All published articles of this journal are available on ScienceDirect.

Curing Depth and Degree of Conversion of Five Bulk-Fill Composite Resins Compared to a Conventional Composite
Authors Info & Affiliations
Abstract
Background:
Limited curing depth and its effect on the degree of conversion are among the challenges of working with light-cure composite resins. The use of bulk-fill composites is one strategy to overcome these limitations.
Methods:
Ever X Posterior (EXP), Filtek Bulk-Fill Posterior (FBP), Sonic Fill 2 (SF2), Tetric N-Ceram Bulk-Fill (TNB), and X-tra Fil (XF) bulk-fill and Filtek Z250 conventional composite were evaluated in this in vitro experimental study. Six samples for the assessment of microhardness and three samples for the evaluation of DC were fabricated of each composite. After light curing and polishing, the samples were incubated at 37°C for 24 hours. Microhardness was measured by a Vickers hardness tester three times and the mean value was calculated. DC of the top and bottom surfaces was determined using Fourier-Transform Infrared Spectroscopy (FTIR). Data were analyzed using one-way ANOVA and Tukey’s test.
Results:
Microhardness and DC were significantly different among the groups (P<0.001). XF and Z250 equally showed the highest bottom-to-top surface microhardness ratio (0.97 ± 0.01) and significantly higher DC in the top (P<0.001) and bottom (P<0.005) surfaces compared to other groups. TNB showed the lowest microhardness ratio (0.88 ± 0.04) and DC (68.66 ± 1.52 and 61.00 ± 2.00); the difference in DC of the bottom surface was statistically significant (P<0.003).
Conclusion:
It appears that bulk-fill composites evaluated in this study are adequately polymerized at 4 mm depth. Their DC was optimal and within the range of conventional composites.
1. INTRODUCTION
The application of composite resins has greatly increased due to their optimal physical, mechanical, and esthetic properties. However, they still have drawbacks that limit their application [1]. Limited curing depth and the risk of insufficient conversion of monomer to polymer in deep areas are among the shortcomings of light-polymerizing composite resins [1, 2]. In other words, light-cure composite resins can be polymerized only to a certain depth, which depends on the penetration of visible light through the composite mass. The energy of light radiated by the light-curing unit is gradually attenuated as it passes through the composite mass. As a result, a gradual reduction in Degree of Conversion (DC) of composite resin monomer occurs as the distance from the irradiated surface increases. Reduction in DC compromises the physical properties of the composite and enhances the release of monomers, which eventually leads to early restoration failure or may negatively affect the pulp tissue [3].
The term “hardness” is used to predict the wear resistance and the wearability of materials by the opposing tooth structure. The bottom to top surface microhardness ratio should meet the minimum acceptable value of 0.80 or 0.85 to ensure that the bottom surface is adequately polymerized [4]. Factors affecting the curing depth include the type of composite resin, its color and translucency, thickness of each increment, distance from the tip of the light-curing unit to the composite surface, and size and distribution of filler particles [2, 5]. Polymerization of composite resins includes conversion of carbon double bonds to carbon single bonds which determine the DC. Factors such as the size of filler particles, polymer matrix, the radiating light, its intensity, wavelength, and duration of radiation, the size of tip of device, type and amount of photo-initiators, and color of composite resins can all affect the DC and subsequently the mechanical properties, wear resistance, and color stability of composite resins [4, 6].
To overcome the aforementioned drawbacks of the conventional composite resins, bulk-fill composites were developed, which can be applied in the cavity as bulk in up to 4 mm thickness, requiring one single curing cycle, with no adverse effect on their adaptation or DC [6, 7]. Bulk-fill composites have unique properties, which ensure adequate curing of the bulk mass even in deep areas. The manufacturers of bulk-fill composites claim that they are superior to conventional composites in many aspects; however, some controversies still exist in this respect. For instance, the DC of >55% is clinically acceptable for bulk-fill composites but this value is still lower than the DC of conventional composites [8]. Considering such controversies and the gap of information regarding the DC and curing depth of different bulk-fill composites available in the market, this study aimed to assess and compare the curing depth and DC of five commonly used bulk-fill composites in comparison to a commonly used conventional composite resin. The null hypothesis was that the curing depth of bulk-fill composites is similar to conventional ones (2 mm) and DC of bulk-fill composites in deep layers is lower than conventional resins.
