values of natural teeth. Twenty volunteers were subjected to 4 spectrophotometric measurements with alternatively a black, grey, white or no background (positive control). The authors demonstrated that background has an influence on color measurements and that black and grey backgrounds better simulate intra-oral environment that was represented by the positive control [21-24].
In our study, we found that the performance of the spectrophotometer in assessing color matching were not different if the measurement was done with the teeth occluded or open, as demonstrated by the slight changes in the CIELAB values for both the gingival and central sections, as well as, for the overall tooth area. Moreover, boxplots of the ΔL*, Δa*, Δb* and ΔE00OC values for incisal, central, gingival and overall tooth area confirmed that there was no significant effect of whether the teeth were occluded or open. A difference was noted in the incisal section, where a greater ΔE00 was found between the two methods, allowing the conclusions that both subjective and objective in vivo color matching can be influenced by the overbite due to a maximum intercuspation. Correlations between colorimetric variation and tooth width, length and tobacco usage were found according to the linear mixed effects regression analysis (Table 2). In particular, ΔL* was found to be closely related to tobacco usage in the central tooth area and the overall crown measurements. Similarly, Δa* showed correlation with tooth width and length both for the incisal tooth section and the overall tooth area. On the other hand, tooth width for the overall area stood in direct correlation with Δa*, but when taking into account only the incisal tooth section there was an inverse proportion of the tooth width to the Δa*.
The clinical significance of these results is: (i) The acquired pellicle on the enamel surface in tobacco users may have an impact on color measurements despite all the individuals were strictly selected and presented A1, A2 and A3 Vita 3D;(ii) The need to have a greater caution in assessing color in central incisors than in lateral, especially when an aesthetic rehabilitation is required in a patient presenting predominant upper central incisors; (iii) The a* colorimetric variable in the CIELAB color space can be influenced by tooth length more with the closed dental occlusion than the open.
The clinical applications based on the results of this study can be introduced into the daily dental activity when color matching procedures are carried out. When color matching is being done for esthetic rehabilitation, care must be taken to ensure that the patient keeps his mouth open and teeth separated, and to pay particular attention to smoking patients to remove the acquired pellicle before the procedure. The conclusion of this study are of paramount importance to those who work daily on esthetic rehabilitation of the upper arch, frontal segment, and want to achieve the best quality results in terms of biomimetic dentistry.
CONCLUSION
In conclusion, our study showed that dental occlusion does not play a significant role in overall toothcolor matching determinations, even though attention should be paid when performing color matching in esthetic rehabilitation due to the effect of the occlusion on tooth color determinants within the incisal section. This aspect can be further exacerbated in tobacco users and dental operators should consider this aspect. Further research is needed to straighten the clinical recommendation in spectrophotometric usage with different background settings.
AUTHORS' CONTRIBUTIONS
MM: conceptualization; SW and MJ: writing; AM: data management; LO: data curation; GMN and FG: supervision.
LIST OF ABBREVIATIONS
| OVJ | = = Overjet |
| OVB | = = Overbite |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the ethical committee of the Department of Oral and Maxillofacial Sciences, Sapienza University of Rome, Italy with approval no.4280.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
All patients participated on a voluntary basis and gave their informed consent.
STANDARDS FOR REPORTING
CONSORT guidelines and methodology were followed.
AVAILABILITY OF DATA & MATERIALS
Not applicable.
FUNDING
None.
CONFLICTS OF INTEREST
The authors declare that they have no conflict of interest.
ACKNOWLEDGEMENTS
Declare none.