2. MATERIALS AND METHODS
This in vitro, experimental study was performed on composite samples fabricated of five bulk-fill composites namely Ever X Posterior (EXP), Filtek Bulk-Fill Posterior (FBP), Sonic-Fill 2 (SF2), Tetric-N-Ceram Bulk-Fill (TNB), and X-tra fil (XF) and one conventional composite namely Filtek Z250 (as control) using a mold. Sample size for the assessment of microhardness was calculated to be six samples in each of the six groups by means of One Way ANOVA Power Analysis of PASSII software and in accordance to a study by Moharam et al. [9], and considering an investigation by Abed et al. [6] and by means of One Way ANOVA Power Analysis of PASSII software the sample size for assessment of DC was calculated to be three samples in each of the six groups.
2.1. Sample Preparation
Table 1 shows the characteristics of the five bulk-fill and one conventional composite (control) used in this study. A two-piece stainless steel mold measuring 4.1 x 4.1 x 4.1 mm was used and the bulk-fill composites were packed in the mold as bulk with 4 mm thickness. After packing, a glass slab measuring 1x25x75 mm was placed over it and light-curing was performed for 30 seconds using a poly-wave LED light-curing unit (BluePhase N, Ivoclar Vivadent AG, Schaan, Liechtenstein) with 385-515 nm wavelength and 1200 mW/cm2 light intensity periodically checked by a radiometer (Model 100; Optilux, SDS, Kerr, Orange, CA, USA). The tip of the light-curing unit was in direct contact with the glass slab during curing in order to standardize the distance from the tip to the surface of samples during polymerization. In the control group, Filtek Z250 conventional composite was applied in to the mold measuring 2.1x2.1x2.1 mm and was light-cured from the superior surface. After removing the samples from the mold, their lateral surfaces were marked to differentiate the top and bottom surfaces. Next, the top and bottom surfaces were polished with 800, 1000, and 1200-grit abrasive papers, respectively, to obtain a smooth surface. After polishing, the dimensions of all samples were measured by a digital caliper to the nearest 0.01 mm (Mitutoyo, Tokyo, Japan). They were then incubated in a dry environment at 37°C for 24 hours. Three samples in each group were fabricated in the same manner described above for the assessment of DC.
| Code | Commercial Brand | Type of Composite | Manufacturer | Composition | Filler Percentage | Color |
|---|---|---|---|---|---|---|
| 1 | EverX Posterior (EXP) | Short fiber composite | GC Corp., Tokyo, Japan | Short E-glass fiber filler, barium glass, Bis-GMA, PMMA, TEGDMA | 74.2wt% 53.6vol% | Universal |
| 2 | Filtek Bulk Fill Posterior(FBP) | Nano fill | 3M ESPE, St. Paul, MN, USA | Non- agglomerated/non-aggregated 20 nm silica filler,non-agglomerated/non-aggregated 4 to 11 nm zirconia filler,aggregated zirconia/silica cluster filler,ytterbium trifluoride filler consisting of agglomerate 100 nm particles,ERGP-DMA,diurethane-DMA,1, 12-dodecane-DMA | 76.5wt%58.4vol% | A2 |
| 3 | Sonic Fill 2(SF2) | Nano Hybrid | Kerr corp., Orange, CA, USA | Poly(oxy-1,2-ethanediyl), α,α′-[(1-methylethylidene)di-4, 1-phenylene]bis[ω-[(2- methyl-1-oxo-2-propen-1-yl)oxy]-Not available. 2,2′-ethylenedioxydiethyl dimethacrylate. |
81.3wt% unreported. | A2 |
| 4 | Tetric N-Ceram Bulk Fill(TNB) | Hybrid | Ivoclar Vivadent AG, Schaan, Liechtenstein | Barium glass,Prepolymer,Ytterbium trifluoride,Mixed oxideBis-GMA, DMA | 75-77wt%53-55vol% | IVA |
| 5 | X-tra fil(XF) | Hybrid | VOCO Cuxhaven, Germany | Barium-boron- aluminosilicate glass,Bis-GMA, UDMA, TEGDMA | 86wt%70.1vol% | Universal |
| 6 | Filtek Z250 Universal(Z250) | Micro Hybrid | 3M ESPE, St. Paul, MN, USA | zirconia/silica without silane treatment,Bis-GMA, UDMA, Bis-EMA |
82wt%60vol% | A2 |
2.2. Assessment of Curing Depth Using Vickers Micro Hardness Test
The fabricated samples were subjected to Vickers microhardness test (Bareiss, Germany) and their top and bottom surfaces were subjected to indentation by the indenter of the device applying 300 g load for 15 seconds such that the indenter applied load to each surface 3 times with at least 3 diagonal widths of 20 µm between indentations. The load application created a symmetrical indentation in each surface, the dimensions of which were determined under a microscope.
2.2.1. Measurement of DC
The DC was measured using Fourier-transform infrared spectroscopy (FTIR; Nicolet IS 10; USA). First, an uncured sample of each composite was subjected to FTIR. Following the passage of light through the sample, chemical double bonds were identified and the absorption peak was recorded at 1608-1638 cm-1. Next, three cured samples in each group were subjected to FTIR such that the absorption peaks were recorded once for the top and once for the bottom surface. The DC of the top and bottom surfaces was calculated using the formula below:
 |
2.2.2. Statistical Analysis
One-way ANOVA was used to compare the top and bottom surface microhardness, the ratio of the bottom to top surface microhardness and DC of the top and bottom surfaces. Pairwise comparisons were performed using Tukey’s HSD test. All statistical analyses were carried out using SPSS version 22 (SPSS Inc., IL, USA) at P<0.05 level of significance.
3. RESULTS
3.1. Results of Surface Micro Hardness
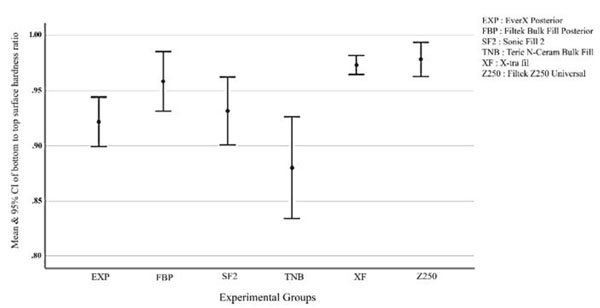
One-way ANOVA showed significant differences in the microhardness of the bottom (P=0.000) and top (P=0.000) surfaces and the bottom/top micro hardness ratio (P=0.000). In the assessment of microhardness of the top and bottom surfaces, Tukey’s test revealed that the microhardness of the XF group was significantly higher than that of other groups (P<0.001). The Z250 composite also showed significantly higher microhardness than other composite resins except for XF. SF2 showed significantly higher microhardness than TNB, EXP, and FBP (P<0.001). TNB showed significantly lower microhardness than other composite resins (P<0.001), and EXP and FBP were not significantly different in this regard (P>0.05). Analysis of the bottom/top surface microhardness ratio by post hoc Tukey’s test (Fig. 1) showed that Z250 had a significantly higher microhardness ratio than SF2, EXP, and TNB (P<0.047). XF showed a significantly higher microhardness ratio than EXP and TNB (P<0.022). Thus, XF and Z250 equally showed the highest microhardness ratio (0.97 ± 0.01) followed by FBP (0.95 ± 0.02). TNB showed the lowest ratio (0.88 ± 0.04).

3.2. Results of DC
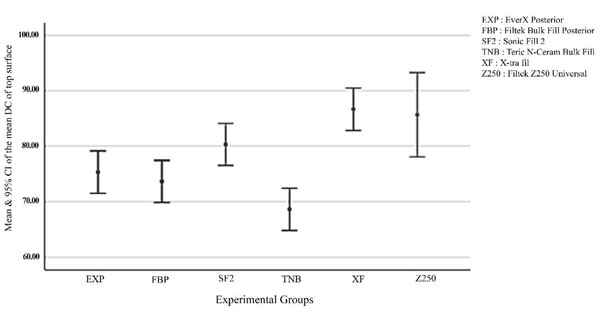
One-way ANOVA showed a significant difference among the composite resins in DC of the top (P=0.000) and bottom (P=0.000) surfaces. Pairwise comparisons by Tukey’s test (Fig. 2) showed that XF and Z250 had significantly higher DC in the top surface compared to other groups (P<0.001). SF2 showed significantly higher DC in the top surface than FBP and TNB (P=0.009), and TNB showed the lowest DC of the top surface (68.66 ± 1.52). Fig. (3) Compares the DC of the bottom surfaces. As shown, Z250 and XF had significantly higher DC of the bottom surface (P=0.005) and TNB had significantly lower DC of the bottom surface than other groups (P=0.003).
4. DISCUSSION
The null hypothesis of this study was rejected because the results showed that the bulk-fill composites tested were well polymerized at 4 mm depth and their DC was above the standard threshold of 55-65%. Several methods are available for the assessment of curing depth. Laser and FTIR are among the direct methods for the assessment of curing depth while microhardness test, scraping, and visual inspection are among the indirect methods applied for this purpose [10]. Since the optical microscopy and scraping methods, which are approved by the ISO 4049, overestimate the curing depth compared to the Vickers or Knoop hardness test [11], the Vickers’s hardness test was used to assess the curing depth in the present study. In the evaluation of curing depth, the ratio of the bottom to top surface microhardness for completely cured samples should be ideally 1; however, 80% curing depth is often regarded as clinically acceptable [2, 3, 12]. Our results showed that XF, Z250, and SF2 had the highest microhardness in both the top and bottom surfaces compared with other groups while TNB showed the lowest surface microhardness. The high microhardness reported for XF in our study was in agreement with other studies [9, 13]. Such a high hardness value can be due to the difference in the chemical composition of organic resin matrix and viscosity of monomers. Also, the flexibility of chemical structure can affect the curing depth of composite resins. The XF organic resin matrix is made of bis-GMA, UDMA, and TEGDMA; the latter is considered as the diluting monomer, which has the lowest viscosity and highest DC among the composite resin monomer systems. When Bis-GMA is diluted with low-viscosity monomer, it exerts a synergistic effect on DC and curing depth. Thus, high amounts of TEG DMA monomer can probably be the reason for the higher curing depth of the XF composite [9, 14]. In our study, Z250 conventional composite also showed high microhardness; this may be due to the composition of its matrix that contains glass, quartz, and ceramic particles as fillers, enhancing its microhardness [15, 16]. High microhardness of SF2 can be attributed to the heat generated during vibration since it can enhance polymerization by increasing the movement of free radicals (directly) and reduction of viscosity (indirectly). However, the effect of ultrasonic energy on the curing of resin has not yet been systematically evaluated [17]. Significantly lower microhardness of the top surface of TNB samples may be due to the initiator/catalyst system, type of monomer, and use of barium glass fillers along with pre-polymerized particles in the composition of this composite resin [14].
The parameters affecting microhardness include morphology and distribution of fillers, shape and density of particles, type and amount of monomer, and DC of monomer, which are highly variable among different composite types [18]. It has been found that the microhardness of the top surface of composite samples was less dependent on the intensity of radiated light because the top surface acquires the highest energy from the curing light [19]. In a study by Rodriguez et al. [20], similar to our study, the top surface of samples showed higher microhardness than the bottom surface; the hardness value decreased by an increase in thickness.
In the current study, XF and Z250 equally showed the highest curing depth (the bottom to top surface microhardness ratio was 97%) followed by FBP (the bottom to top surface microhardness ratio was 95%). In fact, the microhardness of FBP was less than that of SF2 but its curing depth was higher, which indicates that light transmission in FBP is better than in SF2 (the bottom to top surface microhardness ratio was 93%). Regarding the optimal curing depth of FBP at 4 mm thickness, the results of other studies were in line with ours [21, 22]. The fillers of this composite include a combination of non-agglomerated/non-aggregated silica fillers measuring 20 nm in diameter, non-agglomerated/non-aggregated zirconia fillers measuring 4-11 nm, aggregated zirconia/silica cluster fillers (20 nm silica and 4-11 nm zirconia particles), and yttrium tri-fluoride including 100 nm agglomerated particles. Such nanoparticles cannot scatter or absorb the visible light, which is important in their light-curing process [23]. TNB also showed the lowest curing depth; however, its curing depth was still over 80% (88%). It means that it is well cured at 4 mm depth. Similarly, Al-Mansour et al. [24] reported >80% hardness for TNB. This finding can be due to the presence of Ivocerin in its composition. Ivocerin, a germanium-based initiator, has higher photo-curing activity than camphorquinone and absorbs the visible light in a wide wavelength range of 380 to 460 nm; whereas, camphorquinone absorbs light in the range of 450 to 490 nm [25-27]. Moreover, this initiator can be used without the addition of amine as a co-initiator and produces at least 2 free radicals. Thus, it has higher efficacy than the camphorquinone-amine system, which only has one free radical [28]. On the other hand, other investigations [12, 14] revealed that the TNB composite, despite having high filler content, has lower than standard bottom to top surface microhardness ratio (80%), which was in contrast to our findings and this controversy in the results of the two studies can be due to the difference in type of light-curing unit used [12, 14]. We used the BluePhase N poly-wave LED light-curing unit by Ivoclar in this study. This device has been specifically designed to include blue and violet lights and due to having a wide range of wavelengths, it can be used for any material and initiator (385-515 nm). It has a light intensity of 1200 mW/cm2 according to the manufacturers’ instructions regarding using a light intensity higher than 1000 mW/cm2. Any small incompatibility between the wavelength of light source and sensitivity of the photo-initiator can limit the ability to maintain free radicals, which are responsible for the polymerization process [29]. The use of mono-wave LED for curing of bulk-fill composites that contain camphorquinone along with other photo-initiators with lower wavelength absorption decreases the DC [30].
The current results regarding the curing depth of EXP were in line with other studies [11, 31]. The use of short fibers as fillers in EXP does not seem to negatively affect the curing depth [14]. Its resin matrix composition includes bis-GMA, TEGDMA, and PMMA, which comprise a semi-interpenetrating polymer network that provides optimal bonding properties. Also, E-glass fibers enhance the toughness of the polymer matrix [32]. In fact, the random orientation of fibers and semi-interpenetrating polymer network structure of their polymer matrix probably play an important role in the improvement of the mechanical properties of EXP [21]. Interpenetrating polymer networks are composed of two or more polymers in one network that provide a relative heterogeneity in the molecular scale in the matrix. The polymers cannot be released unless the chemical bonds are broken [33]. Also, two photo-initiators namely camphorquinone and trimethyl benzoyl phosphine oxide (which enhances the general function of free radicals compared with camphorquinone) are used in its composition. It should be noted that EXP can be used for filling the entire cavity; however, according to the manufacturers, it should be preferably used with another veneering material to obtain an acceptable wear resistance. In other words, EXP is a non-flowable base composite with the highest mechanical properties and viscosity among the base materials and is comparable with non-base bulk-fill composites [34].
The use of novel resins, modulators, and fillers increased the curing depth of bulk-fill composites [14]. Also, the amount of light passed through the composite resin depends on the amount of reflected light, scattered light and absorbed light, which varies depending on the composition of the composite [35, 36]. Smaller fillers scatter light more than larger fillers [37]. Moreover, evidence shows that by an increase in the amount of filler, the translucency decreases due to an increased likelihood of light refraction at the filler-resin interface. The translucency increases by an increase in filler size [36]. Thus, size, radiopacity, translucency, and pigments of filler particles affect the passage of light through the material and curing depth [38]. However, nano-filled bulk-fill composites such as FBP and SF contain specific amounts of small fillers with dimensions smaller than the visible light wavelength (390 to 750 nm). Due to small size, these nanoparticles cannot scatter or absorb visible light, which can significantly affect the curing, translucency, and esthetics [23, 36]. In our study, only XF had higher microhardness of top and bottom surfaces compared with the control group (Z250). Regarding curing depth, XF and Z250 equally showed the highest curing depth.
DC is determined by the ratio of the frequency of residual C=C aliphatic double bonds in cured composite resin compared with the total number of C=C double bonds in uncured material [39]. FTIR is used to analyze DC in the polymerization of methacrylates [40-43]. There is no consensus regarding minimum DC required for most restorative materials but it is assumed that a minimum DC in the range of 55-65% is suitable for the occlusal layer [41].
Factors such as size and composition of fillers, translucency of materials, curing type, intensity of LED, curing time, composition of monomer, and concentration of photo-initiator can affect the DC of composite resins [44, 45]. Also, by an increase in filler content, DC relatively decreases, which can be attributed to the reduction in resin content and light scattering at the resin-filler interface [46].
In our study, XF and Z250 showed significantly higher DC in the top surface compared to other groups followed by SF2. Primary viscosity and flexibility of chemical structure are two important properties of monomers that affect the DC [47]. Higher DC of XF in our study may be due to the unique chemical composition of its organic matrix. The organic matrix of XF is composed of bis-GMA, UDMA, and TEGDMA. Evidence shows that the maximum DC of different monomer systems increases in the following order: bis-GMA<bis-EMA<UDMA<TEGDMA [48].
Bis-GMA is the most viscous monomer with minimal flexibility due to strong intramolecular hydrogen bonds of its hydroxyl (-OH) groups. UDMA is also a viscous monomer due to having intra-molecular hydrogen bonds between the amine (-NH-) and carbonyl (-C=O) groups. However, UDMA has much lower viscosity and higher flexibility than bis-GMA due to having weak hydrogen bonds of amine groups compared with hydroxyl groups [49]. However, the presence of amine groups in the structure of the urethane monomer of UDMA is responsible for reactions for the continuation of polymerization. These reactions increase the mobility of radicals and subsequently enhance the polymerization and DC [48].
The organic matrix of Z250 includes bis-GMA, bis-EMA, and UDMA. The latter has a higher content than the other two, which may explain the high DC of this composite [50]. Regarding SF, replacing bis-GMA with a low-viscosity ethoxylated analog (bis-EMA) along with the presence of flexible siloxane methacrylate copolymer may increase the molecular reactivity of monomers [34]. Moreover, the sonic vibration process during the application of material with a specific hand-piece may decrease the viscosity and increase the movement of monomers and subsequently their DC [17]. The findings of Goracci et al. [31] and Monterubbianesi [41] supported our results in this respect.
Assessment of DC of the bottom surface revealed that Z250 and XF had significantly highest DC compared to other groups. The lowest DC of both surfaces was noted in TNB. Although TNB contains a dibenzoyl germanium photo-initiator activated by light at 380-460 nm wavelength, it does not cause a higher DC or greater curing depth in this composite compared to others, which may be related to low penetration of light into the composite mass [51].
In bulk-fill composites, two strategies are employed to maintain high DC in deep areas. The first strategy is their increased translucency. For the highest light transfer, most bulk-fill composites are not available in different colors. Increased filler size and compatibility of the refractive index of filler and resin matrix are among the methods to increase the translucency of composite resins. In fact, minimizing the difference in the refractive index of filler and resin improves the DC, curing depth, and color match. The second strategy is to enhance the efficiency of the photo-initiator. Most of the currently available composite resins are based on the camphorquinone-amine system with a limited production of free radicals. To increase their function, they are combined with accessory photo-initiators including TPO derivatives such as Lucerin-TPOTM and Irgacure-819TM or benzoyl-germanium (IvocerinTM) compounds, which have synergistic effects on camphorquinone with simple photo-scission without amine reduction [51, 52].
Future studies are recommended to evaluate other properties of bulk-fill composite resins such as their wear resistance, fracture toughness, and effect of thickness on the passage of light.
CONCLUSION
Within the limitations of this study, the bulk-fill composites tested were well polymerized at 4 mm depth and their DC was above the standard threshold of 55-65%.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Ethics Committee of Tehran University of Medical Science, Tehran, Iran (Code #. IR.TUMS.DENTISTRY.REC.1397.003).
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in Tehran University of Medical Science, central library Tehran, Iran, no URL assigned to research projects but data is well protected.
FUNDING
This work was financially supported by the Dental Research Center, Dentistry Research Institute, Tehran University of Medical Sciences, Tehran, Iran (96-03-70-36890).
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

